8 Total Body Lift Surgery
Abstract
The timing and staging of body-contouring procedures after massive weight loss consider a host of variables relating to the nature of the patient, as well as the temperament and preparation of the plastic surgeon. With so many major deformities needing correction, there must be complex planning. Nevertheless, there is no consensus on the extent of surgery to be done during any given operative session. Total body lift (TBL) surgery was conceived in response to the desires of the majority of our patients, who request comprehensive surgery in as few stages as safely possible. Candidates for TBL are young (<age 50), healthy and physically fit, not obese (body mass index [BMI] <30 kilograms per height in meters squared [kg/m2]), and highly motivated. The optimal patient has lost all excess weight and is left with significant redundancy of skin that would be benefited by body lift surgery. At about 18 months after bariatric surgery and 3 months of stable weight, patients are prepared for their multiple operations by optimizing their medical condition and nutritional support. We plan the TBL in two or three stages separated by a period of at least 3 months, with the anticipation of revisions some time later. The first stage includes a lower body lift with an abdominoplasty and at times a medial thighplasty. If an upper body lift with a reverse abdominoplasty is needed, then that operation is usually set for the second stage along with a medial thighplasty. If the upper body lift does not include a reverse abdominoplasty, then a back roll excision, mastopexy, and brachioplasties are performed during the first stage. The vertical medial thighplasty may be performed then or at a second stage with any revisions needed from the first stage.
Introduction
Massive weight loss (MWL) patients are troubled by pervasive redundant and lax skin. With over 200,000 bariatric operations performed each year in the United States and the increasing acceptance of plastic surgery, there are large numbers of individuals presenting for body-contouring surgery.1 The timing and staging of their procedures consider a host of variables relating to deformities, the nature of the patient, and the temperament and preparation of the plastic surgeon. Some patients focus on correcting one or two areas, whereas many others seek surgery for all affected areas of the trunk, extremities, and face. With so many major operations needed to be done, complex planning must take place. Nevertheless, there is no consensus on the extent of surgery being done at a given operative session.2 Long operations with multiple procedures are advocated by some surgeons.3–5
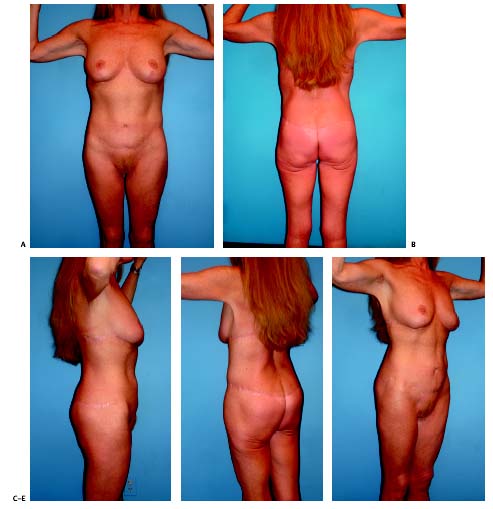
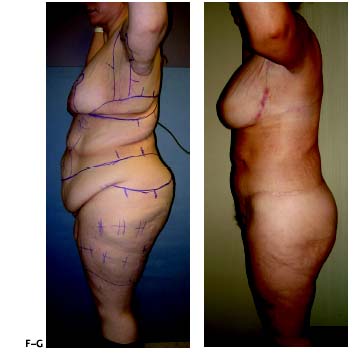
Total body lift (TBL) surgery was conceived in response to the desires of the majority of our patients, who request comprehensive surgery in as few stages as safely possible.6 Otherwise, they face the daunting prospect of repeated major operations over several years. It appears that few of my patients and those of other prominent plastic surgeons complete their surgical rehabilitation when it takes more than three stages due to emotional, physical, and financial exhaustion. TBL approaches both the upper and lower body deformities, which may include the arms and thighs.6–8 The arbitrary, and by no means fixed, criteria for single-stage TBL are a young age (<age 50), health and physical fitness, no obesity (BMI <30 kg/m2), and a high level of motivation. As there is no independent validation of any of these criteria, they need not be strictly observed. The optimal patient has lost all excess weight and is left with significant redundancy of skin that would be benefited by body lift surgery. Few patients are ideal candidates, and, as such, adjustment should be made in reducing expectations and accepting higher risk. Nevertheless, satisfying results can be achieved in both the normal and overweight patient ( Figs. 8.1, 8.2, and 8.3 ). Revision procedures are common but relatively minor.
The major question confronting the decision to perform multiple operations at one time is When is surgical trauma excessive and too long MWL individuals are not traditional cosmetic patients; although these cases are elective, they are not entirely aesthetic. These patients have significant and generalized acquired deformities with functional and psychological issues. For many patients, anything less than comprehensive surgical rehabilitation is a failure, because they still are left with unacceptable residual deformities. Over the past 10 years, this author has been impressed by the resiliency of most of his patients after 8 to 10 hours in the operating room. There are notable exceptions of malnourished, overweight, or poorly adaptive individuals, who should have been better screened and either excluded or better prepared. With the expeditious management of blood volume and blood loss, patients usually experience an uncomplicated medical course. From their rapid emergence from anesthesia through their usual 3-day hospital course, these patients are alert, responsive, and stable when monitored on the regular nursing floor of the hospital. For relatively few, inadequate pain management of their multiple operative areas is a significant and difficult problem. As experienced during lengthy free flap reconstructions, it is clear that prolonged surgery on the skin is not as traumatic to the body as visceral or muscle surgery.
Although TBL surgery dramatically improves body contour, wound healing complications are common.8 Analyzing our results and reviewing the literature have led to an evolution in our patient selection, preparation, operative technique, and aftercare, with a demonstrable reduction in risk.9 As such, over the past few years we have been able to adhere to our philosophy to safely accomplish as much as we can in a given extensive operative session.
Indications and Patient Selection
A medical history is taken with special inquiry into obesity and its associated comorbidities. A long-lasting problem with vast fluctuations in weight may have led to chronic disease. Patients should be questioned about illness prior to their MLW. Diabetes, hypertension, arthritis, obstructive sleep apnea, asthma, congestive heart failure, and depression and other psychiatric problems are a few common comorbidities. The ensuing course of these diseases should be documented; most have either greatly improved or have been resolved with weight loss. With weight loss, dosages of medications may need to be reduced. If the weight loss was exclusively through diet and exercise, nutritional imbalance is a concern. The type of weight-loss surgery and the response of the patient to, and complications from, the bariatric surgery and any other operations are noted. Repeated infections, especially methicillin-resistant Staphylococcus aureus(MRSA) infections, hematomas, and hernias suggest a poor immune response or wound-healing capability, which suggest a conservative start. Prior to body-contouring surgery, weight loss should have reached desired levels, with body weight stable for 3 months. General or specific malnutrition should be considered if there is chronic nausea, vomiting, diarrhea, persistent obesity, or dietary limitations. The types of bariatric surgery, such as adjustable gastric lap band (AGB), Roux-en-Y gastric bypass (RYGBP), and duodenal switch, have their own characteristic nutrient deficiencies, which must be searched for and replenished.10
Many overweight, obese, or morbidly obese patients may have preexisting micronutrient deficiencies of vitamins and minerals, a condition referred to as “high-calorie malnutrition.”11 These deficiencies are exacerbated after both restrictive and malabsorptive procedures and include macro-nutrient as well as micronutrient deficiencies. Indeed, many more patients have subclinical deficiencies that can potentially become clinical after the stress of surgery or wound healing. Ironically, many of the deficient macro- and micronutrients are the essential elements of efficient wound healing. Thus, it is understandable that body-contouring procedures in these patients have had a high rate of wound-related complications.
Protein deficiencies are known to lead to increased inflammation, decreases in wound tensile strength, and an increase in overall morbidity. In our study of 48 postbariatric patients, 38% were found to have a prealbumin of less than 20 mg/dL.10 Furthermore, another 46% were found to have a prealbumin ranging from 20 to 25. Thus, 84% of the patients had a prealbumin of 25 mg/dL or less. Since our evaluation of our first 5 years of total body-contouring patients,8 we have started supplementation of our overweight, obese, and postbariatric body-contouring patients with a specific nutritional formula to support wound healing and to enhance recovery. Special attention is given to educating obese and postbariatric patients to ensure compliance, which can be suboptimal at times. We have used ProMend ABG (Catalina Lifesciences, Irvine, CA) with supplemental vitamins exclusively in the past, but now commonly use our customized formula of ProCare M.D. (Nutressential, Wilmington, CA). Each serving of this supplement contains 20 g of protein, 3 g of free amino acid, 4 g of arginine, 1 g of glutamine, minimal requirements of vitamins A, B12, B6, and C, and folate, iron, copper, zinc, and selenium. Occasionally, we observe a compliance problem due to nausea.


The MWL patient must understand the surgical plan, its alternatives, and its risks. The motivations for the surgery and the desired pace of staging are ascertained. Motivation for a single stage means acceptance of a longer recovery, more pain, and increased risk of complications. Reduced weight but persistent obesity increases complications, as does smoking. Long operations in other fields of surgery have been associated with increased rates of blood transfusions, wound infections, and thrombophlebitis. However, there has not been shown to be a significant difference for major or minor complications for MWL patients who have several staged procedures as opposed to a TBL.3–5,8 In Borud series, patients undergoing single-stage surgery had a 12.5% major and 50% minor complication rate, as compared with patients undergoing more staged surgeries, who demonstrated a 14.3% major and 73.6% minor complication rate.3 The number of transfusions given was greater for the single-stage group.
Most patients have lost 80% of their excess weight by 1½12; years after bariatric surgery. Hence, the scheduling for the first stage in body contouring should be at about 18 months after the bariatric surgery and after 3 months of stable weight. Major surgery with ongoing further weight loss may compromise wound healing because of a catabolic state and malnutrition. Significant weight loss after body-contouring surgery is likely to cause recurrent skin laxity. There should be adequate weight loss that resulted in appreciable skin laxity. Inadequate weight loss forces closure of heavy tissues with frequent wound-healing problems. Despite the best intentions, late adverse weight changes do occur some years after surgery. Either generous weight gain or loss can devastate results.
Patients should be made aware that compromises in the operative plan, such as shorter scar procedures, may affect the quality of the improvement. The patient should have reasonable expectations and understand the unpredictability of wound healing and scars. The patient should be cognizant of the potential for serious, even life-threatening, complications and should realize that, on a given day, multiple operations carry greater risk than one or two operations.
When staging the procedures, a decision needs to be made regarding which ones to combine. I recommend approaching the areas of highest priority first. Improvement in those areas is likely to give the patient the greatest satisfaction and impetus for continuing the surgical rehabilitation.
The operative plan is based on the evaluation of the patient, the patient’s priorities, and the patient’s preparedness to follow through on the surgical recommendations. The previous section of this chapter discussed this evaluation. By our definition, operating on both the upper and lower body at the same time constitutes a TBL. When patients fail to lose excess weight and take the prescribed supplements, complications increase.
Related posts:
 4 Anesthesia and Safety Considerations in the Perioperative Period
4 Anesthesia and Safety Considerations in the Perioperative Period
 5 Propofol/Ketamine Anesthesia
5 Propofol/Ketamine Anesthesia
 7 The Anatomy and Chronology of Body Sculpting: Areas Requiring Correction and Timing of Procedures
7 The Anatomy and Chronology of Body Sculpting: Areas Requiring Correction and Timing of Procedures
 6 Factors Impacting Thromboembolism after Bariatric Body-Contouring Surgery
6 Factors Impacting Thromboembolism after Bariatric Body-Contouring Surgery
 9 Postoperative Pain Management Following Body Contouring
9 Postoperative Pain Management Following Body Contouring
 36 Facial Rejuvenation: Open Technique
36 Facial Rejuvenation: Open Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


