37 Short-Scar Rhytidectomy
Abstract
Facial rejuvenation is often considered an ancillary procedure in massive weight loss (MWL) patients. However, with the popularity of bariatric surgery in conjunction with an aging population, the demand for facial aesthetic surgery concomitantly has increased in MWL patients. The approach to rhytidoplasty in MWL patients, whether as a result of the normal aging process or deflation of the face with weight loss, is similar to that in the general population. However, there are some unique considerations in MWL patients that may accentuate or accompany the normal aging process. These include a greater absence of subcutaneous fat, more excess skin than might be encountered in a non-MWL patient of the same age, loss of fixed points of osteodermocutaneous ligaments, and more damage to dermal elements from repeated weight fluctuation. Although any facelift that achieves the desired goals is acceptable, our preferred approach to MWL patients, as well as the general population, is the short-scar rhytidectomy with fibrin sealant and barbed suture fixation. This procedure allows a shorter and well-hidden scar as well as no disruption of the hairline position or density, a potentially shorter operative time, and a high degree of patient acceptance. With experience, the surgeon can overcome the restrictions of the narrower operative field and gain comfort adjusting the discrepancy in the skin flap during closure. Although a single technique is not appropriate for every patient, we have found wide applicability of the short-scar facelift in the MWL population.
Introduction
As this textbook demonstrates, the unabated pandemic of obesity and the expanded application and development of bariatric surgery through minimally invasive techniques have created a whole new arena for plastic surgeons.1–4 Plastic surgeons are an integral part of a multidisciplinary team that includes internists, weight-loss specialists, dietitians, psychiatrists, and bariatric surgeons.5,6
The expectations of massive weight loss (MWL) patients have grown beyond functional surgery, such as panniculectomy and brachioplasty, to aesthetic surgery, including body sculpting, breast enhancement, and facial rejuvenation.7 The MWL patient presents a challenge because the elastic and structural components of the facial and body skin are often overwhelmed from accelerated weight loss in a pattern similar to, but structurally different from, natural aging ( Fig. 37.1 ). Younger MWL patients, to varying extents, experience remarkable recoil of their facial skin, more so than is observed in their torso. However, as this population ages and as bariatric surgery is expanded to include older patients, the role of facial rejuvenation surgery in MWL patients warrants greater attention.
The aging process occurs over years. However, the MWL patient undergoes rapid transformational changes physically, structurally, and histologically following bariatric surgery. In addition to the known nutritional and metabolic deficiencies affecting wound healing and collagen production, our experience has shown that many MWL patients have a greater absence of subcutaneous fat, greater skin burden, more loss of fixed points at areas of osteodermocutaneous ligaments, and more damage to dermal elements.8 Despite the dissimilarities in process, both the aging patient and the MWL patient have a common end result: loose, ptotic skin and underlying facial structures that respond similarly to surgical intervention.

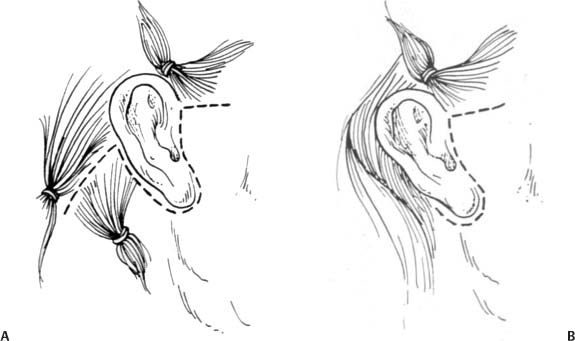
Although any facelift procedure that achieves the desired result may be helpful, we prefer the short-scar rhytidectomy with fibrin sealant and barbed suture fixation in the normal population as well as in MWL patients.9 The facelift technique has evolved from the traditional open facelift incision ( Fig. 37.2 ), extending in a continuous line from the temporal region to the preauricular region, around the earlobe, the postauricular region, and ending with a pre- or post-trichal occipital limb, to the modified open technique ( Fig. 37.3 ), replacing the temporal extension of the incision with a sideburn incision, to the short-scar incision ( Fig. 37.4 ), extending from the sideburn incision to the preauricular region around the earlobe and ending 2 to 3 cm above the lobule in the postauricular sulcus.10 Although patients will accept scars if they achieve their desired results, we have found that patients naturally prefer the less invasive approach, including the shorter incision, so long as the end result remedies their concerns.
All our patients undergoing the short-scar facelift have their fat removed, repositioned, or selectively replaced. Most have submentalplasty with a platysmaplasty. In contrast to the traditional facelift, the short-scar facelift usually requires additional midline platysmal work to shorten redundant platysma and deepen the cervicomental angle. The medial vector pull on the platysma is important for defining the cervicomental angle and for redraping of excess skin into the submental hollow. In accordance with the Pythagorean theorem, as the angle is deepened (lengthening of the limbs), a greater amount of excess skin can be accommodated medially. This technique gives improved definition to the patient’s neck and jawline, while reducing the amount of redundant skin that needs to be excised or incorporated into the shortened scar.

Three advancements that we have integrated—barbed suture for superficial musculoaponeurotic system (SMAS) plication, ball-tip cautery for liposculpturing, and fibrin sealant prior to closure—have enhanced our results and improved the postoperative recovery substantially. We have incorporated barbed 2–0 Monoderm suture (Quill SRS, Angiotech, Vancouver, BC) into the SMAS plication and lateral platysmal suspension as described below. The barbed sutures fasten the SMAS securely while distributing the tissue tension for an even, uniform plication. The advantage of the ball-tip cautery (Teleflex Medical, Research Triangle Park, NC) is twofold. The cautery provides additional hemostasis throughout the operative field while allowing the surgeon to selectively contour the underlying adipose tissue through thermal lipolysis. The resultant effect is a smooth plane of tissue over which to redrape the overlying skin and fewer postoperative palpable irregularities. Finally, the use of fibrin sealant (Tisseel, Baxter Biosurgery, Deerfield, IL) has obviated our need for postoperative drain placement. As described below, the fibrin sealant is placed as the last step prior to skin closure. The elimination of routine drain placement has improved our postauricular incision closure and skin redraping. Because they increase skin bunching at the postauricular site, eliminating the drains improves the postauricular closure and healing, as well as the known disadvantages of drains.
The short-scar facelift with barbed suture and fibrin sealant is our standard rhytidectomy procedure that has been used in about 1000 consecutive cases of facial rejuvenation. We have seen wide applicability in both the MWL population and the general population.
Indications
The indications for the short-scar facelift with barbed suture and fibrin sealant include the patient with the appropriate anatomy desiring facial rejuvenation classically addressed via a traditional facelift incision, and MWL patients are included. Indeed, the sine qua non of our ability to use the short-scar facelift with tissue sealant and barbed sutures is the MWL patient. The degree of skin laxity in the MWL patient should not deter the surgeon from the short-scar technique. Although any incision is acceptable, as seen in Fig. 37.5 , effective results can be achieved with the short-scar techniques described in this chapter.
Careful preoperative planning, consultation, and communication with the patient are essential. Patients with midface, jowl, and neck laxity and lipodystrophy are excellent candidates for this procedure. With continued experience, even patients with excessively loose necks can achieve excellent results. Ancillary facial procedures commonly performed at the same setting include upper and lower blepharoplasty, fat grafting to the lips and nasolabial creases, laser resurfacing, buccal fat pad resection, and rhinoplasty.
Patients are counseled preoperatively to stop all anticoagulant medications and herbal supplements, cease smoke exposure, both direct and indirect, and obtain medical optimization and approval of our medical consultant and anesthesiologist.


Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


