34 Weave Lift Facial Suspension

Abstract
Approaches to facial rejuvenation have evolved over the past several years, with the focus shifting from skin excess to volumetric considerations. Younger patients after massive weight loss, particularly those under 45 years of age, may have descent of soft tissue in the face but minimal to no excess skin. There have been three major trends in facial aesthetic surgery that have emerged in recent times: a desire on the part of the patient to have more limited visible incisions, a desire to have shorter postoperative recovery periods, and, most importantly, a clearer understanding of the volumetric changes that occur with aging. We have utilized a suture suspension technique called the “weave lift” to resuspend and reshape ptotic facial structures along specific anatomic vectors in this patient population. Monofilament nylon sutures are placed percutaneously with specifically designed long needles through stab incisions. The suture is then “woven” into the soft tissue of the face, engaging it in several planes to prevent the “cheese-wiring” effect observed with some other suture suspension techniques. The weave lift can be used along these specific vectors to effect lateral brow elevation, midface elevation, lower face suspension, and neck suspension. Excellent results have been achieved in patients with 3-year follow-up. Complications are minimal, as general anesthesia and wide skin undermining are avoided. The technique can be combined with a short scar around the ear for skin redraping in patients with skin redundancy if necessary. Preoperative, intraoperative, and postoperative photographs illustrate the procedure and results. Near complete maintenance of the corrected result has been demonstrated in 40% of the patients at 24 months postoperatively.
Introduction
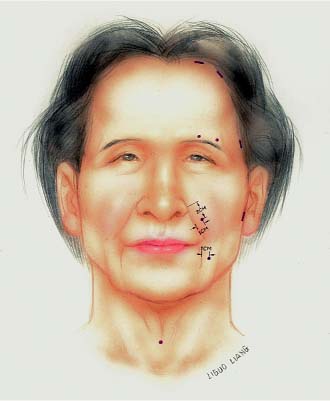
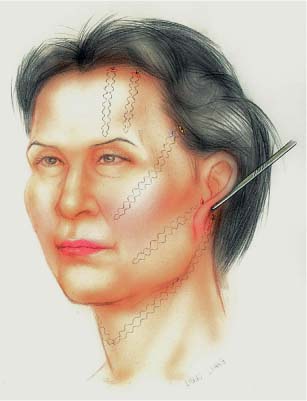
The historic approach to facial rejuvenation, which emphasized excision of excess skin and its redraping, has been replaced by a more holistic approach that includes consideration of volumetric changes that occur with aging. These changes are exacerbated by massive weight loss. They include changes in skin elasticity and facial soft tissue descent, as well as some facial soft tissue atrophy. Volu-metric changes in the massive weight loss patient are not limited to the trunk and extremities. Pronounced deflation of facial soft tissues structures is often observed, which is manifested as midface descent, prominent nasolabial folds, marionette lines, brow ptosis, and skeletonization of the malar eminences. In the younger patient, especially patients under 45 years of age, elevation of facial soft tissue descent may be as important as or more important than surgical treatment of skin elasticity and excess. Recent volumetric studies of the face, including the work of Little,1 have demonstrated that descent of facial soft tissue structures contributes to the characteristic features of aging. Newer techniques in facial rejuvenation that address soft tissue reshaping include, over the past several years, superficial musculoaponeurotic system (SMAS) flaps and midface lifts.2–4 Vectors have been defined along which soft tissue descends with aging and with weight loss. These vectors include a midfacial vector, along which the malar soft tissue and fat pad descend, causing a loss of the youthful prominence of the malar area. In addition, along specific vectors, lateral brow descent and relaxation of the neck soft tissues occur ( Figs. 34.1 and 34.2 ). Techniques utilized to correct malar descent include malar imbrication,1 a variety of suture and sling resuspension methods,5–14 and placement of prosthetic meshes and implants.2 Autogenous and prosthetic materials have been used to increase volume in the face, including fat, dermalfat grafts, and a variety of soft tissue fillers.15,16 A study involving over 400 patients demonstrated the marked improvement in facial appearance attainable by malar fat pad elevation alone using suture suspension.17 Suture suspension18 and galeal resuspension procedures have been described to address lateral brow ptosis.19 Neck suture suspension platysmaplasty has been used for many years for neck rejuvenation.20 We describe a suture suspension technique, called the “weave lift,” that can provide minimally invasive midface, lateral brow, and neck rejuvenation using percutaneously placed nylon sutures along specific vectors in the carefully selected patient.

Indications
The success of any technique is dependent on patient selection and the indications for which it is applied. We have found that the younger weight-loss patient, generally younger than 45 years of age, may be a good candidate for the weave lift. These patients generally demonstrate descent of the mid-face, with skeletonization of the malar eminences, nasojugal grooving, and deepening of the nasolabial folds. In addition, descent of the lateral brow and of the neck with platysmal diastasis and banding is common. Patients with significant skin excess along the face and neck are not good candidates, as skin redraping may be necessary in these patients concomitant with soft tissue redistribution. Significant skin excess is generally observed in older patients who undergo massive weight loss, especially over 45 years of age.
A wide variety of suture suspension techniques have been employed in this patient population for rejuvenation of the face as well as in cases of facial paralysis.21 Many suture materials have been used, including absorbable and nonabsorbable ones, most commonly polytetrafluoroethylene,22 polydioxanone,6 polypropylene and barbed polypropylene,8 and monofilament nylon. Based on a study in an animal model that showed the lowest inflammatory reaction to and capsule formation around monofilament nonabsorbable suture materials,23 we have employed monofilament nylon sutures in these cases.
Technique
The procedure is almost always done in the office setting with the patient under local anesthesia, 0.5% lidocaine with 1/200,000 epinephrine. An oral sedative preoperatively may make patients more comfortable. Vectors are marked on the face using a marking pen. The eyebrow vector is marked from the mid-eyebrow to the hairline and lateral aspect of the brow to the hairline. The midface vector is marked from 2 cm inferior to the apex of the nasolabial fold and 1 cm lateral to the fold along a line that bisects a point 1 cm lateral to the lateral canthus and ends 2 cm into the hairline. The lower face vector starts 1 cm lateral to the lower nasolabial fold at the level 1 cm below the lip commissure. This extends laterally to a point of juncture of the lower tragus with the lobule and ends at the preauricular sulcus. The neck sutures start at an 8 mm incision in the midline at the level of the cricoid cartilage ( Figs. 34.1 and 34.2 ). The suture is passed in the deep subcutaneous level along a vector from the midline to the mastoid prominence. When the second half of the suture is passed, the two sutures are intertwined at the midline ( Fig. 34.3 ). In patients with mild skin excess, a preauricular incision may be marked, extending from the temporal hair into a tragal incision, and to the ear lobule or just posterior to the lobule in the postauricular crease. Minimal skin undermining in the preauricular area is planned in these cases, usually less than 2 cm. In many cases, after the malar fat pad and lower lid fullness is restored, only a simple lateral pinch blepharoplasty and canthopexy are needed to restore the youthful contour to the lower lid. The upper lid is significantly improved with the eyebrow lift, and, if needed, a limited excision of skin is added above the palpebral fold.
Lidocaine with epinephrine is infiltrated along the vector lines and in any lid or preauricular skin excision areas. The brow hairline sutures are secured to the galea; the midface sutures are secured to the temporalis fascia; the lower face suture is secured to the SMAS over the parotid; and the neck sutures are secured to the periosteum of the mastoid prominence. The levels of the sutures are as follows: the forehead at the level of the galea, and the midface through Bichat’s fat pad and then along the superficial aspect of the orbicularis oculi muscle to the temporalis fascia. The lower face is through the SMAS and secured to the preauricular SMAS. The neck sutures are passed at the deep subcutaneous level, exiting at the mastoid and secured to the periosteum of the mastoid.
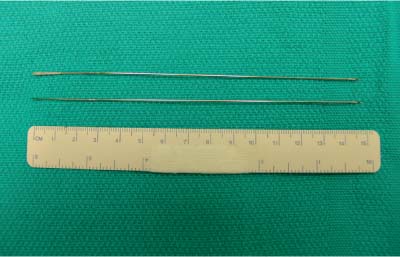
The 3–0 clear nylon suture is secured to the Weavelift needle, a 15 cm Keith-type needle (ASSI, Westbury, NY) at either end. A 2–0 nylon suture is used for neck suspension. A stab wound is made at the medial entrance wound, the needle is introduced and then woven either laterally or superiorly, depending on the vector, and brought out at the exit incision. The second needle at the other end of the suture is introduced through the same stab wound and woven through the tissues to the exit point. The needles are then removed and exchanged for round needles to better allow passing the suture to the anchor tissue. When the suture is tied, movement of the tissue is visible, and the tissue is raised symmetrically on each side. The midface suture sometimes causes a dimpling of the cheek skin. This can be relieved by firm massage of the entrance region. When the sutures are tied, there is an accordion effect of the sutures, allowing for firm multilevel attachment securing the sutures.
Elevation of the upper brow eliminates most of the upper lid excess. Elevation of the midface causes a bunching of the lower lid skin, which is amenable to a pinch blepharoplasty. This movement of tissue usually corrects the tear trough deformity and lower lid bulging. A lateral pinch of skin at the lateral canthus is excised. This can be complemented by a lateral canthopexy with 5–0 nylon suture to improve lower eyelid tone. In the older patient with some skin excess, the preauricular skin excision can be performed at this time as well. A light dressing is applied. Skin sutures are removed at 5 to 7 days.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


