35 Midfacelifting
Abstract
The gravitational effects on the midface, commonly seen with aging, are accentuated considerably by the effects of very rapid weight loss in the postbariatric patient. All of the soft tissue structures of the face are affected, manifested by deepening of the nasojugular folds and descent of the malar fat pad, which produces the jowls along the ramus of the mandible. This results in relative flattening of the prominence of the zygoma. At the same time, there is lowering of the corners of the mouth, giving the patient a saddened appearance. These changes, among others, are herein described, and methods for their satisfactory and lasting correction are outlined in detail.
Introduction
The Problem: Obesity
In 1995, the sentinel work by Pories et al1 reliably demonstrated the dramatic success of gastric bypass in achieving substantial weight loss. Multiple studies have subsequently published similar data corroborating the findings of Pories et al, documenting the long-term efficacy of gastric bypass in maintaining weight loss and effectively reversing diabetes, hypertension, dyslipidemias, obstructive sleep apnea, gastroesophageal reflux, and other disorders.2
These benefits, however, are achieved at an unfortunate price. The resultant changes in body morphology after massive weight loss (MWL) are significant and can dramatically affect a patient’s physical and emotional well-being. Significant body contour deformities affect the face, arms, breasts, abdomen, mons pubis, flanks, back, buttocks, and thighs. The significant skin excess and laxity, diffuse lipodystrophy, and ptosis in the truncal areas are a source of postural, functional, hygienic, dermatologic, and aesthetic impairment. Despite these apparent hindrances to quality of life, in some patients the aforementioned issues take a back seat to the issue of facial skin excess. This has spawned a new generation of post–bariatric surgery patients all over the country seeking out the expertise and artistic sense of a plastic surgeon who can address the dramatic contour disfigurements of both trunk and face that result from MWL.
The facial contour irregularities that occur as a result of MWL are most analogous to the aging process, albeit accelerated. The sine qua non of physical exam findings of the face and neck in MWL patients is excess skin. The loss of sub-cutaneous fat, decreased skin tone, and sagging redundant skin result in ptosis of the facial structures, including the corners of the mouth and lower cheeks, with excessive jowling and obliterated neck lines. The malar fat pad descends and produces a hollowing effect in the infraorbital region. To illustrate the similarities between the changes in facial morphology incurred with MWL and those of aging, and to adequately understand the problem that our proposed technique sets out to address, a detailed look at the aging process is warranted.
The Aging Process
The aging process is regulated by genetic and environmental factors (e.g., illnesses, sun exposure), lifestyle, and gravitational migration. These changes manifest in different parts of the face at different rates and vary from person to person. With age, changes in the face result from the disproportional descent of the skin, fat, superficial musculoaponeurotic system (SMAS), and muscles over the skeletal framework. The midface is affected by age more noticeably than other areas. Typically, these include a pronounced nasojugal line and infraorbital hollowing, lateral canthal relaxation, malar flattening, cheek ptosis, nasolabial fold prominence, marionette line formation, and jowl laxity.3
The eyebrows droop, and permanent wrinkles appear in the periorbital areas because of decreased skin elasticity. The nasojugal fold deepens because of descent of the lower lid skin and loosening of the orbicularis muscle. The drooping of the corners of the mouth, with the commissures adopting a downward orientation, implies a tired and sad appearance ( Fig. 35.1A ).
These stigmata of the aged face are seen prematurely in postbariatric patients with MWL. This occurs as the gravitational force from the weight of redundant facial skin pulls on the malar fat pad and its suspensory structures, as well as those of the SMAS. This, coupled with fat atrophy in the submalar region, leaves a sagging and hollowed appearance reminiscent of the findings seen in the aging process ( Fig. 35.1B,C ).4
The contour alterations in MWL patients can be a significant cause of anxiety for patients and, in certain cases, may supersede a patient’s desire for truncal contouring. Attempts to restore facial contour, akin to rejuvenating the aging face, should aim at repositioning the facial structures that have atrophied or lowered. This correction is achieved mainly by vertical restoration of the soft tissues to their original position. It is the belief of the senior author that the appropriately placed SMAS plication, malar fat pad elevation, and adjunctive brow, superior palpebral, and lateral orbital rejuvenation procedures, in concert with an appropriate cervicoplasty, can address the myriad anatomic sequelae of facial contour disfigurement caused by MWL. Our preferred technique addresses the volume loss from fat atrophy and the sagging due to the gravitational pull exerted on the redundant atonal facial skin and the suspensory structures of the malar fat pad and SMAS.
The Solution: Surgery
The recognition that the sagging redundancy of MWL and the midface ptosis of aging share a similar pathophysiology affords us the opportunity to apply similar surgical strategies for both, employing modifications and adjustments as necessary based on the patient’s unique facial contour morphology and specific complaints. Attempts to rejuve-nate the MWL face should include vertical elevation of the soft tissues to their original place. This is accomplished via suture suspension of the malar fat pad, a technique that has been demonstrated to be safe and effective, and can be used in the postbariatric patient.5 It restores the deep structures of the face to a more youthful position and allows the excess skin to be resected and skin edges apposed without tension. After a facelift, the tissues undergo changes related to the plane of dissection (there is more edema the deeper the plane), vector of pull (windswept appearance for lateral vector), closure tension (widening of scars), and placement of incisions (visibility, dog-ears). Sequelae of the traditional facelift technique include an increased distance between lateral orbit and temporal hairline, elevation of the sideburn above the junction of the ear with the scalp, tragal distortion, misplaced postauricular scars, hollow eyes, and a lateral sweep appearance.6–8 These unattractive consequences can be averted with our technique, giving the face, instead, a natural and rested appearance. In addition, to achieve increased facial harmony, attention is given to the forehead, eyebrows, periorbital region, nasal tip, lips, chin, and neck as warranted.9,10 The procedure produces lasting results and a high level of patient satisfaction.

Relevant Anatomy
The central third of the face is defined by a triangle with its base at the forehead hairline and its apex at the tip of the chin. The malar fat pad is the main structure within the central third of the face and is considered the primary structure in the facial aging process. However, the malar fat pad is also the principal target of facial rejuvenation strategies due to its contribution to the youthful appearance.
First described by Owsley in 1997,10 the malar fat pad is a discrete fibrofatty mass, “triangular in shape with the base at the nasolabial fold,” fixed in place by suspensory ligaments attached to the skin above and the SMAS below. The youthful face displays a smooth convexity that traverses the lid–cheek junction and continues through the midface to the mandibular margin, imperceptibly feathering out laterally. This is the result of a well-incorporated malar fat pad into the surrounding superficial fat layer of the remainder of the face. Although the malar fat pad rests on the SMAS, its loose adherence allows for subtle movements of the facial musculature beneath, without drastic movements of the malar fat pad and midface skin above.11 Anteromedially, however, the SMAS coalesces with the zygomaticus major and periorbital orbicularis oculi, allowing muscle contraction to be transmitted to the superficial layers of the face.
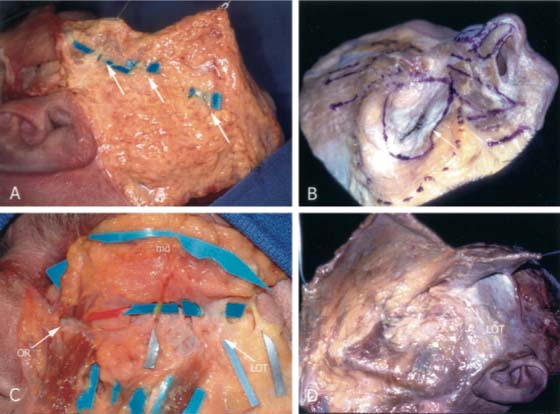
Although the interface between the SMAS and malar fat pad may be obliging as regards facial movements, it unfortunately allows the effects of gravity to have a disproportionately greater impact on the more superficial facial layers, rendering the malar fat pad and skin more ptotic with increasing age. Laxity over time of the malar suspensory structures results in ptosis of the malar fat pad. These structures are clearly identified and displayed on the fresh, hemifacial cadaver dissections performed by Gamboa et al12 in 2004 ( Fig. 35.2 ).
The SMAS is a fibroadipose layer that is continuous with the orbicularis muscle and the galea superiorly and the platysma muscle inferiorly. It is anchored strongly to the zygomatic arch. Manipulation of the SMAS by lateral resection or imbrication has its major effect in the neck.
History Through Surgical Options
A cursory glance at the history of facelifting allows one to note the great advances that have been made. These are, in large part, attributable to progressive anatomic discovery and an increased understanding of skin and muscle physiology. The origins of facelifting were essentially the skin-only lifts pioneered by Holländer, Lexer, Joseph, and Passot at the turn of the last century.13–16 These early procedures were rudimentary and consisted of skin removal near the hairline without any deliberate undermining.
In 1926, Hunt described elevation of the brows with coronal, anterior hairline, and direct incisions,17,18 Hunt in 1926 and Passot in 1930 performed excisions of the glabellar region and above the eyebrows to manage the glabellar creases and to elevate the eyebrows, respectively.18 Lexer in 1931 described incisions for the forehead lift and facelift in his book Die Gesamte Wiederherstellungs-Chirurgie.18,19 Claoue in 1933 proposed more extensive undermining of the forehead, face, and neck.18 Through these procedures, evolution in facelifting occurred but had minimal effect on the mid-face.
Gonzales-Ulloa19 in 1962, Viñas and coworkers20 in 1965 and 1976, Tessier21 in 1979 and 1989, and Ortiz-Monasterio and coworkers22 in 1978 performed coronal incisions and elevated frontal flaps for frontal and midfacelifting. Mitz and Peyronie23 originated the term superficial musculoaponeurotic system (SMAS) in their anatomic studies in 1976. Even before this time, Skoog24 in 1974 abandoned the idea of using skin excision and tension as the key facelifting element, and instead dissected sub-SMAS and used the deeper layer for suspension. These descriptions were catalysts in shifting the focus of facelifting from skin to the deeper planes and highlighted how the midface can be manipulated for effective rejuvenation.
The notable works of Tessier,25 Psillakis,26 Hamra,27 Krastinova-Lolov,28 Ortiz-Monasterio,29 and others are very nicely reviewed by Paul et al.30 These contributions explore various strategies for facelifting based on different depths of dissection. They represent the multitude of important evolutionary steps and refinements that have occurred since the subperiosteal “mask-lift” of Tessier. Although making it difficult to compare results, the existence of various techniques underscores the necessity of tailoring the operative procedure to the individual needs of the patient.31
Furthermore, endoscopic facial surgery has undoubtedly bolstered the rejuvenation armamentarium. The birth of endoscopic plastic surgery occurred in the 1990s. This technique was accomplished by creation of an optic space with dissection and was first introduced by Core and Vasconez at the fall meeting of the American Society of Plastic and Reconstructive Surgeons in 1992.32 Although endoscopy was first used for browlifting, it was later applied in facelifting, cervicoplasty, mammaplasty, abdominoplasty, and gynecomastia operations. The senior author’s preferred technique incorporates browlifting, when appropriate, as part of the overall treatment in the creation of a harmonious, natural appearance for the MWL patient.
Our Preferred Approach
To safely and effectively approach the patient after MWL, the goals of the operation must be tailored to the individual. That being said, most contour irregularities in this patient population are relatively similar. There is excess skin, infraorbital hollowing, loss of subcutaneous fat, and an overall lowering of facial structures. The technique that we believe produces the most impressive and lasting results is the subcutaneous approach to the lateral malar fat pad with vertical elevation coupled with varying degrees of SMAS plication determined by the remaining facial and neck anatomy. This is discussed in detail in the following subsections.
Elevation of the Eyebrows
The eyebrows begin drooping at age 26 in most people. This descent also applies to the MWL patient, and, if anything, it is probably accelerated. Elevating the eyebrows is important, particularly beyond the fourth decade of life, because as one addresses the patients’ midface and the neck, to leave them with wrinkled foreheads would indicate disharmony and a loss of balance to an otherwise rejuvenated face.
Elevation of the eyebrows is best accomplished by the endoscopic approach. With over 15 years of experience, we have proven this technique to be physiologically correct, effective, and lasting. There are additional advantages: the coronal incision is avoided; there is no increase in the height of the forehead; and paresthesias, which are caused by manipulation of the supraorbital nerves, are usually transient and disappear in 3 months. Only the occasional patient may develop lasting dysesthesias requiring attention.
The important steps for a successful endoscopic forehead-lift are the following:
Subperiosteal dissection to the supraorbital rims and extension of the dissection to the tip of the nose with a blunt elevator
Division of the periosteum at the level of the supraorbital rims from the supraorbital nerves to the lateral orbital rim on each side
Ablation of the glabellar musculature, which is responsible for the convergence and lowering of the eyebrows
Avoiding periosteal excision during glabellar musculature ablation is imperative. The periosteum is at a different layer from the muscles, and, if removed, will give rise to undesirable depressions in the forehead. The reason for extending the dissection to the tip of the nose is that it serves to slightly shorten the elongated nose, but it also exposes the procerus muscle in its entirety. In patients who have a transverse wrinkle at the level of the glabella, that wrinkle is ameliorated or disappears by extending the dissection to the tip of the nose.
We suggest three incisions at the hairline level. The incisions are actually excisions of small triangles of skin with the apex oriented toward the nose so that when closing the wound the incision will be transverse and at the hairline. Placing the incisions in front of the hairline is more advantageous than placing them within the hair for two reasons. First, it shortens the distance to the supraorbital rims, greatly facilitating the procedure. Second, it avoids the localized alopecia that invariably occurs when making an incision within the hair.
Three triangles of skin are excised, one in the midline and one at each paramedian level, in line with the midportion of each eyebrow. One should remember that the distance from the midline of the forehead to the supratrochlear and supraorbital nerves is approximately 1.8 cm and 2.8 cm, respectively. The dissection begins at the paramedian incisions with a clamp to avoid dividing the branches of the supraorbital nerves. The sharp subperiosteal elevator is then introduced, and, with bimanual action, the periosteum is dislodged from its attachment to the frontal bone, up to the supraorbital rims. The subperiosteal elevation is limited to the frontotemporal line. Additional incisions along the temple are necessary only if one is to include an endoscopic midfacelift. Three traction sutures are placed, one over each mid-eyebrow and one in the midline, to serve as the optical cavity as the assistant holds them up like a tent. The endoscope, outfitted with an appropriate guard, is then introduced and oriented with 30 degrees of downward angulation to aid with optical field maximization. This allows ample visualization of the nerves, musculature, and frontal bone. The operator, again with bimanual activity, places the nonoperating hand on the skin over the supraorbital rims while bluntly dissecting to free up the musculature along the glabellar region. The supraorbital and supratrochlear nerves are identified. It should be noted that the supratroch-lear nerves are more anterior than the supraorbital nerves, and once the nerves are identified, the periosteum is cut at the supraorbital rim, bilaterally, with a disposable carpal tunnel knife. This is an essential step of the procedure. Cutting the periosteum by itself will allow up to 1 cm of eyebrow elevation. However, after the periosteum reattaches at a higher level, it provides the frontalis muscle an additional mechanical advantage for eyebrow elevation. The glabellar musculature, which has now been freed up completely, is excised from the midline to the level of the supraorbital nerves. There is a superficial vein at that level that is usually maintained intact, but if disrupted, it should be cauterized with a disposable suction coagulator, available in all operating rooms from the ear, nose, and throat (ENT) tray. One should check for complete and equal removal of the glabellar musculature. One sees the subcutaneous tissue through the endoscope when adequately removed. One should not observe depressions in the forehead or at the glabellar region as long as the periosteum is not excised. The wound is then thoroughly irrigated, hemostasis is obtained, and the closure begins.
The closure is performed in two layers. The first layer approximates the galea in an effort to prevent a small but bothersome depression at the site of the triangular excisions. The second layer approximates the skin, and most of the time no dog-ears need to be removed, even though the wound has been closed transversely. The incisions should fall at the hairline level.
The suspension is similarly simple. Three rows of staples are placed: one staple along each incision and a second approximately 2.5 cm posterior to the incision on the scalp. While the assistant holds the eyebrows elevated, 3–0 nylon sutures are placed through the loops of the staples and tied. This is a sufficient and lasting suspension. The last step is to tape the forehead to allow for further reattachment of the periosteum. Most of the time drains are not used, but if there is any question, a small drain is placed in the glabellar region and brought up through one of the lateral incisions to be removed within 24 hours.
The endoscopic forehead lift has proven to be physiologically effective and lasting, and is relatively simple and straightforward. By utilizing the maneuvers indicated above, and with a relatively simple method of suspension, we have completely avoided the potential of overelevation of the eyebrows. We do not favor the use of screws or miniplates or any other soft tissue suspension maneuvers because they are more complex and may give rise to over-elevation of the eyebrows. Sufficient reports are now available to indicate the effectiveness as well as the longevity of this procedure.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


