33 Facial Rejuvenation: Indications and Analysis
Abstract
Massive weight loss can result in profound changes in facial anatomy, in addition to those in the trunk and extremities. These changes are most profound in patients older than 40 to 45 years of age. In addition to skin excess, noticeable volume loss and redistribution that produces midfacial descent, cheek and temporal hollowing, jowling, deep nasolabial folds, and neck ptosis must be addressed. Not to be overlooked are the stigmata of aging in the eyelids that are associated with extreme weight loss. Successful rejuvenation of the face and neck must include restoration of harmony between facial subunits. Often, adjunctive methods such as fillers, implants, and grafts can be combined with facelifting and neck lifting in a cohesive approach. As in body contouring of the trunk and extremities, adequate consideration of nutritional factors, medical comorbidities, and psychological dimensions is crucial.
Introduction
There are numerous reports on body contouring after massive weight loss (MWL). In contrast, there has been a paucity of literature about the effects of MWL on the face and its treatment. Many weight-loss patients say that the facial changes are of less concern to them than the changes that have occurred to their breasts, abdomen, back, and thighs. Often, these patients undergo a variety of body-contouring procedures well before they consider any facial surgery. However, it is predicted that as the number of MWL patients increases, more patients will seek facial surgery as an adjunct to their overall rejuvenation.
Many of the anatomic changes that result in deformity of the breast, abdomen, back, and thighs with MWL also occur in the face and neck. Loss of skin tone and elasticity, redundant skin, and loss of soft tissue support and volume can contribute to an appearance of premature aging. On the other hand, the facial anatomy presents some unique considerations. In contrast to the breasts, abdomen, back, and thighs, facial deformity cannot be as easily concealed with clothing. The more complex nature of facial structure, including the relationships between subunits of the face, including the neck, cheeks, eyelids, forehead, and nose, precludes the surgeon from viewing each part of facial anatomy in isolation to restore harmony and balance between facial features. As the face is one of the major focal points of one’s appearance and a large part of one’s identity, adequate consideration must be given to the effects of MWL on the facial anatomy and the treatment options available, as well as the psychological dimensions involved, including effects on self-perception.
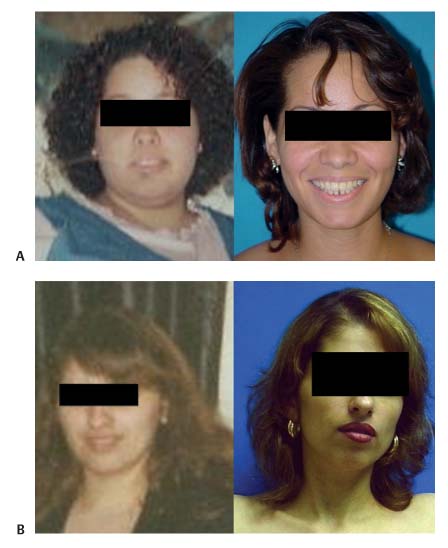
The age of the patient at the time of weight loss also can have a greater effect on facial changes after weight loss than on other parts of the body, as patients younger than 40 to 45 years of age may have significant skin contraction that results in little or no visible deformity in the face and neck. Patients older than 45 years of age begin to show relaxation of the neck and midface. The degree of relaxation increases with age and the volume of weight loss ( Figs. 33.1, 33.2, 33.3, 33.4 , and 33.5 ).
We provide a systematic approach to the evaluation of MWL patients undergoing facial rejuvenation, including key elements in the work-up, diagnosis, and treatment of these patients.


Medical History
As with all patients, a very careful and thorough consultation with the patient seeking facial rejuvenation should be conducted. This is critically important in the MWL patient. Many of these patients have complicated medical and surgical histories, and thus may require significant time and attention. Nutritional, metabolic, anesthetic, and psychological considerations have been discussed in earlier chapters of this textbook.
Of the utmost importance is the need to understand the goals and expectations of the patient seeking a facial procedure. Many of these patients have been shown to have mood disorders and a body dysmorphic disorder.1 It is essential to ensure that the patient’s expectations are consistent with the surgical plan and known outcomes.
Many patients are concerned about the overall prematurely aged appearance of their face. Patients may ask surgeons simply to make them “look younger.” But some patients will specify the deformities that bother them and state clearly their desired outcome. For example, some patients may want a reduction in the fullness and excess skin of the neck. It is important to extract as much detail and information about each area of complaint so as to prepare a sound surgical plan.

Once the patient’s concerns and expectations have been addressed, it is important to establish the method of weight loss, whether it was by gastric bypass, laparoscopic banding, or diet and exercise. This information, along with the patient’s age, will guide further questions about the patient’s medical and surgical history. The use of nutritional supplements, anemia, other associated procedures, and the occurrence of complications should be investigated. The maximum weight, total weight loss, and chronology of weight loss should be elucidated. In general, patients continue to lose weight many months after their surgery. They should be stable in their weight for at least 6 months before undergoing any facial procedures because their appearance may change if weight loss continues. Most patients will have undergone other body modification procedures before concentration on facial rejuvenation.
The past medical and surgical history should be reviewed. Questions about allergies, medications, family history, and smoking should be pursued. The patient’s responses to prior weight loss surgeries, including attendant anesthesia, should be explored. This review facilitates the surgeon’s identifying all tests and follow-up information needed for the preoperative work-up. In addition, a thorough review of all these issues will identify if there are any possible contraindications to surgery, such as smoking.
Examination
The face of an MWL patient is best examined alongside pictures of the face taken before the weight loss occurred. Therefore, patients should be instructed to bring old photographs to the consultation. New pictures should be taken of the face according to standard recommendations.2 This enables the surgeon to compare and contrast the findings on physical exam. In addition, it enables the patient to better explain his or her concerns. This is an invaluable tool that will greatly enhance the surgeon’s overall examination and surgical planning.
One of the most common findings after MWL is the appearance of a “gaunt” face ( Fig. 33.4 ). The midface and the cheek areas display a loss of volume secondary to the weight loss. In the older patient, in addition to the loss of volume, there is descent of the residual malar fat pad, accentuating the prominence of the malar eminence and lateral orbital rim, and deepening the nasolabial folds and marionette lines. These findings may be accentuated by prominence of the malar eminence and lateral orbital rim. Massive weight loss may also result in temporal hollowing, which exacerbates this appearance. Therefore, examination of the face begins with a careful analysis of the upper face, midface, lower face, and neck for signs of volume loss. Areas of inadequate volume, or reduced volume compared with the patient’s pre–weight-loss appearance, should be carefully noted.

Massive weight gain, with its proliferation of adipose tissue, creates skin expansion throughout the body, including the neck. Although MWL results in loss of adipose tissue of the neck, the neck skin after 45 years of age often does not contract sufficiently to redrape over the new neck contour ( Fig. 33.2 and Fig. 33.3 ). The neck should be examined for the presence of excess skin. The platysma should be examined for banding and diastasis. The amount of fat should be assessed. Prominence of the submandibular glands is documented.
Some MWL patients may have the appearance of decreased chin projection. This may be due to an obtuse cervicomental angle that obscures the prominence of the chin. This area should be carefully examined. If there is a suggestion of decreased chin projection, facial measurements should be taken. This helps confirm microgenia, if present.
These patients may also have early signs of jowling, prominent nasolabial folds, and laxity of the facial skin, depending on their age. The presence and extent of these changes should be documented. Older patients who have undergone MWL have more advanced stages of these changes. Younger patients who underwent their weight loss earlier may not yet have these findings. We have observed that skin contraction in patients younger than 40 to 45 years of age may be sufficient to decrease the incidence of the aforementioned facial deformities; these patients may not require much or any facial rejuvenation surgery as a result ( Fig. 33.5 ).
There is very little subcutaneous tissue in the eyelids. Thus, this area is not as profoundly affected as other regions of the face. Findings on examination of the eyelids are usually consistent with the findings in any other individual in the patient’s age group, irrespective of weight change. It is rare to see excess skin or even excess fat in the eyelid pockets that is out of proportion to age.
Similarly, the forehead skin has relatively little subcutaneous tissue. As a result, most patients have forehead rhytides and brow ptosis consistent with their age group. Massive weight loss usually has little influence on the appearance of this area of the face. Compensated brow ptosis should be excluded.
The nose is an overlooked area of facial rejuvenation. A full exam of the nose should be completed. Nasal tip ptosis and a resulting acute nasolabial angle occur with aging in general and not specifically with weight loss. Minor improvements of the nose may synergistically improve the entire appearance of the face.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


