32 Superomedial Vertical Breast Reduction
Summary
A true superomedial pedicle vertical breast reduction provides a breast with a good long-lasting shape. The inferior wedge principle avoids a boxy breast shape because there is good control of the horizontal base diameter of the breast. The vertical elliptical excision gives the breast good projection. Removal of the inferior breast tissue prevents bottoming out by avoiding the effects of gravity on the lower pole.
Key Teaching Points
Remove excess where it is inferior and lateral.
The true superomedial pedicle has a dual axial blood supply.
Blood supply is in the subcutaneous tissue, so the pedicle can be debulked for easier inset.
Use the Wise pattern for parenchyma to leave behind, not the skin.
Mark the nipple about 8 to 10 cm below the upper breast border.
Keep the vertical skin excision at least 4 cm above the inframammary fold.
There should be no tension on the pillar closure.
There should be no tension on the skin closure.
The vertical skin closure should not be cinched or gathered.
Liposuction is used to tailor out the resection beyond the Wise pattern.
The (true) superomedial vertical breast reduction technique provides a simple, reliable method to achieve good, long-lasting results. The pedicle has a dual axial blood supply and the procedure allows the surgeon to remove the unwanted breast tissue and leave the desired parenchyma.
Surgical Plan
Assess patient’s problem and desires.
Assess chest deformities/asymmetries.
Assess patient’s footprint.
Assess breast size and asymmetry.
Assess amount of glandular ptosis.
Assess amount of nipple ptosis.
32.1 Assess Patient’s Problem and Desires
Different patients are looking for different results. It is important to listen first in order to best manage patient expectations. Bra sizes are confusing at best and discussion of desired size is better discussed using photographs. A 36C is the same cup size as a 34D which is the same cup size as a 32DD or 32E. What used to be called a “C” is now called a “D.” The band size is dependent not only on the chest measurements but also on how apart the breasts are. The bra cups are closer together on the brassieres with the smaller bands. Patients need to be prepared for possible loss of sensation in both the nipples and the breast skin and they need to be prepared for possible inability to breast-feed.
32.2 Assess Chest Deformities/Asymmetries
Chest wall deformities such as pectus excavatum and pectus carinatum will affect the results. Scoliosis can affect the chest wall shape and orientation. Many patients are not aware of their asymmetries and it is best to make sure that this is discussed preoperatively.
32.3 Assess Patient’s Footprint
Breasts are attached to the chest wall in a variety of patterns. The breast footprint on the chest is like the footprint of a house on a lot. The footprint needs to be assessed both vertically and horizontally. There can be a significant difference from one side to the other.
The upper breast border (UBB) (junction of chest and breast) will not change with a breast reduction.
The lower breast border (inframammary fold[IMF]) can rise when the weight is removed.
The medial breast border (cleavage) can be improved with the control of the horizontal base diameter of the superomedial pedicle vertical techniques.
The lateral breast border can be improved with removal of excess parenchyma either directly or with liposuction.
Clinical Pearl
Understanding variations in the breast footprint allows the surgeon to predict results and manage patient expectations.
32.4 Assess Breast Size and Asymmetry
Patients often do not know which breast is larger and it helps if they are asked to pay attention before surgery to which breast overflows their brassiere the most. Breast asymmetries become more obvious when the patient holds her arms above her head.
Clinical Pearl
Breast asymmetries become more obvious when the patient holds her arms above her head.
32.5 Assess Amount of Glandular Ptosis
Glandular ptosis is the amount of excess breast parenchyma that hangs below the ideal breast size and shape. The IMF may be high or low and it is often different from side to side. It is not the ideal landmark because it is so variable. The UBB does not change with a breast reduction; it is a better landmark for determining ideal breast shape and nipple position.
32.6 Assess Amount of Nipple Ptosis
Nipple ptosis is how low the nipple is compared to the ideal position on that size of breast. Traditionally, the IMF is used as a landmark for the ideal nipple position, but the IMF can be misleading because it is so variable. The ideal nipple is about 8 to 10 cm below the UBB (which does not change postoperatively). The ideal nipple position will vary depending on the final desired breast size. A nipple, which is too high, can be quite bothersome for a patient if the areola slides up over the edge of the brassiere or bathing suit. It is always best to place the new nipple slightly lower than the horizontal midline of the breast. It is easier to raise a nipple, which is too low on the breast mound than it is to lower a nipple which is too high on the breast mound. When analyzing postoperative results, it can be seen that the nipples that are determined to be too high are too close to the UBB.
Clinical Pearl
It is best to assess nipple and glandular ptosis as separate considerations. The upper breast border is a better landmark than the inframammary fold for determining how much glandular ptosis to remove and where the new nipple position should be.
32.7 Markings
This 53-year-old woman presented for a breast reduction. Note that folding up (not pushing up) her breast will show the UBB where the skin creases. She was 5 feet 9 inches tall and weighed 140 pounds (▶Fig. 32.1a,b).
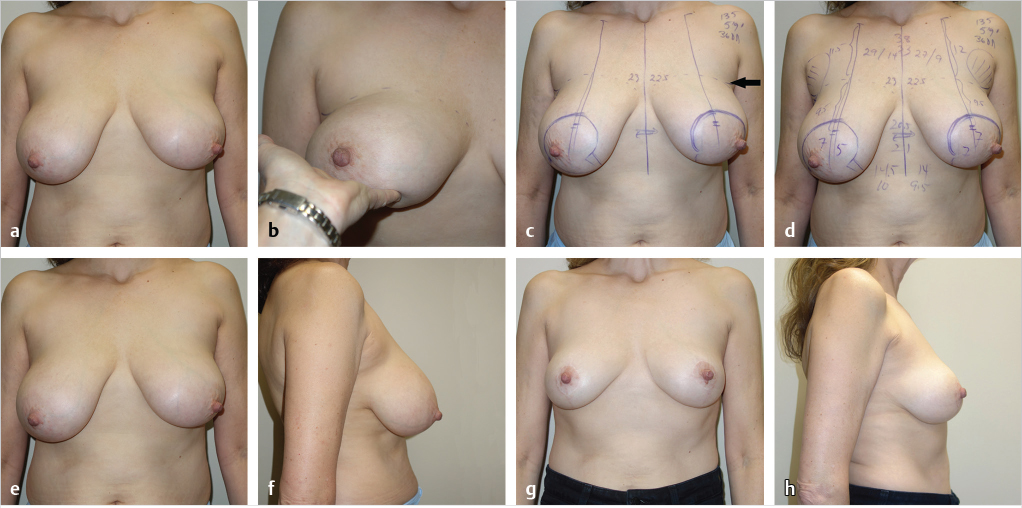
32.7.1 The Upper Breast Border Is Marked with a Dotted Line
The UBB is at the junction of the preaxillary fold and the breast at the level of the indentation. In this case, the new nipple position was close to the same level as the IMF.
32.7.2 The Breast Meridian Should Be Drawn in Its Ideal (Not Existing) Nipple Position
This patient had very lateral nipples. Note that the new breast meridian is drawn where the nipple should be and not where it is. The new nipple position was marked at 9.5 cm below the UBB. It is important to mark the nipple slightly lower on the larger breast. This is probably because closure of a wider ellipse will push the nipple up higher (▶Fig. 32.1c,d).
Clinical Pearl
The new breast meridian should be drawn in its ideal location—not necessarily in its existing location.
32.7.3 The top of the areola was marked at 2 cm above the new nipple position.
It is important to mark the medial aspect of the areola in the ideal position and the lateral aspect can vary in order to go outside the areolar borders. The new medial borders need to be symmetrical side to side.
The new areola will stretch to fit the skin opening (the actual size of the cookie cutter is less important).
A 16-cm areolar opening will fit a 5-cm diameter areola. A 14-cm areolar opening will fit a 4.5-cm diameter areola. It is better to take excess skin out vertically to prevent stretching of the final areola.
32.7.4 The vertical limbs are not much different from an inverted-T type pattern.
The breast can be rotated medially and laterally and the vertical limbs can be matched up to the chest meridian the way Marchac, Lassus, and Lejour described. The vertical limbs for an inverted T, inferior pedicle breast reduction tend to be a bit wider because the skin is used as a brassiere. The superomedial vertical breast reduction relies on parenchymal reshaping after excision of parenchyma where it is in excess; it is not a skin brassiere operation so it is important not to take out too much skin. She had 230 g removed from her right breast and 190 g from her left breast. She had another 150 cc of fat removed by liposuction. She is shown at 18 months after her breast reduction (▶Fig. 32.1e–h).
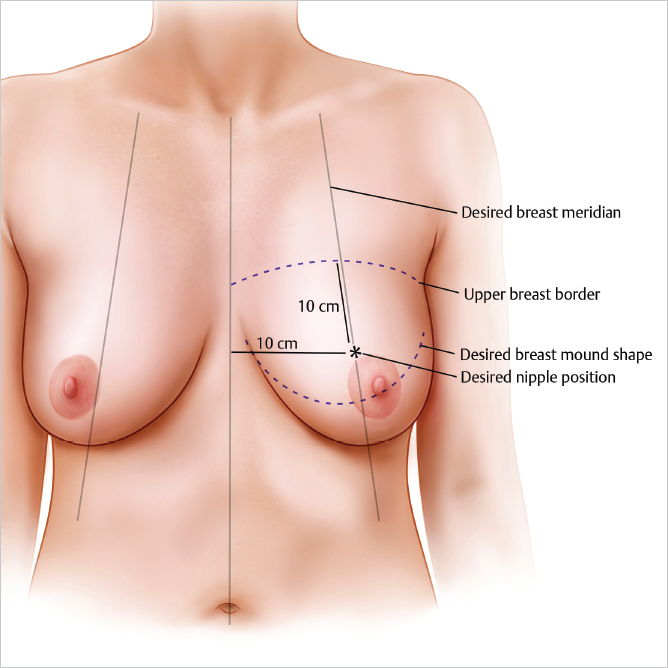
The ideal nipple position on an “average” “C” cup breast is about 10 cm down from the UBB and about 10 cm from the chest midline (10 cm as drawn with a straight ruler—not measured around the curve of the breast) (▶Fig. 32.2).
32.8 Surgical Procedure Superomedial Pedicle Vertical Breast Reduction
This 65-year-old patient presented for a breast reduction. She was 5 feet 5 inches tall and weighed 175 pounds.
Note that the UBB is marked. The left breast was larger and it is marked with a star. The new breast meridian is marked where it should be—slightly medial to the left nipple but at the same position as the right nipple. The right breast meridian is 10.5 cm from the chest midline and the left breast meridian is marked at 11 cm from the chest midline. The new nipple position is marked at 10 cm below the UBB on both sides. Note that the new nipple position is marked higher in this patient than the (asymmetrical) IMFs. The UBB is a better landmark for new nipple position than the IMF (which can be misleading) (▶Fig. 32.3).
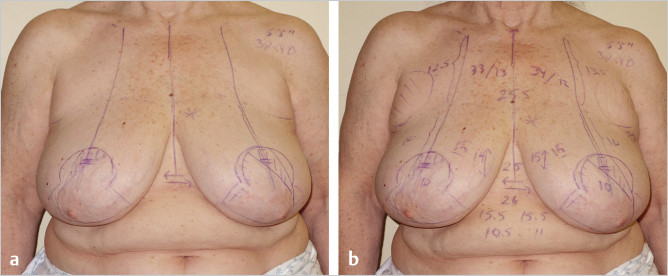
The breast base diameter is 15.5 cm on both sides (the ideal breast base diameter is usually 11–14 cm). The new areolar opening measures 15 cm on both sides (so the new areola will measure just < 5 cm). The vertical limbs are 14 and 15 cm long.
Clinical Pearl
The new areolar diameter will depend more on the length of the skin opening than it does on the diameter of the cookie cutter.
Related posts:
 33 Superomedial Pedicle Technique with Inverted-T Closure (Wise Pattern)
33 Superomedial Pedicle Technique with Inverted-T Closure (Wise Pattern)
 34 Central Mound Inferior Pedicle Technique
34 Central Mound Inferior Pedicle Technique
 36 Outcomes and Reducing Complications in Breast Reduction
36 Outcomes and Reducing Complications in Breast Reduction
 35 Free Nipple Graft Technique
35 Free Nipple Graft Technique
 37 Gynecomastia: Evaluation and Treatment
37 Gynecomastia: Evaluation and Treatment
 31 Vertical Superior Pedicle Breast Reduction (Modified Lassus Technique)
31 Vertical Superior Pedicle Breast Reduction (Modified Lassus Technique)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


