30 Anterior Proximal Extended (APEX) Medial Thigh Lift

Abstract
Thigh lifting has been one of the most challenging procedures in body contouring after weight loss, in part due to often disappointing results and high complication rates. Advances in the understanding of thigh anatomy, including the importance of the superficial fascial system, have contributed to more successful, safer, and longer-lasting techniques in thigh lifting. This chapter describes the approach used at Johns Hopkins to medial thigh lifting in the massive weight loss patient. Our preferred technique in the majority of patients is termed the anterior proximal extended (APEX) thigh lift. In this technique, the thigh flaps are secured to periosteum, with the incisions extended anteriorly into the lower abdominal area and posteriorly into the infragluteal creases. In patients with excessive distal-third of the thigh skin laxity, a vertical thighplasty is often performed. For patients demonstrating significant lipodystrophy of the thigh, liposuction can be added as a separate stage prior to thigh lifting. The most prevalent complications are wound-healing problems, infection, lymphedema, and lymphocele formation. We have found our technique to be safe and effective, improving not only thigh contour but also harmony with adjacent body regions, including the gluteal areas.
Introduction
Thigh lift is one of the most challenging procedures to perform for massive weight loss (MWL) patients. Thigh presentation in MWL is highly variable from patient to patient, with different degrees of skin laxity, quality, and redundancy; subcutaneous lipodystrophy; venous incompetency and varicose veins; and lymphedema. The lower extremity is also highly dynamic and prone to gravitational forces, increasing the risk of poor surgical outcomes with regard to healing, edema, and thromboembolism.
History of Thigh Lift
Thigh lifting has been a topic of interest since Lewis1 published his paper in 1957. Although MWL has catalyzed growing interest and publication regarding thigh lift, the components of the thigh addressed in this procedure have remained unchanged over the past 50 years. Furthermore, elements of current concepts, such as vertical thigh lifting and proximal anteromedial techniques, may be traced back to the earlier literature. Lewis1,2 advocated in the 1950s and 1960s wide elliptical excision of the medial thigh along the inguinal crease with vertical extension into the medial thigh. Pitanguy3 in 1964 described extensive dermatolipectomy for correction of trochanteric lipodystrophy and the ptotic inner thigh, bringing an incision from the lateral buttock at the fascia lata across the gluteal fold, ending anteriorly in the medial thigh. This technique was further elaborated upon by Hoffman and Simon,4 who described significant morbidity associated with the procedure with a prolonged recovery period, as well as the less substantial results for the medial thigh relative to the trochanter. Schultz and Feinberg5 described a medial thigh lift from the inguinocrural crease to the gluteal crease, using lithotomy positioning, without suspension sutures. Vilain and Dardour6 utilized an approach from the anterior medial thigh into the gluteal crease, also without suspension. More recent evolution in technique emphasizes treatment of skin laxity over lipodystrophy.
Contemporary Thigh Lift
Lockwood7,8 popularized thigh lifting in the contemporary literature. Importantly, he defined the functional anatomy of the superficial fascial system (SFS) in the region of the thigh to allow suspension of tissues, as well as zones of adherence from SFS attachments to the skin requiring release to allow optimal lifting.8 In his technique, conservative skin resection is performed in combination with undermining and liposuction, and hiding the scar in the groin crease. Lifting is accomplished by approximating the superficial fascia of the thigh to Colles’ fascia in the groin, achieving a vertical pull. This suspension was performed to counteract inferior wound migration, scar widening, vulvar traction, and recurrent ptosis. The technique incorporated thigh lift into lower body lifting, including abdominoplasty and lower back lift. Lockwood cautioned against extending the thigh lift scar into the infragluteal fold and suggested limiting skin resection to 5 to 7 cm. Although remarkable results have been demonstrated, the applicability of this procedure to MWL patients has been inadequate due to limited skin removal and the risk of scar migration from dependence on attenuated tissue, leading to the potential risk of labial spread and the need for revisions. Further, a segment of the MWL population tends to house more subcutaneous fat in the thigh than the standard Lockwood patient.

Due to the limited applicability of the Lockwood thigh lift to MWL patients, more surgeons have turned to vertical, extended thigh lift.9–12 This technique involves removal of medial thigh tissue from the groin to the knee through a vertical incision, converting the axis of pull from vertical to horizontal. There is no reliance on suspension of fascial tissues that might fail due to attenuation, decreasing the risk of recurrent ptosis and vulvar traction. It is important to avoid injury to the saphenous vein and lymphatics to prevent lymphedema.
There is heterogeneity in the vertical, extended thigh lift techniques described by different authors. Several surgeons discuss the benefit of using liposuction to prevent injury to lymphatics and veins, while also improving contour.9,13 Other surgeons caution against the use of liposuction in body regions undergoing excision, recommending that surgery be staged in these cases, with liposuction designated as the first stage. All agree that vertical thigh lifting provides the best outcome for patients with significant skin laxity and poor skin quality extending to, and beyond, the knee ( Fig. 30.1 ). In exchange for the dramatic results, the patient accepts a visible scar with a risk of irregularity in the junction between the anterior and posterior thigh, as well as the accompanying risks of lymphedema and lymphoceles9,14,15 ( Fig. 30.2 ).

Technique
Thigh Lift with a Hidden Scar in Massive Weight Loss Patients: The APEX Thigh Lift
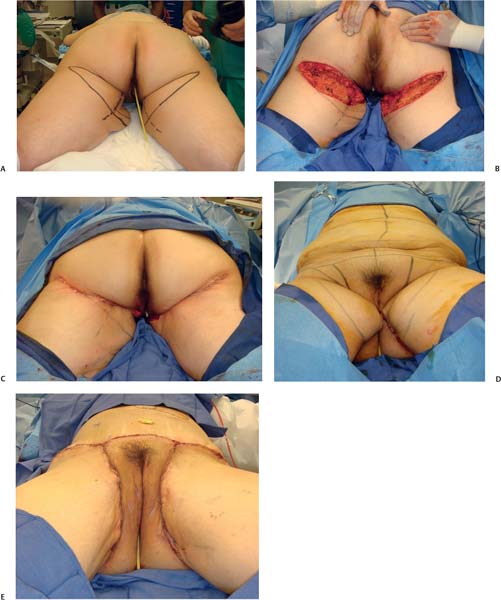
Although the greater power of the vertical, extended medial thigh lift can be appreciated, many MWL patients do not have poor skin quality or exaggerated skin redundancy along the length of the thigh requiring a visible scar with potential injury to venous and lymphatic structures. We have worked to extend the Lockwood medial thigh lift to improve its utility in the MWL population. We have extended the anterior inguinal crease incision posteriorly into the infragluteal fold with suspension of posterior thigh skin to the ischial periosteum, and have extended the superior portion of Lockwood’s incision into the abdominal incision, superior to the level of pubic suspension of anteromedial thigh skin ( Fig. 30.3 ). This technique has been named the APEX thigh lift; APEX stands for anterior proximal extended approach.16 The APEX thigh lift has increased the degree of skin excision and pull beyond that of Lockwood’s technique, while maintaining a scar that is hidden even in revealing clothing. The key to this procedure, which sets it apart from other thigh lifts with similar incisions, is the suspension to the periosteum posteriorly and anteriorly. A further advantage of this technique is the secondarily improved appearance of the buttock, removing the inner thigh and infragluteal skin that blunts the aesthetic contour of the medial inferior buttock17,18 ( Fig. 30.4 ).

Some authors describe combining the Lockwood medial thigh lift with vertical extension for patients with laxity extending distal to the upper third of the inner thigh.12 The drawback of this technique is disruption of the breakpoint in the upper thigh at the junction of the distal portion of the thigh, effectively disturbing the lower extremity aesthetic unit ( Fig. 30.5 ).
There is a subgroup of patients who have sustained MWL who demonstrate skin laxity but still have disproportionate significant lipodystrophy. The plan is to treat these patients in two stages: the first stage is liposuction, and the second stage is vertical thigh lift after appropriate deflation has been achieved ( Fig. 30.6 ). In actuality, it is rare for these patients to present for both stages, for financial reasons or due to failure to maintain adequate weight loss.

Related posts:
 28 Spiral Thigh Lift
28 Spiral Thigh Lift
 29 Fascio-Fascial Suspension Technique for Medial Thigh Plasty
29 Fascio-Fascial Suspension Technique for Medial Thigh Plasty
 32 Combination Circumferential Abdominoplasty with Medial Thigh Lift
32 Combination Circumferential Abdominoplasty with Medial Thigh Lift
 31 Medial Thigh Contouring: Cones and Cylinders
31 Medial Thigh Contouring: Cones and Cylinders
 4 Anesthesia and Safety Considerations in the Perioperative Period
4 Anesthesia and Safety Considerations in the Perioperative Period
 36 Facial Rejuvenation: Open Technique
36 Facial Rejuvenation: Open Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


