31 Medial Thigh Contouring: Cones and Cylinders
Abstract
Medial thigh contouring is an integral part of the body-sculpting continuum. Patients often present with functional concerns, including rash and skin breakdown, as well as cosmetic ones. Early techniques for medial thigh lifting were met with disappointment and with an unacceptable rate of complications, including wound dehiscence, scar migration and hypertrophy, flap necrosis, infection, and recurrent ptosis. Refinements in the technique, including a suspension of the superficial fascial system, have revolutionized the procedure. Medial thigh deformities can be classified as cone shaped or cylinder shaped, depending on the degree and location of skin excess. The majority of deformities can be treated using a transverse excision in the upper thigh only, but cylindrical thighs with severe skin excess require a vertical incision to the knee area. The technique includes undermining of the thigh flap superiorly, combined with discontinuous inferior undermining using liposuction, resuspension of the superficial fascial system, and limited direct undermining of the thigh flaps. With proper classification of the preoperative deformity and appropriate choice of the surgical approach, the operation can result in a satisfactory outcome.
Introduction
In the past decade, advances in surgery and surgical outcomes have led to an exponential rise in the number of patients seeking to undergo bariatric surgery. As bariatric surgery becomes more common, the plastic surgeon is more frequently called upon to deal with the results of massive weight loss that wreak havoc on a patient’s body habitus.
Not surprisingly, these patients have routinely lost massive amounts of weight but are left draped with loose, ptotic skin on their trunk, arms, and legs. This has led to numerous procedures that are very effective in addressing this skin laxity, but usually at the expense of visible scarring. A prime example of this is the medial thigh. Post–bariatric surgery patients have a significant functional morbidity from excess medial thigh skin, including skin breakdown and intertrigo in the inguinal creases and thigh creases, as well as potential disabilities in ambulation. However, patients often find that solutions involving a long visible scar along their inner thigh are aesthetically unacceptable. The lateral thighs and hips are usually addressed through a lower body lift in an earlier stage of body contouring.
The medial thigh lift was introduced in 1957 by John Lewis.1,2 The initial designs included a vertical incision, placed posteromedially to make the scar as inconspicuous as possible. In 1971, Pitanguy3 described a horizontal incision hidden in the bathing-suit line. The medial thigh lift operation has historically been met with some resistance due to dissatisfaction with scarring and other associated complications, namely seromas, infections, skin necrosis, distortion of the labia, and high recurrence rate. Descriptions of the superficial fascial system by Lockwood4,5 and a superficial fascial anchoring technique contributed to significant advancement in the medial thigh lift and a considerable decrease in complications. Further refinements in the technique of this surgery have limited some of the complications. These include minimizing dissection in the region of the femoral triangle to avoid lymphatic disruption, utilizing the superficial fascial system to support the tension of the repair, and thoughtful incision placement to avoid tension on the labia and pubic region.

Indications
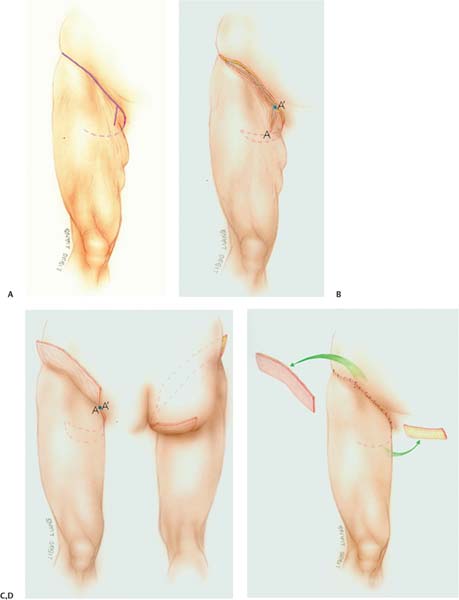
An algorithm of medial thighplasty must consider differences in patients’ anatomy. With experience, we have noted two basic shapes of the thigh that result after weight loss: a funnel or cone shape, and a cylinder shape ( Figs. 31.1 and 31.2 ). The cone shape consists primarily of superior or proximal excess with little to no distal excess skin. In these cases, medial thigh contouring with a horizontal excision without a vertical excision can allow for a circumferential tightening of the thigh while avoiding a vertical medial thigh scar down to the knee, which is much less aesthetically pleasing. Patients with cylinder- shaped thighs, on the other hand, present with significant horizontal and vertical excess skin with ptosis that extends down to the knee. In these cases, it has been found that both the horizontal and vertical excisions are necessary for the optimal result. We reserve the vertical excision for patients with severe skin excess distally to the knee, as redraping after a horizontal excision is sufficient for the majority of deformities.
Initially, we combined wide undermining of the medial thigh flap with liposuction along the medial thigh to the knee. Experience demonstrated that this resulted in vascular compromise that caused a higher than desired rate of me-dial thigh wound edge necrosis, dehiscence, and infection. As a result, we now perform a more limited medial thigh flap dissection with liposuction. The complication rate has decreased noticeably with this modification, as blood supply is more preserved. The discontinuous undermining with liposuction allows for redraping of the medial thigh flap as well as recontouring by fat excision.

As in any surgery, patient selection is important. As with other stages of body contouring, we reserve surgery until the patient’s weight is stable for a period of at least 6 months. A full medical work-up in conjunction with the primary care physician is conducted preoperatively to ensure that the patient’s general health and cardiac status are optimized. Contraindications to this particular surgery include peripheral vascular disease, lymphatic disease, and active smoking.
Related posts:
 28 Spiral Thigh Lift
28 Spiral Thigh Lift
 29 Fascio-Fascial Suspension Technique for Medial Thigh Plasty
29 Fascio-Fascial Suspension Technique for Medial Thigh Plasty
 30 Anterior Proximal Extended (APEX) Medial Thigh Lift
30 Anterior Proximal Extended (APEX) Medial Thigh Lift
 32 Combination Circumferential Abdominoplasty with Medial Thigh Lift
32 Combination Circumferential Abdominoplasty with Medial Thigh Lift
 4 Anesthesia and Safety Considerations in the Perioperative Period
4 Anesthesia and Safety Considerations in the Perioperative Period
 36 Facial Rejuvenation: Open Technique
36 Facial Rejuvenation: Open Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


