3 Scar Revision
Introduction
The purpose of scar revision is to optimize scar camouflage. Although scar appearance can in many circumstances be improved, a scar cannot be completely removed. Patients should be informed as such. The ultimate appearance of a scar is dependent on many factors. The orientation of the scar, amount of tissue loss or injury, scar position on the face, age of the patient, patient’s underlying health, genetic predisposition to abnormal scar formation, technique of wound closure, and presence of wound healing complication all contribute to the final scar result. Scar position, extent of tissue loss, patient age, genetic factors, and underlying health are for the most part beyond a surgeon’s control. However, the surgeon can implement specific wound healing and scar formation principles in the surgical planning to effect an optimal outcome for the patient.
Understanding the mechanism of scar formation can be helpful in deciding on the method of scar revision. Blunt trauma, gunshot wounds, and burn scars tend to involve a larger surrounding area of injury than surgical incisional scars. Initially, it may be difficult to determine how much of the adjacent soft tissue is not viable, especially in wounds associated with thermal injury. Debridement during the initial stage of repair should be conservative to preserve as much viable tissue as possible. Scars resulting from these types of injuries may be less amenable to a satisfactory result or may require staged revisions.
There are some guidelines for optimizing initial scar formation, which in turn may facilitate later scar revision or even circumvent the need for a secondary procedure. All wounds should be as clean as possible, with removal of foreign bodies. Irrigation with sterile saline has been shown to decrease bacterial counts. Clearly devitalized tissue should be debrided with preservation of healthy tissue. The orientation of the scar should not necessarily be altered during the initial injury because scar irregularities may serve to help camouflage the scar, and neighboring tissues can be observed for viability and preserved for any required secondary procedures. During initial closure of traumatic injuries, soft tissues should be closed in multiple layers if the injury penetrates the subcutaneous tissues. Conservative undermining may be necessary to approximate wound edges without tension. Tension increases the risk for widened or hypertrophic scars. The wound surface should be kept moist with antibiotic ointment or an occlusive dressing.
Scar Analysis
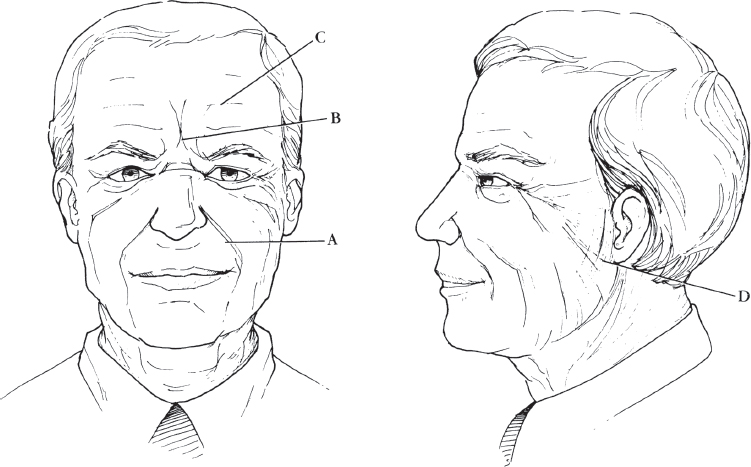
The ideal scar is narrow, flat, and level with the surrounding skin. It has similar color match to the surrounding skin. The scar should be parallel or within the relaxed skin tension lines (RSTLs) ( Fig. 3.1 ) and possibly in a junction between aesthetic subunits. The scar should not tent or bunch up the surrounding skin. Scar revision is indicated for scars that are hypertrophic, widened, depressed, perpendicular to RSTLs, webbed, trapdoor, causing malalignment of a facial landmark (brows, vermilion), or interfering with facial function. Scars that are narrow, within the RSTLs, but hypertrophic may respond to intralesional triamcinolone injection alone ( Fig. 3.2 ). The tendency for a patient to develop hypertrophic scars and keloids may be evident from prior sites of injury or incisions. Therefore, it is wise to examine all sites of old scars or wounds to identify and mitigate risks for abnormal scar formation when necessary.
Timing of Scar Revision
All scars tend to improve spontaneously after a period of maturation of 1 year. However, the patient frequently wishes for earlier intervention, if warranted. The characteristics of a scar can help guide the timing of the scar revision. If a fresh scar is narrow, flat, situated within the RSTL, but erythematous, it may serve the patient better to reassess the scar after it matures because erythema usually dissipates. However, if the scar has significant unfavorable characteristics, such as malalignment, which will usually not improve with time, then earlier scar revision may be beneficial.
Minor revisions, such as dermabrasion and laser therapy, may be routinely performed ∼8 weeks after the initial wound repair. Dermabrasion during this early period of wound healing may in theory benefit from the high fibroblast activity. At this time scars are usually still erythematous. Dermabrasion itself causes significant transient erythema. Therefore, early dermabrasion may decrease the total time that a patient has to endure an erythematous scar by overlapping the erythematous periods associated with early scar healing and dermabrasion. In cases of hypertrophic scars and keloids, early treatment with a pulsed dye laser to flatten the scar and reduce the associated erythema, itching and burning sensation may be helpful. In addition, Q-switch laser can help reduce the hyperpigmentation seen in these scars. Dermabrasion and laser therapy can also be performed in chronic or mature scars as well.
Excisional Techniques
Scar Repositioning
Frequently scars can be repositioned to fall within RSTLs, borders between aesthetic units, or hairbearing scalp. Scar repositioning requires the scar to be in proximity to the more hidden site. This concept can be applied to the facelift or postparotidectomy patient who has a noticeable preauricular scar. Often these scars can be repositioned close to the tragus, resulting in better camouflage ( Fig. 3.3 ). Scars that cause malalignment of an aesthetic landmark can be excised and repositioned.

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


