29 Fascio-Fascial Suspension Technique for Medial Thigh Plasty
Abstract
Thigh lifting is indicated in the treatment of redundancy of tissue in the upper two thirds of the medial thigh. Deformity of the medial thigh is a very common problem, with patients often complaining about it, but medial thigh lifting is a seldom-used procedure because of historic postoperative problems, such as inferiorly displaced and widened scars, vulvar distortion, and early recurrence of ptosis. To provide stronger support to the thigh flap, we have developed a deep-anchoring technique based on overlap of the adductor longus and gracilis fasciae. This fascio-fascial suspension allows for strong vertical support with minimized tension on the skin, thereby obtaining a predictable improvement of the redundant medial thigh that is commonly seen in patients after massive weight loss. The deep anchoring contributes also to minimizing the early and late complications traditionally associated with this procedure.
Introduction
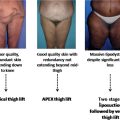
In massive weight loss patients, aesthetic deformities of the medial thigh are the result of redundant and loose skin, which also can be associated with localized adiposity, especially in the proximal third. When skin tone is adequate and the primary problem is bulging fat, liposuction alone can efficaciously correct the problem. On the other hand, in those patients with a large amount of redundant skin and poor skin tone, as commonly seen in patients after massive weight loss, medial thigh lifting is usually required.
Many techniques of medial thigh lifting have been described in the past, with older methods being limited to the simple resection of an oblique ellipse of skin and fat from the inguinal fold.1–8 In 1977, Agris1 suggested the use of a dermal-fat suspension flap for thigh and buttock lifting. In the thigh, the de-epithelialized suspensory flap was sutured directly to the inguinal fascia and buried with a vest-over-pants closure. A step forward to more stable results was the introduction of deep anchoring of the distal flap to fixed anatomic structures, such as Colles’ fascia. In the fascial anchoring technique introduced by Lockwood5 in 1988, resection of a crescent of redundant skin and fat in the superior medial thigh is followed by suspension of the distal skin flap to Colles’ fascia of the perineum, an inelastic and strong anatomic structure. Subsequently, Lockwood9,10 combined the superficial fascial suspension with a new flank-thigh- buttock lift design that allowed a wider transverse skin and fat resection with less noticeable scarring. Despite these most recent modifications, thigh lifting has never gained widespread acceptance because of high rates of postoperative complications, such as inferiorly displaced and widened scars, vulvar distortion, and early recurrence of ptosis. In 1995, we developed a different deep-anchoring technique based on overlapping of the adductor longus and gracilis fasciae, which constitutes our favored approach, both in patients seeking surgery for aesthetic reasons and in massive weight loss patients.11
Relevant Anatomy
The gracilis and adductor longus fasciae constitute the me-dial portion of the inguinocruralis fascia, the lateral and the central portions being formed, respectively, by the sartorius fascia and the fascia cribrosa.12 The inguinocruralis fascia is fixed proximally to the ligamentum inguinale and continues into the surrounding fasciae (fascia glutea, fascia lata, and fascia perinealis). The deep layer of the superficial fascia of the perineum, Colles fascia, is a distinct connective tissue layer lying deep to the subcutaneous fat of the perineum.13 Laterally, it attaches to the ischiopubic rami, anteriorly it blends with Scarpa’s fascia of the abdominal wall, and posteriorly it fuses with the posterior border of the urogenital diaphragm. Colles’ fascia provides the anatomic shelf that defines the perineal thigh crease.13
Indications
Patient selection for this technique is based on an accurate preoperative examination of the thigh. A large amount of relaxed skin in the proximal third of the thigh is not a good indication because of destruction of the fibrous septa, which fixes the skin and subcutaneous tissue to the underlying fasciae. In these patients, wider subcutaneous undermining is suggested and a vertical scar should be incorporated to better address the laxity. Ideal patients for fascio-fascial suspension are those presenting with a moderate excess of skin in the proximal third of the medial thigh, with accompanying fat. Localized adiposity, in fact, is not a true contra-indication because liposuction can reduce the thickness of the flap while preserving the fibrous ligaments between the skin and fasciae.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


