Arthropod Bites, Stings, and Cutaneous Infections 
Cutaneous Reactions to Arthropod Bites 
 Arthropods are defined by an exoskeleton, segmented body, and jointed appendages. Four of 9 classes of arthropods cause local and systemic reactions associated with their bites: Arachnida, Chilopoda, Diplopoda, and Insecta.
Arthropods are defined by an exoskeleton, segmented body, and jointed appendages. Four of 9 classes of arthropods cause local and systemic reactions associated with their bites: Arachnida, Chilopoda, Diplopoda, and Insecta.
 Cutaneous reactions to arthropod bites are inflammatory and/or allergic reactions.
Cutaneous reactions to arthropod bites are inflammatory and/or allergic reactions.
 Characterized by an intensely pruritic eruption at the bite sites immediately to minutes to hours to days after the bite, persisting for days to weeks, manifested by solitary or grouped: Urticarial papules; papulovesicles; bullae. Persons are often unaware of having been bitten.
Characterized by an intensely pruritic eruption at the bite sites immediately to minutes to hours to days after the bite, persisting for days to weeks, manifested by solitary or grouped: Urticarial papules; papulovesicles; bullae. Persons are often unaware of having been bitten.
 Systemic symptoms may occur, ranging from mild to severe, with death occurring from anaphylactic shock.
Systemic symptoms may occur, ranging from mild to severe, with death occurring from anaphylactic shock.
 Arthropods are vectors of many systemic infections.
Arthropods are vectors of many systemic infections.
Arthropods that Bite, Sting, or Infest
Four of nine classes of arthropods cause local or systemic reactions.
1. Arachnida (four pairs of legs): mites, ticks, spiders, scorpions
a. Acarina. (mites and ticks) Sarcoptes scabiei (scabies). Demodex folliculorum and D. brevis (demodicidosis). Environmental mites. Ticks (Fig. 28-1) that feed on humans and are vectors for disease include blacklegged or Ixodes tick, lone star tick, and dog tick.
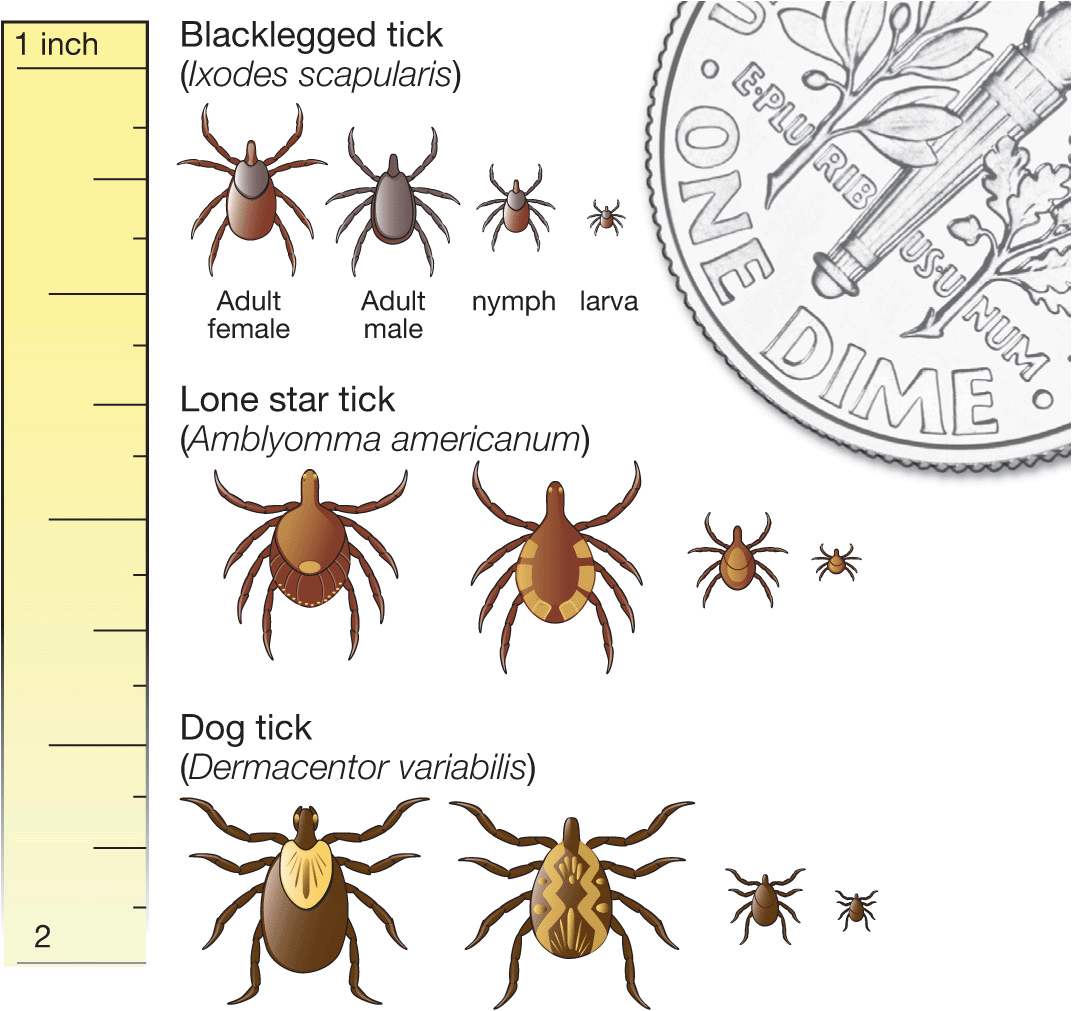
Figure 28-1. Comparison of blacklegged, lone star, and dog ticks Blacklegged or Ixodes nymphal ticks transmit Borrelia burgdorferi (Lyme disease) and other infections. Lone star ticks or Amblyomma americanum is the vector for anaplasmosis, tularemia, and Southern tick-associated rash illness. Dog or wood ticks, Dermacentor variabilis, transmit Rocky Mountain spotted fever and tularemia.
b. Araneae. (spiders) Loxosceles reclusa or brown recluse spider. Latrodectus or widow spiders. Tegenaria or hobo spiders cause necrotic arachnidism in Pacific Northwest of United States. Tarantula: Mild inflammatory response to bite and to shed hairs.
c. Scorpionida. Venom contains a neurotoxin that can cause severe local and systemic reactions.
2. Chilopoda or centipedes
3. Diplopoda or millipedes
4. Insecta (three pairs of legs)
a. Anoplura. Phthirius pubis or crab lice. Pediculus capitis or head lice. Pediculus corporis or body lice.
b. Coleoptera. Beetles. Blister beetles contain the chemical cantharidin, which produces a blister when the beetle is crushed on the skin.
c. Diptera. Mosquitoes, black flies (bites produce local reactions as well as black fly fever with fever, headache, nausea, generalized lymphadenitis), midges (punkies, no-see-ums, sand flies), Tabanidae (horseflies, deerflies, clegs, breeze flies, greenheads, mango flies); botflies, Callitroga americana, Dermatobia hominis, phlebotomid sand flies, tsetse flies
d. Hemiptera. Bedbugs, kissing bugs
e. Hymenoptera. Ants, bees, wasps, hornets
f. Lepidoptera. Caterpillars, butterflies, moths
g. Siphonaptera. Fleas, chigoe or sand flea
Arthropod-Borne Infections
• Lyme borreliosis, tularemia, bubonic plague
• Scrub typhus, endemic (murine) typhus, spotted fever groups, Q fever
• Human granulocytic anaplasmosis
• Tick-borne meningoencephalitis
• Leishmaniasis, trypanosomiasis (sleeping sickness, Chagas disease).
• Filariasis, onchocerciasis (river blindness), loiasis
Clinical Manifestation
Erythematous macules. occur at bite sites and are usually transient.
Papular urticaria or urticarial papules persistent for >48 h (Fig. 28-2, Fig. 28-3); usually <1 cm; vesicle may for on papule. Large urticarial plaques may occur.

Figure 28-2. Papular urticaria A 21-year-old male awoke with multiple pruritic erythematous papules on exposed of face, neck, forearms, and hands. Bedding was heavily colonized with bedbugs.

Figure 28-3. Papular urticaria A 6-year-old girl with multiple mosquito bites on face.
Bullous Lesions. Tense bullae with clear fluid on a slightly inflamed base (Fig. 28-4); excoriation results in large erosion.

Figure 28-4. Bullous insect bite A 10-year-old child with bullous lesions on the ventral wrist and popular urticarial on the forearm.
Secondary Lesions. Excoriations of urticarial, papular, vesicular lesions common. Painful erosion may be secondarily infected with Staphylococcus aureus. Excoriated or secondarily infected lesions may heal with hyper- or hypopigmentation and/or raised or depressed scars, especially in more darkly pigmented individuals.
Systemic findings may occur associated with toxin or allergy to substance injected during bite. Many varied systemic infections can be injected during bite.
Clinical Variations by Arthropod
Mites. Sarcoptes scabiei causes infestation scabies (see Scabies). Demodex folliculorum and D. brevis live in human hair follicles and sebaceous glands, causing demodicidosis (see Fig. 28-15).

Figure 28-5. Furuncular myiasis A pruritic papule at the site of deposition of a botfly larva, slowly enlarging over several weeks into a domed nodule (resembles a furuncle). The lesion has a central pore through which the posterior end of the larva (inset) intermittently protrudes and thus respires.
Food, fowl, grain, straw, harvest, and animal mite bites cause papular urticaria.
Food Mites. Cheese, grain, mold mites can cause mild contact dermatitis: baker’s or grocer’s itch. Straw mites. Bites occur during harvest season causing dermatitis; straw itch. Harvest mite: Chiggers. Bites can cause dermatitis. One species transmits Rickettsia tsutsugamushi, the cause of scrub typhus.
Dermatophagoides species of house dust mites are implicated in the pathogenesis of asthma and atopic dermatitis. Feed on desquamated human skin and other organic detritus, living in bedding, carpets, and furniture. Bodies and excreta may have a role in asthma and other allergies. Affected persons respond with production of IgE antibodies. Fowl mites. Chicken, pigeons, etc. Bites cause papular urticaria on exposed sites. Rat mites cause painful bites and dermatitis and transmit endemic/murine typhus. House mouse mite is the vector for rickettsialpox. Cheyletiella spp. (dog and cat mites) bite pet owners causing pruritic lesions on forearms, chest, and abdomen. Canine sarcoptic mange (S. scabiei var. canis) and feline mange (Notoedres cati) cause a pruritic dermatosis in pet owners.
Ticks. Ticks attach and feed painlessly. Secretions can produce local bite reactions (erythema), febrile illness, and paralysis. Blacklegged or Ixodes tick, lone star tick, and dog tick are vectors for diseases. Erythema migrans (Fig. 25-81), characteristic of primary Lyme disease or borreliosis, occurs at the bite site of an infected Ixodes tick that transmits Borrelia burgdorferi.
Lymphocytoma cutis (Fig. 25-82) also occurs at the site of bite of an infected Ixodes tick.
Spiders. Brown recluse spider bites can result in mild local urticarial reactions to full-thickness skin necrosis. Associated with a maculopapular exanthem, fever, headache, malaise, arthralgia, and nausea/vomiting. Most lesions diagnosed as brown recluse spider bites are bite reactions to other arthropods. Widow spiders inject a neurotoxin (α-latrotoxin) that produces bite site reactions as well as varying degrees of systemic toxicity.
Insects. Pubic lice, head lice, body lice papular urticaria, excoriations, secondary infections (see page 707).
Mosquitoes. Bites usually present as papular urticaria (Fig. 28-2) on exposed sites; reactions can be urticaria, eczematous, or granulomatous.
Black Flies. Anesthetic is injected, resulting in painless initial bite; may subsequently become painful with itching, erythema, and edema. Black fly fever characterized by fever, nausea, and generalized lymphadenitis.
Midges. Bites produce immediate pain with erythema at bite site with 2- to 3-mm papule and vesicles, followed by indurated nodules (up to 1 cm) persisting for many months.
Tabanidae or horse flies. Bites painful with papular urticaria; rarely associated with anaphylaxis.
Dermatobia hominis (human botfly) in tropical regions causes furuncular myiasis, painful lesions that resemble pyogenic granuloma or abscess. Female botfly captures mosquito and attaches its eggs to the mosquito body, and then releases the mosquito. Eggs hatch on mosquito becoming larvae and are deposited on human skin. Larvae use bite site as portal of entry into skin. A pruritic papule develops at the site, slowly enlarging over several weeks into a domed nodule (resembles a furuncle) with a central pore (Fig. 28-5). Larvae drop out after 8 weeks to pupate in soil.
House Flies. Larvae deposited into any exposed skin site (ear, nose, paranasal sinuses, mouth, eye, anus, and vagina) or at any wound site (leg ulcers, ulcerated squamous and basal cell carcinomas, hematomas, umbilical stump) and grow into maggots, which can be seen on surface of wound causing wound myiasis (Fig. 28-6). Maggot debridement therapy is used to selectively debride necrotic wound tissue.
Figure 28-6. Wound myiasis Multiple housefly larvae in a chronic stasis ulcer on the ankle after castellani paint and Unna boot treatment for 1 week. Upon removal, the maggots were visible; and base of the ulcer was red and clean, having been debrided by maggots.
Cimex lectularius or bedbugs bite exposed skin (face, neck, arms, hands) of sleeping humans. Feeding, which takes 5–10 minutes. Papular urticaria (Fig. 28-2) occur at bite sites. Bedbug hides in crevices of walls, mattresses, and furniture. Reddish brown streaks may be seen on mattress; bedbugs defecate old blood meal while ingesting a new meal.
Reduviid or kissing bugs bite usually present as papular urticaria; severe reactions can produce necrosis and ulceration. Subfamily of reduviid bugs transmits Trypanosoma cruzi, the agent of Chagas disease.
Fleas. Papular urticaria at bite site. Dog fleas often live in carpeting and bite exposed lower legs. Secondary changes of excoriation, prurigo nodularis, and S. aureus infection occur.
Tunga Penetrans or Chigoe Flea. Papule, nodule, or vesicle (6–8 mm in diameter) with central black dot (tungiasis) produced by posterior part of the flea’s abdominal segments. As eggs mature, papule becomes a white, pea-sized nodule (Fig. 28-7). With severe infestation, nodules and plaques with a honeycombed appearance. Ulceration, inflammation, and secondary infection can occur. Most common on feet, especially under toenails, webspaces, plantar aspect of the feet, sparing weight-bearing areas; in sunbathers, any area of exposed skin.
Figure 28-7. Tungiasis Periungual papule with surrounding erythema on the lateral margin of the fifth toe; the larva is visualized by removing the overlying crust.
Female bee, hornet, or wasp sting producing immediate burning/pain, followed by intense, local, erythematous reaction with swelling and urticaria. Severe systemic reactions occur in individuals who are sensitized, with angioedema/generalized urticaria and/or respiratory insufficiency from laryngeal edema or bronchospasm and/or shock.
Fire and harvester ants produce local skin necrosis and systemic reactions to sting; bite reaction begins as an intense local inflammatory reaction that evolves to a sterile pustule.
Caterpillar/moth contact can produce burning/itching sensation, papular urticaria, irritation due to histamine release, allergic contact dermatitis (Fig. 28-8), and/or systemic reactions. Windborne hairs can cause keratoconjunctivitis.

Figure 28-8. Immunologic IgE-mediated contact urticaria: pine processionary caterpillar Linear edematous papules and vesicles occurred on the exposed arm shortly after exposure to Thaumetopoea pityocampa in a pine forest.
Differential Diagnosis
Papular urticaria. Allergic contact dermatitis, especially to plants such as poison ivy or poison oak.
Diagnosis
Clinical diagnosis, at times, confirmed by lesional biopsy.
Treatment
Prevention. Apply insect repellent such as diethyltoluamide (DEET) to skin and permethrin spray to clothing. Use screens, nets, clothing. Treat flea-infested cats and dogs; spray household with insecticides (e.g., malathion, 1–4% dust).
Larvae in Skin. Tungiasis. remove flea with needle, scalpel, or curette; oral thiabendazole (25 mg/kg per day) or albendazole (400 mg/d for 3 days) for heavy infestations.
Furuncular myiasis: suffocate larvae by covering with petrolatum and removing the following day.
Glucocorticoids. Give potent topical glucocorticoids for a short duration for intense pruritis. Oral glucocorticoids can be given for persistent pruritus.
Antimicrobial Agents. Secondary Infection Antibiotic treatment with topical agents. Systemic Infection/Infestation Treat with appropriate antimicrobial agent.
Pediculosis Capitis ICD-9: 132.0  ICD-10: B85.0
ICD-10: B85.0 
 Infestation of the scalp by the head louse.
Infestation of the scalp by the head louse.
 Feeds on scalp and neck and deposits its eggs on hair.
Feeds on scalp and neck and deposits its eggs on hair.
 Presence of head lice is associated with few symptoms but much consternation.
Presence of head lice is associated with few symptoms but much consternation.
Etiology and Epidemiology
Subspecies. Pediculus Humanus Capitis. Sesame seed size, 1–2 mm. Feed every 4–6 h. Move by grasping hairs close to scalp; can crawl up to 23 cm/day. Lice lay nits within 1–2 mm of scalp. Nits are ova within chitinous case. Young lice hatch within 1 week, passing through nymphal stages, growing larger and maturing to adults over a period of 1 week. One female can lay 50–150 ova during a 16-day lifetime. Survive only for a few hours off scalp. Transmission: head-to-head contact; shared hats, caps, brushes, combs; theater seats; pillows. Head louse is not a vector of infectious disease.
Demography. In United States, more common in whites than blacks; claws have adapted to grip cylindrical hair; hair pomade may inhibit infestation. In Africa, pediculosis capitis is relatively uncommon; however, lice easily grip noncylindrical hair. Estimated that 6–12 million persons in the United States are infested annually.
Clinical Manifestation
Symptoms. Pruritus of the back and sides of scalp. Scratching and secondary infection associated with occipital and/or cervical lymphadenopathy. Some individuals exhibit obsessivecompulsive disorder or delusions of parasitosis after eradications of lice and nits.
Infestation. Head lice are identified by eye or by microscopy (hand lens or dermatoscope) but are difficult to find. Most patients have a population of <10 head lice. Nits are the oval grayish-white egg capsules (1 mm long) firmly cemented to the hairs (Fig. 28-9); vary in number from only a few to thousands. Nits are deposited by head lice on the hair shaft as it emerges from the follicle. With current infestation, nits are near the scalp; with infestation of long standing, nits may be 10–15 cm from the scalp. In that scalp hair grows 0.5 mm daily, the presence of nits 15 cm from the scalp indicates that the infestation is approximately 9 months old. New viable eggs have a creamy-yellow color; empty eggshells are white. Sites of predilection: Head lice nearly always confined to scalp, especially occipital and postauricular regions. Rarely, head lice infest beard or other hairy sites. Although more common with crab lice, head lice can also infest the eyelashes (pediculosis palpebrarum).
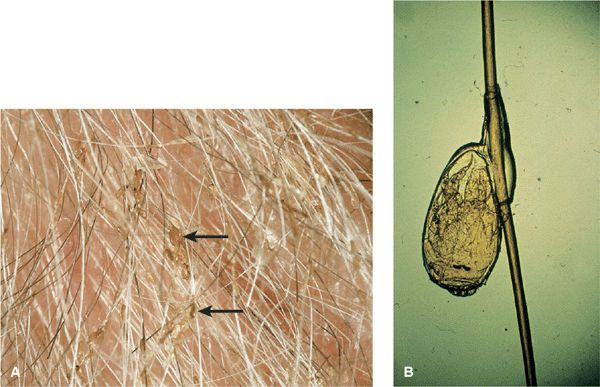
Figure 28-9. Pediculosis capitis: nits (A) Arrows: grayish-white egg capsules (nits) are firmly attached to the hair shafts, visualized with a lens. (B) Magnified, an egg with a developing head louse nymph attached to a hair shaft is seen.
Skin Lesions. Bite reactions: papular urticaria on the neck. Reactions related to immune sensitivity/tolerance. Secondary lesions: Eczema, excoriation, lichen simplex chronicus on occipital scalp and neck secondary to chronic scratching/rubbing. Secondary infection with S. aureus of eczema or excoriations; may extend onto neck, forehead, face, ears. Posterior occipital lymphadenopathy.
Differential Diagnosis
Small White Hair “Beads” Hair casts (inner root sheath remnants), hair lacquer, hair gels, dandruff (epidermal scales), piedra.
Scalp Pruritus. Atopic dermatitis, impetigo, lichen simplex chronicus.
No Infestation. Delusions of parasitosis.
Laboratory Examinations
Microscopy. Nits 0.5-mm oval, whitish eggs (Fig. 28-9B). Nonviable nits show an absence of an embryo or operculum. Louse. Insect with six legs, 1–2 mm in length, wingless, translucent grayish-white body that is red when engorged with blood.
Diagnosis
Clinical findings, confirmed by detection of lice. Louse comb increases chances of finding lice. Nits alone are not diagnostic of active infestation. Nits within 4 mm of scalp suggest active infestation.
Treatment
Topically Applied Insecticides. Permethrin, malathion, pyrethrin, piperonyl, butoxide.
Systemic. Oral ivermectin (200 mg/kg).









