div class=”ChapterContextInformation”>
8. A 25-Year Old Woman with Scaly Hypopigmented Lesions
Keywords
Pityriasis versicolorMalasseziaSpaghetti and meat ballsAzelaic acidAzoles
Multiple hypopigmented macules and patches with fine scales on upper back (Courtesy: Dr. Piyush Kumar)
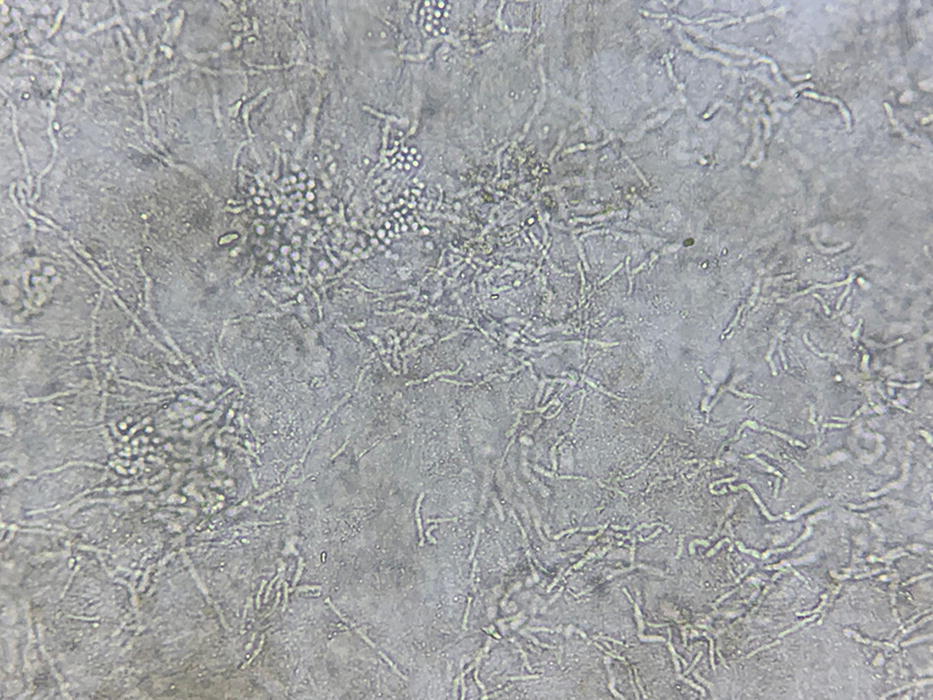
KOH mount showing thick-walled spherical yeast in clusters, with short fungal filaments (Courtesy: Dr. Piyush Kumar)
- 1.
Pityriasis rosea
- 2.
Pityriasis versicolor
- 3.
Pityriasis lichenoides chronica
- 4.
Seborrheic Dermatitis
Diagnosis
Pityriasis versicolor (Tinea versicolor)
Discussion
Pityriasis versicolor (PV), also known as tinea versicolor is a superficial, recurring fungal infection of the stratum corneum, characterized by scaly, dyspigmented irregular macules most often occurring on the trunk and extremities [1]. Malassezia yeast, a dimorphic fungus, is the causative organism whose mycelial form is mainly responsible for clinicopathologic changes [2]. Currently 12 species of this dimorphic fungus are known; commonly implicated ones are M. furfur, M. sympodialis, and M. globosa [3].
As mentioned earlier, PV may present with both hypopigmented and hyperpigmented macules and patches; sometimes, both types of lesions are noted in same patient. In general, dark-skinned population develops hypopigmented lesions, while hyperpigmented lesions are common in people with lighter skin color. The hypopigmentation in PV is caused by azelaic acid (a dicarboxylic acid produced by fungus) mediated inhibition of tyrosinase enzyme [4]. Malassezin, another metabolite from fungus, is implicated in causing apoptosis of melanocytes and may have a contributory role in causing hypopigmented lesions. On the other hand, hyperpigmentation is believed to be caused by abnormally large melanosomes [5], a thick stratum corneum [6], and a hyperemic inflammatory response [7, 8]. Malassezia spp. secrete other metabolites like pityriacitrin, pityrialactone, etc. which are responsible for fluorescence produced under wood’s lamp.
Malassezia spp. is a common commensal, present over seborrheic areas of the body (head, scalp and central trunk) and usually does not cause disease. Various predisposing factors which results in transition of normal commensal form of this dimorphic fungus into pathogenic mycelia form are hot and humid environment, hyperhidrosis, immunosuppressed state, use of medications like systemic corticosteroids, oral contraceptives, and malnourished state [9]. Other than PV, Malassezia sp. is implicated in Pityrosporum folliculitis and Seborrheic dermatitis.
Clinical appearance of PV is characteristic enough to clinch the diagnosis and is characterized by scaly oval to round macules coalescing to form patches of pigmentary alteration ranging from almost white to pink to reddish brown with dust like scales and wrinkled surface present over upper trunk and extremities, with macules starting in perifollicular location (vide Fig. 8.1) and then coalescing. On scratching the lesions, extensive scaling is produced (Scratch sign or coup d’ongle sign). Wood’s lamp examination helps in making the diagnosis and potassium hydroxide (KOH) examination is confirmatory. Biopsy is rarely required and periodic acid-Schiff (PAS) staining reveals oval budding yeast and branching hyphae which appears as ‘banana and grapes’ or ‘spaghetti and meat balls’.
The common differential diagnoses include pityriasis lichenoides chronica, pityriasis rosea and seborrheic dermatitis. Pityriasis lichenoides chronica starts with erythematous scaly papules which leave hypopigmented macules on healing, and runs a longer course. Pityriasis rosea has a history of herald patch, followed by development of secondary lesions along the lines of cleavage in a Christmas tree pattern. The individual lesion is annular with collarette of scales. Seborrheic dermatitis is characterized by greasy loose or adherent scales, involvement of scalp, glabella, ala nasi, retroauricualr area, sternal area, midscapular area, and flexures. This itchy condition runs a chronic relapsing course.
PV is treated by topical and oral antifungals with some life style modifications (avoiding prolonged exposure to hot, humid environment if possible, changing wet under garments frequently, frequent baths etc.). Topical treatment can be divided into specific ones having fungistatic activity and non-specific ones. Topical antifungals bifonazole, clotrimazole, oxiconazole, and miconazole have direct fungistatic activity. Most commonly prescribed topical antifungals are ketoconazole shampoo and 1% terbinafine cream. Selenium sulphide (lotion, cream, or shampoo), and zinc pyrithione are other helpful agents.
Non-specific topical measures act by physically or chemically removing the superficial dead infected skin layers. Non-specific treatments include propylene glycol, and Whitfield’s ointment [10, 11].
Fluconazole 400 mg single dose
Itraconazole 200 mg daily for 5 days
Pramiconazole 200 mg daily for 3 days
Related posts:
 Years Old Male with Multiple Hyperpigmented Macules on Trunk
Years Old Male with Multiple Hyperpigmented Macules on Trunk
 Gray Pigmented Macule on Right Cheek
Gray Pigmented Macule on Right Cheek
 6 Years Old Male with Multiple Black Spots on Face
6 Years Old Male with Multiple Black Spots on Face
 of Skin Pigmentation on Feet in a Female
of Skin Pigmentation on Feet in a Female
 Young Man with Hypopigmented Macules on Trunk and Multiple Shiny Nodules Over Face
Young Man with Hypopigmented Macules on Trunk and Multiple Shiny Nodules Over Face
 Young Boy with Generalized Hyperpigmentation
Young Boy with Generalized Hyperpigmentation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


