Abstract
Contouring procedures and treatments of the thighs that rely on invasive and noninvasive technologies, present a unique challenge to any level of surgeon. Technical competence notwithstanding, outcomes are often negatively influenced by the complex 3-dimensional anatomy of this region, the notable variance of patient clinical presentations and the inherent risk profile of the contouring technologies themselves. But mastery is not elusive. It is dependent on many pre-treatment and preoperative factors including the adequacy of the physical exam, the competent analysis of the patient’s imaging, the reasonable management of a patient’s expectations, and most importantly, the strength of the treatment plan that takes into account how well each technology works in the specific aesthetic subunits. Successful and reproducible outcomes should also be expected. Good results are largely dependent on the adequacy of the pretreatment and preoperative markings, the maintenance of patient comfort during the treatment or surgery, safe use of the contouring technology that systematizes patient positioning and a conservative approach to lipoplasty when included, especially when combined with technology based lipolysis. Lastly, post-treatment and postoperative care can be easily standardized and it should take into account the length of time for full results to be realized, up to 6+ months when laser-assisted lipolysis (LAL) or radiofrequency-assisted lipolysis (RFAL) is used.
24 Technology-Based Contouring of the Thighs
24.1 Introduction
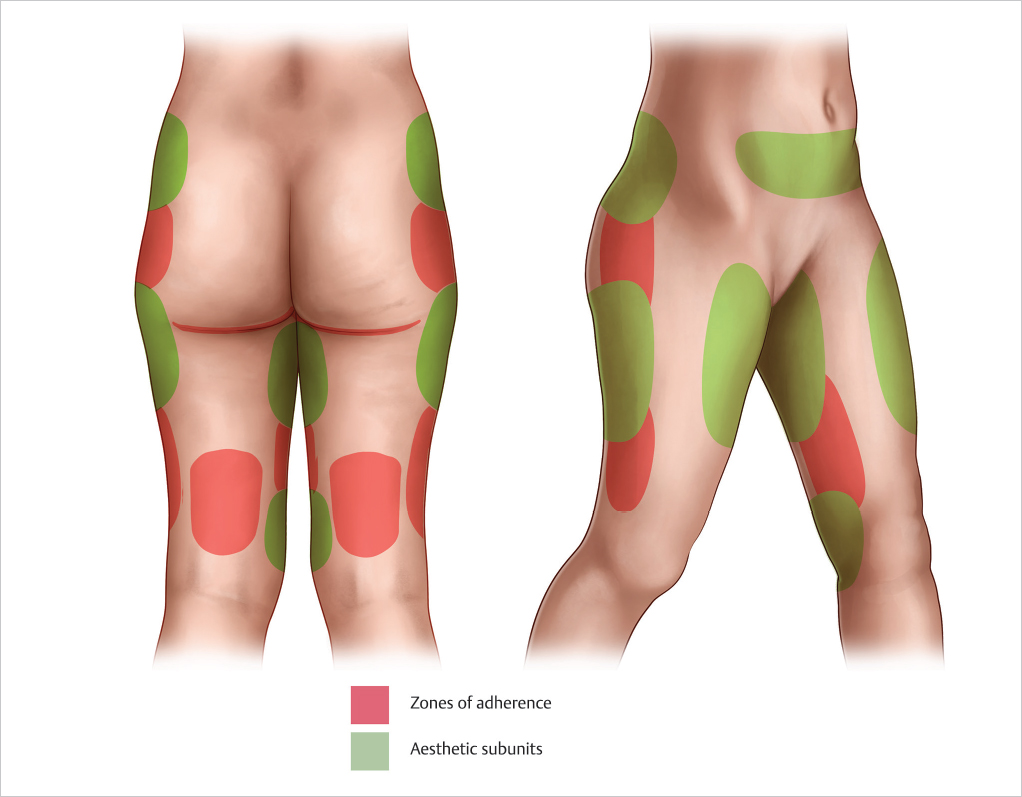
When considering the nascency of liposuction in the field of aesthetic surgery in the 1980s, Illouz’s understanding of the complexities of lower extremity contouring procedures was remarkable. His delineation of the zones of adherence of the lower extremity (▶Fig. 24.1) and his descriptions of the associated blunt liposuction related complications (e.g., edema, ulceration, and hyperpigmentation) in these areas created a road map that plastic surgeons use to this day. 1 However, from the time of Illouz to present day, lower extremity contouring treatments and procedures have presented a special challenge to surgeons with a disproportionate number of average to unsatisfactory outcomes. Invariably multifactorial, this inherent difficulty does not often correlate to the surgeon’s technical competency. Asymmetric localized adiposity, variable elasticity, contour deformities including cellulite, post-surgical deformities, skin abnormalities like striae and varicosities, heterogeneity of thigh fat and bilateral three-dimensional variances, are just a few of many factors that muddy the waters of a patient’s clinical presentation. Add in the exploding field of invasive and noninvasive energy-assisted body contouring devices and the approach to thigh contouring has become more elaborate and progressively more confusing. Therefore, to truly master technology-based contouring of the thighs, one must be as facile and competent with the creation of a treatment plan as they are with the contouring treatments and procedures themselves.
As all aesthetic subunits of the lower extremities should be addressed en bloc, limiting your focus to one area will diminish the power of any treatment or procedure outcome. In the interest of clarity, this chapter will focus solely on the thighs, or the area of the lower extremities superior to the patella and popliteal fossa and inferior to the inguinal and gluteal crease.
24.2 Patient Evaluation
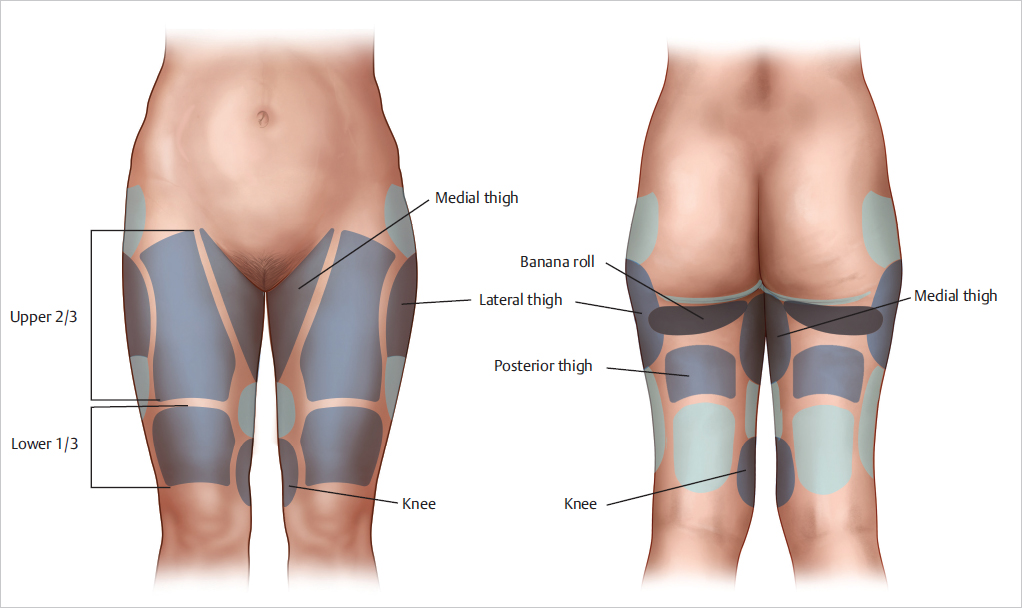
Evaluation of the thighs should always take into account the variable three-dimensional distribution of the superficial fat. As with the nose, assessing a complex three-dimensional anatomic location like the thigh for aesthetic purposes should incorporate aesthetic subunits. This author has found benefit in defining these subunits solely on the common areas of localized adiposity. This includes the medial thigh, lateral thigh, banana roll, upper 2/3rd of the anterior thigh, lower 1/3rd of the anterior thigh and the posterior thigh (▶Fig. 24.2). The lateral portion of each thigh, inferior to the saddlebags, rarely has issues related to localized adiposity in a normal weight patient. The fat in this area is often fibrous and diminished along tensor fascia lata. In a similar fashion, the medial portion of each thigh, inferior to the medial thigh fat pad, usually has a paucity of superficial fat and should be approached with care. It is important to note that the presentation of cellulite is often an outlier and is many times found in these medial and lateral zones. Therefore, when assessing cellulite alone, this author divides the thigh into four equal quadrants and then further divides each quadrant with a grid pattern.
The clinical exam should proceed as follows:
A thorough review of the patient’s pertinent past medical history including but not limited to surgical history, comorbid conditions, psychiatric history and current medications.
A discussion of expectations related to a patient’s thigh contour, both with and without clothes is essential to establishing realistic expectations. This should be completed before the exam so as to not to introduce bias.
The physical exam should be completed both in a standing and sitting position. Furthermore, tangential lighting should be incorporated into the exam to better elucidate superficial contour deformities like cellulite.
Photographic and/or three-dimensional imaging documentation during the initial clinical exam is highly recommended. Reviewing these images during the initial consult allows for a more constructive discussion with the patient regarding the treatment plan. In the author’s practice, the images are projected to 1/2 life size proportions on the wall of the consulting room with overlay of diagramming, so that the patient can clearly visualize the areas of concern.
24.3 Preoperative Planning and Preparation
The treatment options for technology-based contouring of the thighs are plentiful. At the time of this publication, there were at least 15 noninvasive body-contouring devices that have FDA clearance or off label application for thigh contouring and at least Level 4 evidence from clinical studies using the American Society of Plastic Surgeons Levels of Evidence Rating Scale. 2 This does not include the multitude of devices and treatments, like injection lipolysis, that are just making their way to market for thigh contouring. A thorough review of noninvasive body-contouring devices can be found in Section 2 of this book. As integrating all of the devices into a clinic setting would not be feasible for even the largest practice, it is important to focus your practice’s capital expenditure on diversity of treatment technology and the combination treatment potential. But make no mistake, the field of body contouring is heading in a less invasive direction and it is imperative to have at least one noninvasive device in your office. In the author’s experience, treatment of superficial thigh localized adiposity with noninvasive body-contouring devices offers, at best, a 30% reduction in the treated fat. This is far removed from the efficacy of lipoplasty and should therefore not be presented as an equal alternative. Consider these devices adjunctive and a formative tool to potentiate lipoplasty results. Furthermore, as standalone treatments, they offer a powerful option for patients who are not good candidates for lipoplasty or those who do not desire a more invasive option. These options will vary per physician depending on their device lineup and their practice focus. Treatment settings should be adjusted per the clinical judgment of the physician and the recommendations from the manufacturer.
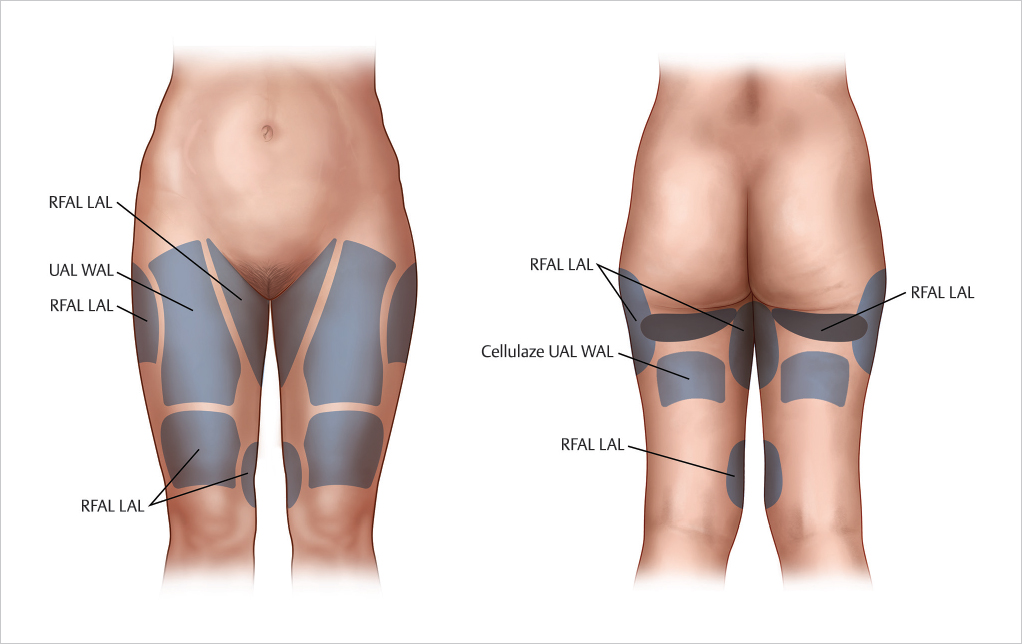
Technology based lipoplasty devices offer the most absolute treatment of localized adiposity of the thigh. A thorough description of these technologies can be found in this book. When developing a treatment plan for thigh contouring, it is useful to sort the application of these technologies by their usefulness in each aesthetic subunit and most importantly, by the skin quality in the treatment area. In general, ultrasound-assisted liposuction (UAL) and water-assisted liposuction (WAL) are more useful in large areas of debulking that have less skin elasticity concerns, like the upper 2/3rd of the anterior thigh and the majority of the posterior thigh. These technologies also have the added benefit of preserving the viability of adipocytes for autologous fat transfer, preserving the superficial lymphatic network thus decreasing postoperative edema and having the most desirable safety profile. 3 , 4 LAL and RFAL are more useful in areas of localized adiposity with variable levels of skin elasticity, like the medial thighs and lower 1/3rd of the anterior thigh. Although UAL technology like VASER does appear to have improved skin retraction in comparison to suction-assisted liposuction (SAL) (17% versus 10%), LAL devices like Smart Lipo and RFAL devices like Bodytite offer more potential for skin retraction (18 to 22% and up to 35% respectively). 3 , 5 , 6 Smart Lipo devices have the added bonus that Cellulaze can be added to the platform. Cellulaze is currently the most effective energy assisted invasive treatment option for cellulite. 7 Recommended application of each technology as it pertains to aesthetic subunits can be found in ▶Fig. 24.3. Lastly, as each of these devices allows for improved treatment and recovery when compared to SAL, the primary focus should be on inclusion in a liposuction case, not exclusion based on an aesthetic subunit.
As with any aesthetic procedure, there should be a binal approach to preoperative planning, balancing patient expectations with the clinical presentation. Al la carte approach is discouraged as residual localized adiposity in untreated aesthetic subunits will diminish results. For areas that need less than 30% improvement, the patient is given the option between invasive or noninvasive modalities. For more notable levels of localized adiposity, technology based lipoplasty is the treatment of choice. Progressive practices incorporate combination treatments of both invasive and noninvasive modalities. Furthermore, the noninvasive modalities are usually a patient’s first introduction to the practice allowing for more meaningful marketing of the invasive options.
Exclusion criteria for liposuction and the requirements for office-based surgery is reviewed in Section 1. Thigh lipoplasty cases can be completed in the office setting unless combined with other procedures that require a higher degree of anesthesia. Diagramming on the preoperative photos is an important tool to finalize the surgical plan and is additive to the medical records.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


