Abstract
Injection adipocytolysis is a relatively new concept for treating discernable pockets of fat. Though injecting medications in the hope of destroying adipocytes has been ongoing for years, there has never been a Food and Drug Administration (FDA) approved drug for this aesthetic indication until the introduction of deoxycholic acid (ATX-101) into our aesthetic armamentarium. This treatment requires no incision or scar creation and its slight discomfort is ameliorated with pretreatment of local anesthetic injection. The irreversible destruction of the adipocytes leads to significant, bespoke, nonsurgical contouring of the treated area.
15 Injection Lipolysis–Neck
Key Points
FDA approved first in class drug to permanently destroy adipocytes and treat submental fullness.
Non-selective cytolysis.
Addition to aesthetic physician armamentarium to treat patients with palpable preplatysmal fat for neck contouring.
15.1 Introduction
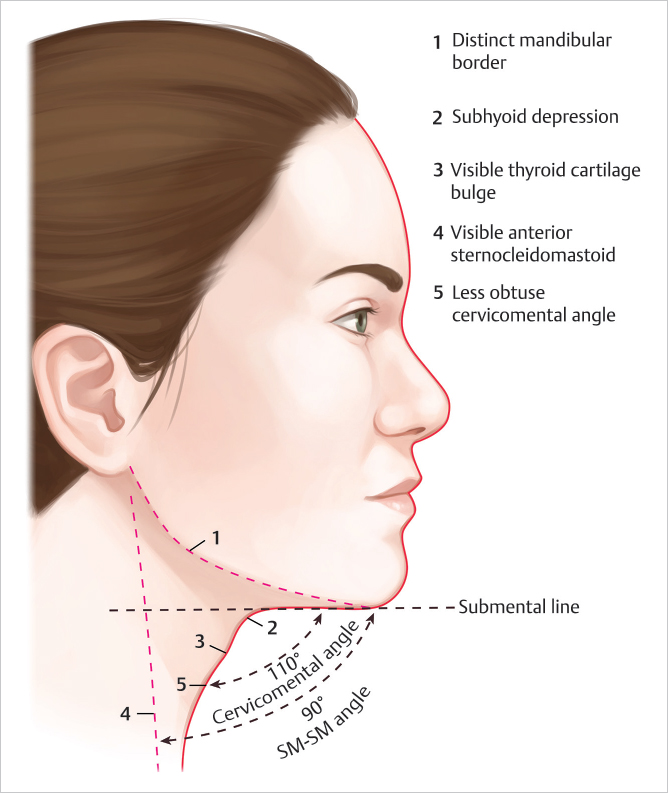
A youthful appearing neck remains essential to the aesthetically pleasing face. The submental region/neck falls into the “lower third” of a full-face assessment and has a strong impact on the overall aesthetics of a male or female. Hallmarks of the ideal aesthetic neck are: distinct mandibular border, cervicomental angle of 105 to 120 degrees, visible anterior border of the sternocleidomastoid m., subhyoid depression, and thyroid cartilage bulge (▶Fig. 15.1). 1 All characteristics of the aesthetically pleasing neck can be softened or obliterated by accumulation of submental fat also known as the preplatysmal fat, resulting in an undefined and unpleasing neck appearance. Submental fat accumulation can be attributed to aging, obesity, poor lifestyle and diet, or genetic predisposition. 2 , 3 As stigmata of aging and/or obesity, an excess accumulation of subcutaneous fat in the neck may have negative psychological impact.
Several multimodal approaches to neck rejuvenation have been employed to address unwanted submental fat. Invasive techniques, including platysmaplasty, liposuction, direct lipectomy, or any combination of these procedures can be effective in addressing submental fat. 1 , 4 These procedures may not be suitable or desired by all patients, however. Invasive procedures, while generally well-tolerated, have: increased recovery times, higher risk profile, need for additional staff expertise, need for anesthesia, and need for additional office infrastructure—operating room or similar suite. Several of the technical considerations resultantly lead to increased procedural costs. Non-surgical energy devices have been developed to address excess submental fat are limited by insufficient evidence supporting their efficacy.
The need for an effective, noninvasive alternative to surgical management of excess submental fat was the impetus to the development of the injectable form of the lipolytic agent deoxycholic acid (DCA). The drug was studied under the name: ATX-101. To date the only FDA approved agent of the market is Kybella (Allergan Pharmaceuticals, Irvine, California) (▶Fig. 15.1).
15.2 Deoxycholic Acid (DCA)
Over the last several decades, chemical techniques for fat reduction have been developed as nonsurgical alternatives. The first agent utilized was phosphatidylcholine (PC), introduced in 1985 for the treatment of xanthelasmas. Later, PC was used for correction of lower eyelid bulging due to prominent fat pads 5 , 6 and for localized subcutaneous fat deposits. 7 , 8 With further experience, it was observed that DCA, the solvent for PC, was responsible for the lytic action of PC/DCA combination formulations on cells in cell culture and fresh porcine skin, leading to the hypothesis that detergents play a role in the elimination of undesired adipose tissue. Studies demonstrated that DCA-alone induced adipose cell lysis just as effectively as DCA with PC. 9
Deoxycholic acid is a naturally occurring, bile-derived compound found in most animals 10 and functions as a nonselective detergent-like lipolytic agent. 11 Detergents have both hydrophobic and hydrophilic regions and are classified as ionic, nonionic, or zwitterionic. 12 Sodium deoxycholate belongs to the ionic group of detergents, containing polar and nonpolar chemical properties that function to emulsify insoluble substances by reducing surface tension of cell membranes. 12 , 13 In doing so, DCA causes adipocyte rupture by disrupting the integrity of adipocyte cell membranes, which results in smaller micelles of fat that ultimately undergo phagocytosis. The DCA is in turn metabolized through the liver while the remaining adipocyte remnants are excreted through the gastrointestinal tract.
When injected into the subcutaneous layer, DCA causes adipocyte lysis ultimately resulting in decreased adipocyte density with fibrotic tissue replacing the adipose tissue. 12 The resulting physical and histological changes do not lead to atrophy or hardening of the surface layer of the skin, but rather has been hypothesized to instigate a moderate skin tightening/retracting effect. These combined effects have led to increasing public interest in DCA as an ideal substance for minimally invasive treatment of unwanted fat.
15.3 Patient Evaluation
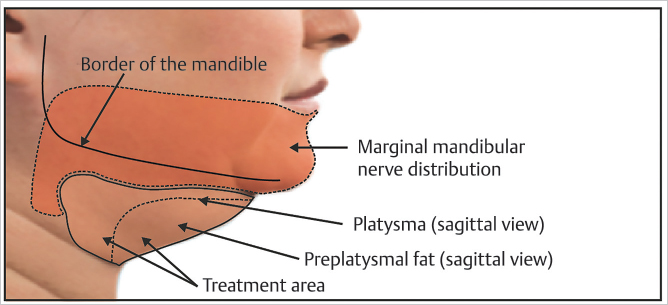
Assessment of the neck for lipolytic injectable treatment requires a thorough understanding of preplatysmal fat and its compartmentalization. As in other fat compartments of the face, the submental fat pad is located in a distinct compartment. Housed within the preplatysmal fat, the submental fat pad is consolidated to the submental crease, caudal continuation of labiomandibular fold, and palpable hyoid bone. The fullness can contribute to an obtuse cervicomental angle (▶Fig. 15.2). 14 There exists a continuation of submental fat pad outside the anatomic landmarks, however, the fat is less full (generally) but is uniformly distributed in the subcutaneous space. In cadaveric studies, the dispersion of injections of dyed gelatin was used to elucidate the boundaries of submental fat compartments. 15 Injection of lipolytics can be expected to disperse similarly and understanding this compartmental anatomy is essential in procedural planning to address specific patient needs. On initial patient evaluation, the submental landmarks should be identified and the contained soft tissue evaluated with special attention toward volume, contour, skin quality and thickness, and any preexisting asymmetries (▶Fig. 15.2).
Patient evaluation and physical exam are quite straightforward and mirror evaluation of patients who are requesting liposuction in this anatomic area. The physical exam maneuvers require the physician to pinch, palpate, pull, and have patient grimace. Pinching and palpating allows one to assess the amount of palpable subcutaneous fat in this region. An obtuse cervicomental angle could also be secondary to platysma laxity and aging skin with minimal submental fullness (SMF). Care should be taken to rule out thyroid goiter, neck masses, adenopathy, and prominent submandibular glands. Once the practitioner establishes that there is presence of subcutaneous fat amenable to treatment, pulling on the skin and looking for laxity and dermal recoil helps the physician establish whether or not the patient is a good candidate. Ideally, the patient has appropriate skin recoil, which establishes that he/she will benefit from the treatment and see significant improvement from the subsequent fibrosis, which results after the liquefactive necrosis is cleared during the inflammatory reaction. Finally, asking the patient to grimace effectively is asking the patient to fire his/her platysma muscle which forces the post-platysma fat deep allowing the practitioner to assess the subcutaneous fat of the neck. One can liken this maneuver to asking patients to fire his/her rectus abdominis muscles, which pushes intra-abdominal fat deep and allows one to only pinch and palpate the subcutaneous fat of the abdomen.
15.4 Preoperative Planning and Preparation
Patients should undergo physical and local examination (assessment for edema, bruising, numbness, paresis, and tenderness), assessment of vital signs, and evaluation for bleeding disorders before and after initiation of each treatment session. The only absolute contraindication to the procedure is active infection at the treatment site. The patient should be counseled that he/she will experience a period of edema secondary to the inflammatory response. The swelling can be pronounced, but generally fully resolves by day 5–10 depending on age, skin laxity, amount of subcutaneous fat, and aggressive nature of treatment (amount of medication used).
Pre-procedure photography should be undertaken to document response. Respecting the Frankfort horizontal plane is critical to standardize angles of the photos. The patient should be counseled that he or she should anticipate the need for 2–4 treatments at 6 weeks intervals to see full effect. Furthermore, there is continued improvement without treatment at weeks 6–12 during wound healing.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


