Abstract
This chapter discusses the use of solid silicone implants in buttock augmentation including patient evaluation, preoperative planning, surgical technique, management of common complications and revisional buttock implant surgery. Intramuscular and subfascial implant placement along with the advantages and disadvantages of both techniques are discussed. Recommendations for achieving successful outcomes are presented along with relevant citations from the scientific literature. Case examples with photographs are included illustrating the results of gluteal augmentation with implants.
23 Gluteal Augmentation with Implants
Key Points
Biodimensional planning is essential to obtaining good results.
Select an implant that will produce the maximum point of projection at the correct level.
Avoid implants greater than 350 cc in primary implant surgery.
Choose the insertion plane best suited for the patient.
Ensure that the wound closure is tension-free.
Recognize and act on complications as soon as possible.
Be prepared to remove implants early in case of infection.
Patient compliance with limited activity in the postoperative period is essential.
Implant replacement after infection can be performed after 6 months.
23.1 Patient Evaluation
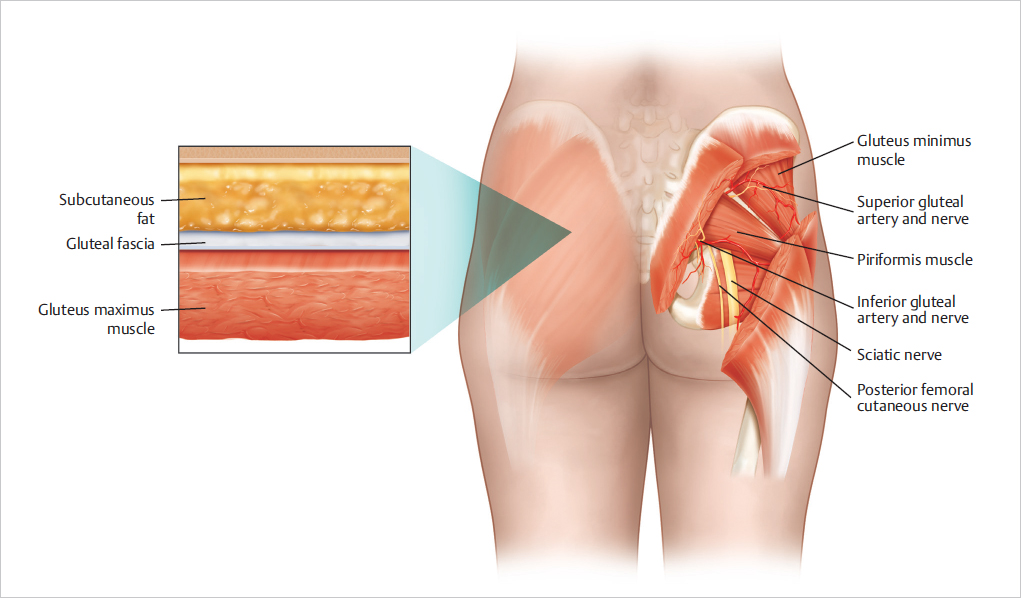
The evaluation of a potential candidate for gluteal augmentation begins with an assessment of several anatomic variables which determine the suitability for surgery and affect the potential results. The underlying shape of the pelvis and spine although not part of the augmentation procedure should be considered. The pelvis may present limitations on the size of the implant as a narrow pelvis will require an implant of less base diameter than would fit in a wide pelvis. The spine should be examined to look for preexisting asymmetries that may affect the results. The shape and volume of the buttocks are mostly determined by the gluteal musculature along with the amount and distribution of subcutaneous fat. Understanding the contribution of the muscle and fat specific to each patient is an important part of evaluating potential candidates for gluteal augmentation. 1 The skin of the buttock region should be evaluated in terms of thickness, elasticity, and position relative to the infragluteal fold. Patients with skin laxity and infragluteal fold ptosis may require a buttock lift or direct fold excision in order to obtain an acceptable result. An understanding of the anatomy of the gluteal region is essential in the evaluation and planning of surgery (▶Fig. 23.1). 2 , 3 , 4
The practical approach to evaluating a patient presenting for buttock augmentation using an implant involves choosing the type of implant and the plane of insertion. The choice of implant between round and oval and the plane of insertion of either subfascial or intramuscular depends on three anatomic variables. The first anatomic variable requiring attention is the length of the buttock. A patient with a long buttock would be more suitable with an oval anatomic implant. A round implant placed in a long buttock would likely leave the bottom third of the buttock empty. A short buttock would be more suited towards a round implant since an implant with an appropriately sized base diameter would fill all areas of the buttock. Implant position can be determined through evaluation of the second anatomic variable which is the amount and quality of subcutaneous fat. A patient with thick subcutaneous fat would likely have enough soft tissue to conceal a subfascial buttock implant. Patients with minimal buttock subcutaneous fat would benefit from intramuscular implant placement to avoid complications such as palpability and visibility. In patients with inadequate soft tissue of the buttock gluteal implant placement is not advisable. The third anatomic variable of skin laxity should be evaluated to determine the need for skin excision. Moderate buttock skin laxity is likely to require infragluteal fold excision after buttock implant surgery while severe buttock skin laxity should be managed with a buttock lift prior to implant placement.
It is important for surgeons who perform buttock augmentation to be familiar with both techniques of intramuscular and subfascial implant placement. 5 , 6 The history of buttock augmentation with implants dates back to 1969 with the insertion of a round breast implant through an infragluteal fold incision to correct left gluteal muscle atrophy. 7 Cosmetic gluteoplasty was first described in 1973 by placing implants in the subcutaneous plane. 8 The choice of incision including bilateral supragluteal, infragluteal fold, and the intergluteal crease was described in 1977. 9 , 10 The intramuscular implant is more difficult to insert as the dissection plane is indistinct and often bloody. In addition, intramuscular placement can result in lack of inferior fullness if the inferior pole is not dissected enough. Intramuscular implant placement has been shown to result in as much as a 6.4% atrophy of the gluteus maximus muscle with a subsequent return of strength. 11 The advantage of intramuscular placement is less palpability, less visibility, and less infragluteal fold stretching. The complication rates after intramuscular placement were found to be lower than other pocket locations. 12 The subfascial technique is based on the ability of the gluteal aponeurosis to hold the implants in position. 13 The subfascial technique has the advantage of an easier and distinct dissection plane with less blood loss along with a more global buttock enhancement with greater projection. 14 The disadvantage of subfascial placement in thin patients is implant palpability and visibility of the edges and possible infragluteal fold displacement.
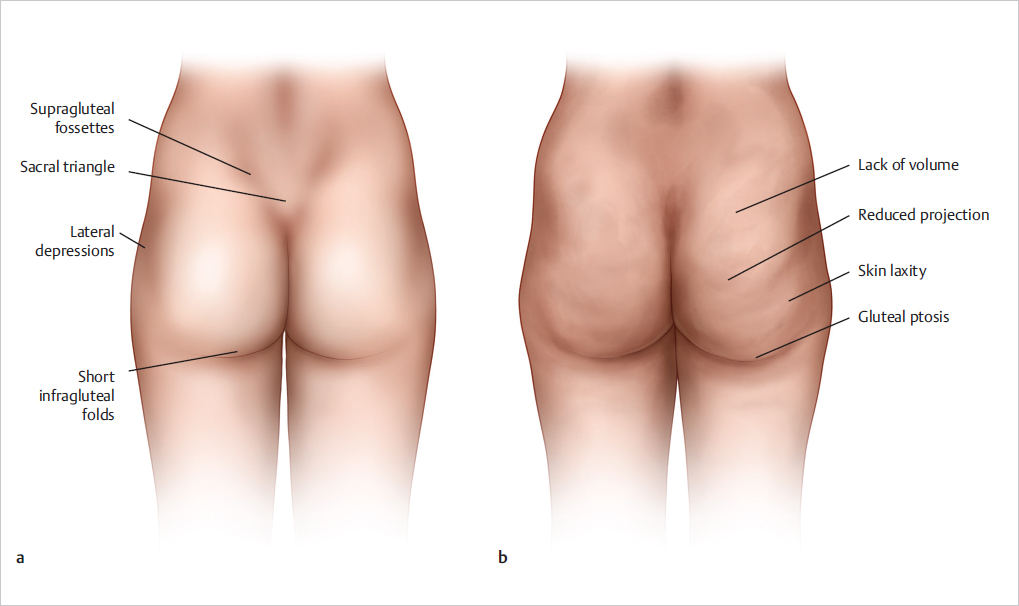
After examining a patient presenting for consultation for gluteal implants the surgeon must decide whether the patient is a good candidate for surgery. The ideal candidate for gluteal implants is a normoweight patient in good health with sufficient buttock soft tissue to support and conceal an implant. Indications for buttock augmentation with an implant include: lack of volume, poor projection, asymmetry, contour deformity, and limited availability of fat for transfer (▶Fig. 23.2). Contraindications to buttock implant surgery include: inadequate soft tissue, general or local infection, unrealistic expectations, psychological instability, and diabetics on insulin. Precautions to buttock implant surgery include: autoimmune disease, poor wound healing, BMI greater than 30, prior buttock injections, and a history of radiation to the buttocks. 15
23.2 Preoperative Planning and Preparation
When planning buttock implant surgery it is important to first define patient expectations in order to determine whether these expectations can be met. After an evaluation of the anatomic variables of the buttock and determining implant shape and placement and potential need for skin lift the potential choice of implants can be presented to the patient. Having sample implants of varying shapes and sizes is essential to precise preoperative planning. Biodimensional analysis with consideration of the buttock base diameter and length and capacity for volume expansion should be exercised when choosing the appropriate buttock implant. The limitations of implant size should be communicated to the patient during the planning stage of surgery. It is important to only use an implant that is appropriately sized to the dimensions of the patient. Attempting to insert an implant that is overly large in order to satisfy patient desires is counterproductive and can result in complications. Implants over 350 cc should not be inserted by the inexperienced buttock implant surgeon. During the preoperative examination, the implant sizer is placed over the buttock at the desired point of maximal projection to determine suitability. By placing the sizer on the patient, a determination can be made whether to use an oval or round implant by the amount of lower buttock that is covered by the implant sizer. If the lower pole is not adequately addressed with a round implant an oval anatomic implant should be considered. For patients who desire large volume augmentations the risk of wound healing complications should be emphasized. These patients would benefit from insertion of an appropriately sized implant and offered an implant exchange to a larger size after a minimum of 6 months when the capsule is formed and stable.
The patient can prepare for surgery by cleansing the surgical site with Chlorhexidine the night before and the morning of surgery. A light low residue diet is recommended prior to surgery. A bowel prep is not necessary. Preoperative labs and medical clearance are obtained for those patients with medical concerns.
23.3 Surgical Technique
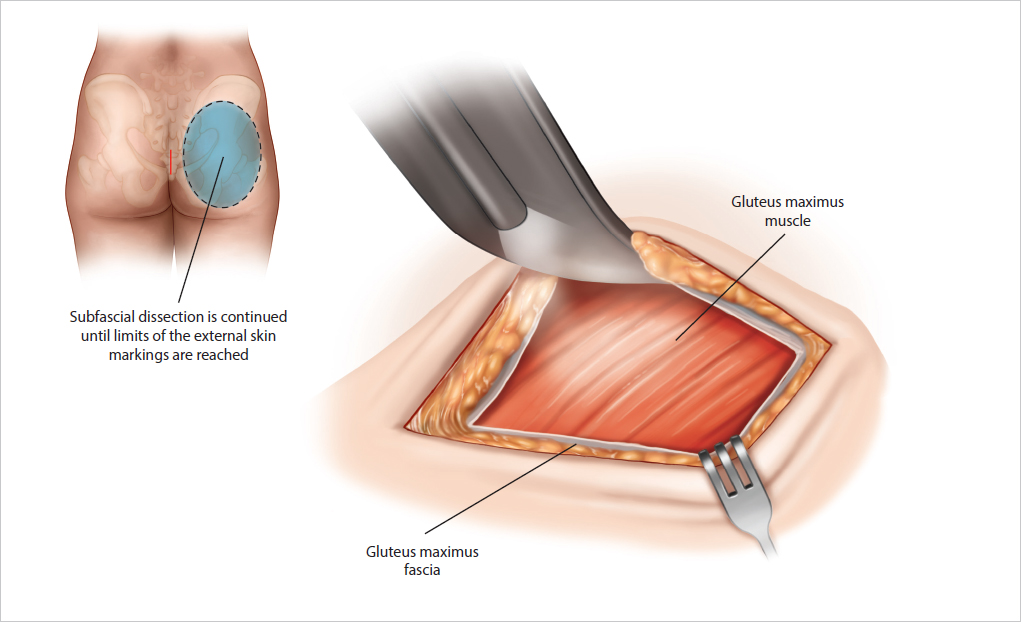
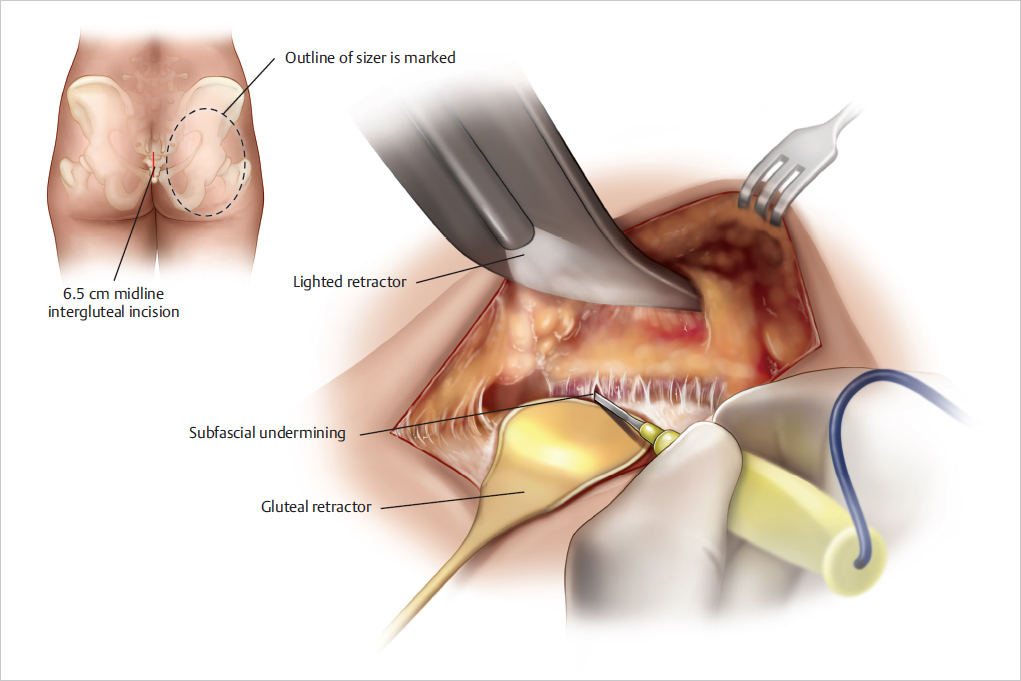
The patient is marked in the upright position by placing the appropriate implant sizer over the desired maximum point of projection of the buttock which usually corresponds to the level of the pubis. The sizer is then outlined with a surgical marker. Areas of liposuction or fat grafting are marked if necessary. The patient is placed on a stretcher and undergoes either general endotracheal, epidural, or spinal anesthesia. Bolsters and placed under the hips and chest and the patient is positioned prone on the operating table. A urinary catheter is inserted if the expected length of surgery is over 3 hours. Sequential compression devices are placed on the lower extremities. A surgical scrub of the buttocks is done followed by a surgical prep with either povidone iodine or chlorhexidine and alcohol. A rolled-up laparotomy sponge is placed over the anus followed by draping. The use of a barrier drape such as Ioban (3M, St. Paul, MN) is recommended to reduce potential intraoperative wound contamination. A dose of Cefazolin is administered intravenously prior to skin incision. The markings are infiltrated with 1% lidocaine with epinephrine. A single 6.5 cm midline intergluteal incision is made down to the sacral fascia ending inferiorly at the level of the coccyx. Surveys of American and international surgeons revealed a preference for the single midline incision. 16 , 17 Another acceptable incision is the bilateral parasacral incision which leaves an intact area of midline intergluteal skin for closure. After making the intergluteal incision dissection is performed laterally exposing the gluteus maximus fascia. The fascia is then incised parallel to the intergluteal skin incision exposing the gluteus maximus (▶Fig. 23.3). Subfascial undermining is then performed with the aid of a lighted fiberoptic retractor and long tip electrocautery. The use of a specially designed gluteal retractor can aid in the dissection by placing downward pressure on the gluteal musculature thereby creating a better optical cavity (▶Fig. 23.4). The dissection is continued until the limits of the external skin markings are reached. Perforating blood vessels can be coagulated with the use of an insulated forceps. The subfascial dissection should be precise and mostly bloodless. It is important to not over dissect laterally or inferiorly to avoid potential migration and malposition of the implant. After dissection is complete the wound is rinsed with an antimicrobial solution of either povidone iodine and saline or antibiotics. Hemostasis is obtained and the wound is re-prepped. The implant is rinsed in antibiotic solution and then placed into the subfascial space through the intergluteal wound. It is important to position the implants far enough away from the midline so that a tension-free closure can be performed. Closed suction drains are not usually necessary. Wound closure is then begun by tacking each side of the incision to the midline sacral fascia and periosteum. Layered wound closure is then continued with absorbable sutures and a running intracuticular suture.
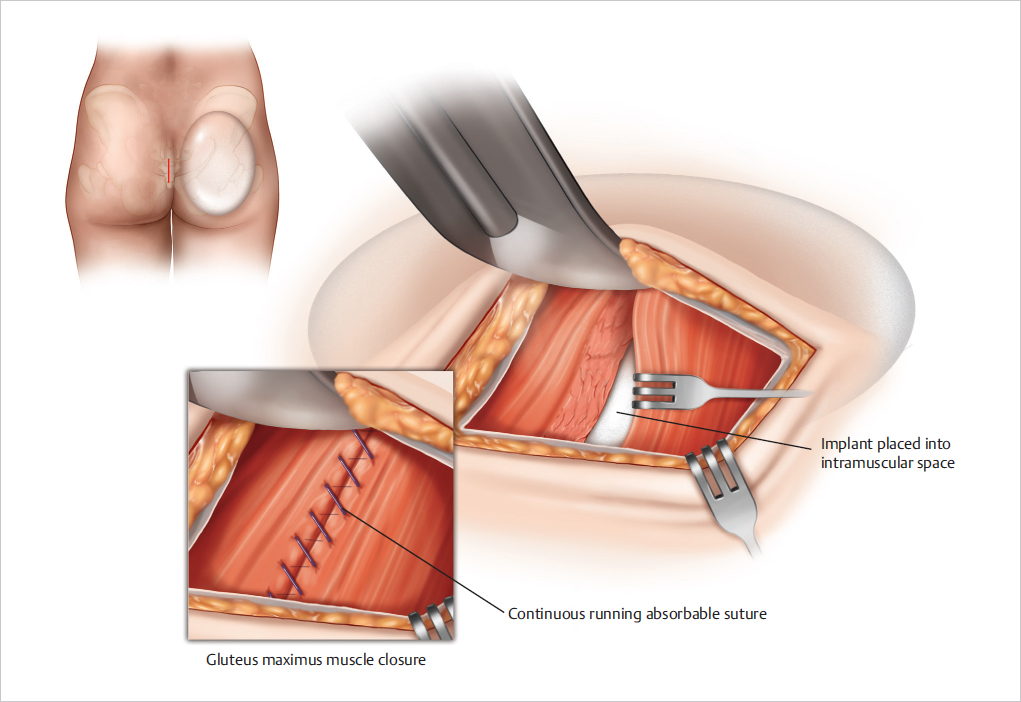
The intramuscular technique begins with subfascial dissection exposing the gluteus maximus for 7 cm on both sides of the midline incision. The gluteus maximus is then divided parallel to the direction of its muscle fibers to a depth of 2–3 cm. A mostly blunt dissection plane is then established using a blunt dissector and a fiberoptic retractor. A long smooth tip insulated forceps is used to coagulate perforating intramuscular blood vessels. The inferior portion and the superior portion of the intramuscular pocket should be at the same depth and result in the creation of one continuous intramuscular space 2–3 cm thick of sufficient size to accommodate the desired implant. 18 , 19 It is important not to over dissect laterally to avoid implant displacement. Care must be taken to avoid perforating the gluteus maximus muscle when dissecting laterally as the muscle curves downward toward the hip. 20 After completion of the dissection laparotomy pads are placed into the newly created intramuscular space to check the adequacy of dissection and to check hemostasis. Laparotomy pads are then removed and adjustments to the dissection can be made. The wound is then rinsed with antibiotic solution. The wound is re-prepped and the implants are placed into the intramuscular space and positioned appropriately. Drains are often used as the blunt muscle dissection results in bleeding. The gluteus maximus is closed securely over the implant with either a continuous running absorbable or permanent suture. The midline incision is then closed in layers as described earlier (▶Fig. 23.5).
After the completion of surgery the patient is placed on a stretcher and awakened from anesthesia. Compression shorts are applied. The patient is then brought to the recovery area and placed in the prone position until discharge.
Patients are advised to recover at home in the prone position as much as possible for the first week. Sitting should be avoided for 2–3 weeks if possible. Compression shorts are recommended for 3 weeks. Early ambulation is recommended to avoid deep vein thrombosis but strenuous activity is discouraged. Exercise can be resumed in 6–8 weeks. Muscle relaxants may prove beneficial in patients undergoing intramuscular implant placement. Oral antibiotics are used according to surgeon preference. Drains are removed when less than 25 mL of fluid is obtained in a 24-hour period. If the drainage does not subside or fluid accumulates after drain removal a sample of periprosthetic fluid should be sent for culture. If infection is suspected antibiotic therapy can be initiated and then adjusted after the results of the culture are obtained.
Ancillary surgical procedures that can enhance the results of buttock augmentation include liposuction, fat grafting, buttock lift, and excision of the infragluteal fold. Liposuction of the lower back can improve the waist to hip (WHR) ratio to produce a more desirable proportion. 21 , 22 , 23 A WHR quotient of 0.7 in women is widely accepted as a standard of beauty. 24 In men, liposuction of the lower back and flanks can create a more attractive result. Fat grafting can add additional volume to the buttocks and create a smooth transition between the buttock implant and the lateral thighs and hips. Liposuction with fat grafting can be safely performed at the time of buttock implantation or later on to add volume or correct contour irregularities. 25 In patients with severe laxity of the buttocks infragluteal fold excision or buttock lift may be performed prior to implantation. In patients with mild buttock skin laxity a reassessment of the buttock skin 3 months after implantation is advisable. At this time, precise correction of the infragluteal fold may be safely performed. Markings for infragluteal fold excision are performed in the upright position taking care to place the scar in the new infragluteal fold. After full-thickness skin excision the wound is closed in multiple layers without wide undermining of the wound edges. It is important to tack the wound margins to the fascia to secure the position of the new infragluteal crease. The goal of the skin excision is to create a buttock that is rounder, tighter, and more youthful appearing. Drains are not required. Compression shorts are applied and patients are instructed to recover in the prone position. Sitting is to be avoided for 2–3 weeks.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


