24 Back Contouring

Abstract
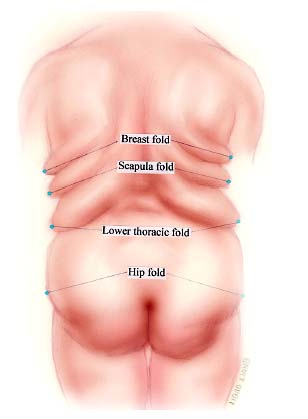
Surgical management of morbid obesity offers sustained massive weight loss (MWL). Acceptance of bariatric surgery as an effective method of weight loss has led to increases in the number of these procedures and, subsequently, an increase in bariatric plastic surgery. According to the American Society of Plastic Surgeons’ statistics, almost 60,000 body-contouring procedures after massive weight loss were performed in 2008. Body contouring in the MWL patient involves treatment of multiple areas of redundant skin and subcutaneous tissue, usually in a staged manner. Although much has been written about the surgical management of the abdomen, chest and breasts, arms, buttocks, and thighs in these patients, the back has received relatively less attention. Excess back tissue causes difficulty fitting into clothes and brassieres. It can also contribute to back pain. This chapter reviews the anatomy of the back folds and details our approach to back contouring in postbariatric weight-loss patients. In general, up to four individual back rolls are observed in weight-loss patients, each requiring surgical correction: breast fold, scapula fold, lower thoracic fold, and hip fold.
Introduction
Anatomy of the Back Folds
Patients typically develop back folds of excess skin, subcutaneous fat, and fibrous tissue after massive weight loss (MWL). These folds develop around “zones of adherence,” as the redundant tissue drapes over these attachments. The back rolls generally number from one to four on either side of the mid-line, depending on the patient’s pre–weight-loss anatomy, amount of weight loss achieved, and degree of tissue adherence. The number of back folds can also differ on each side.
Based on examination of multiple postbariatric plastic surgery patients, we have developed nomenclature for the various back folds to clarify the surgical management of each fold. The superiormost fold is a posterolateral extension of the breast fold related to the inframammary fold and is thus referred to as a breast fold or roll. The next highest fold is the scapula fold. The lower truncal back folds are the lower thoracic fold and hip fold ( Fig. 24.1 ). A fifth roll is infrequently identified near the axilla.
Indications
Patients usually develop problems related to redundant skin and subcutaneous tissue after bariatric surgery, although some patients are able to achieve MWL through nonsurgical means. In either case, body-contouring procedures are deferred until the patient’s weight is stable for several months, generally no earlier than 1 year after bariatric surgery. The procedures are staged, usually addressing circumferential truncal excess as the first stage. Breast surgery and brachioplasties are then performed together. Back contouring occurs over several operations, depending on the individual patient requirements. Medial thigh lifts are performed as the last stage. The patients understand that they are accepting multiple long scars for better body contour.
The lower thoracic and hip rolls are addressed during a circumferential abdominoplasty.1 All the tissue from the middle of each roll is excised. When the balance of the rolls is flattened, closure is obtained without tension or undermining. The lateral breast roll is removed as part of the Wise-pattern breast procedure extending to the posterior axillary line. An elliptical excision is used to contour the remaining breast fold and scapular fold. The entire breast fold is excised, but only the superior half of the scapula fold is removed. The lower half of the scapula fold advances superiorly, allowing for a tensionless closure.
Technique
The majority of MWL patients who undergo mid-body contouring have circumferential abdominoplasties. The decision to perform a circumferential excision is based on the presence of the lower thoracic and hip folds, as well as buttock ptosis. The removal of the lower two back folds as part of a circumferential abdominoplasty has been previously described.2 The midpoints of these rolls mark the upper and lower limits of the lines of resection in the circumferential abdominoplasty, with incisions planned through the apex of the two rolls. Placing the incisions through the apex of the rolls allows for adequate tissue resection without undue tension ( Figs. 24.2 and 24.3 ). No undermining is performed, and the residual elements of the lower back rolls are flattened as the back excision is closed. Avoiding unnecessary undermining reduces dead space and decreases the risk of seroma formation.
Patients who have significant lateral breast fold excess undergo removal of this excess tissue as part of the breast procedure. The Wise pattern is extended laterally to the mid-axillary line to incorporate the lateral breast fold into the excision.
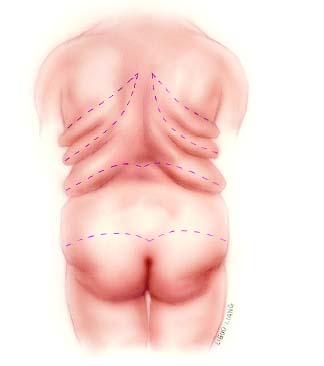
In a separate procedure, the remaining upper breast roll and scapular roll are excised in an elliptical fashion ( Fig. 24.3 ). Preoperatively, the patient is marked in a standing position with arms at the sides. An oblique ellipse is drawn along the axis of the back rolls on each side, avoiding crossing the mid-line. The upper line includes the entire breast fold, whereas the lower line follows the apex of the scapular fold. In the operating room, tumescent fluid (1 ampule of 1:1,000 epinephrine and 50 cc of 1% lidocaine in 1 L of lactated Ringer’s solution) is injected into the back rolls. The tissue within the markings is removed using sharp dissection in a suprafascial plane. Similar to the lower back, no undermining is necessary after the excision of the excess tissue. The wound is then closed as a straight line using 2–0 chromic sutures for the deep layer and 4–0 Monocryl or absorbable dermal staples for the deep dermis and superficial dermis. Tissue glue and Steri-Strips complete the closure. A Penrose drain is placed in the wound before final closure ( Figs. 24.4, 24.5, 24.6, 24.7,, and 24.8 ).

Related posts:
 26 Upper Body Lift for the Correction of Back Rolls
26 Upper Body Lift for the Correction of Back Rolls
 27 Bra-Line Back Lift
27 Bra-Line Back Lift
 25 Approach to Excess Trunk Rolls with a Vertical Excision
25 Approach to Excess Trunk Rolls with a Vertical Excision
 4 Anesthesia and Safety Considerations in the Perioperative Period
4 Anesthesia and Safety Considerations in the Perioperative Period
 17 Brachioplasty with Interdigitation of the Posteromedial Scar
17 Brachioplasty with Interdigitation of the Posteromedial Scar
 36 Facial Rejuvenation: Open Technique
36 Facial Rejuvenation: Open Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


