25 Approach to Excess Trunk Rolls with a Vertical Excision
Abstract
Traditional methods of abdominoplasty and mastopexy do not address the skin excess and laxity seen in post–massive weight loss patients. Redundant tissue of the lateral chest wall and residual laxity of the abdominal wall are bothersome to these patients and may not be addressed even with a midline abdominal incision or by extension of the inframammary scar. An approach that includes a vertical lateral excision, either just of the thorax or extending down the length of the body, can be used to remove this excess. The scar is well tolerated and hidden down the length of the body.
Introduction
As the population of patients who have undergone bariatric surgery continues to increase, more patients are being seen with areas of excess skin and fat that are not addressed by traditional body-contouring procedures. New approaches and techniques are being developed to address these areas. Traditional approaches to the upper body have dealt primarily with the arms and breasts. Brachioplasty techniques have not addressed areas proximal to the axilla. Breast procedures have been limited to the breast itself. Post–massive weight loss (MWL) patients, however, have themselves brought the area of the lateral chest as well as the back rolls to the attention of plastic surgeons.
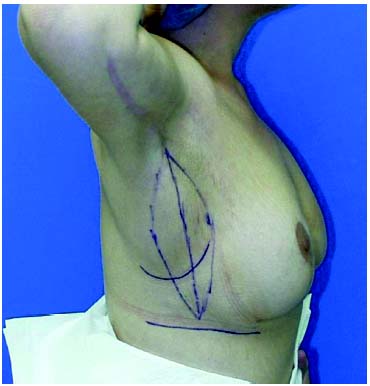
Excess skin and fat of the upper body has been a concern of women as they age and their weight changes. Arm reduction surgery was described as early as 1930 by Torek.1 Despite early descriptions of aesthetic brachioplasty in the South American literature2 and later by Pitanguy,3 Baroudi,4 and Lockwood,5 brachioplasty was still an uncommon procedure. When the first wave of MWL patients first appeared in plastic surgeons’ offices in the early 1990s, most plastic surgeons had never done a brachioplasty, let alone addressed excesses of the upper trunk. When applied to MWL patients, traditional techniques of brachioplasty, with the scar ending in the axilla, as well as the traditional techniques of mastopexy, with the inframammary scar ending no farther than the lateral aspect of the breast, left the excess of the chest wall untouched ( Fig. 25.1 ).
Similar to the traditional methods of brachioplasty and mastopexy not addressing areas of concern to the MWL patient, traditional abdominoplasty techniques do not adequately address the problems of laxity of the abdominal area or the back. Many of the first patients who had undergone bariatric surgery had done so through an open incision. This made it easy to approach the excess of the abdominal wall by adding a vertical incision. However, as more patients underwent laparoscopic procedures, there has been reluctance to add a midline scar due to the risk of dehiscence at the T-juncture. In addition, the addition of a T-incision has often been inadequate to address the upper abdominal laxity ( Fig. 25.2 ). Attempts to remove the excess of the upper abdomen by reexcision at a later time were often unsuccessful or inadequate even with the cosmetically undesirable extension of the scar superiorly over the sternum. The technique of lateral chest excision therefore has evolved from the natural extension of the brachioplasty onto the chest wall and then the natural extension of this incision along the length of the torso. This technique, when extended down the length of the torso, has been called the lateral thoracoabdominoplasty.6
Indications
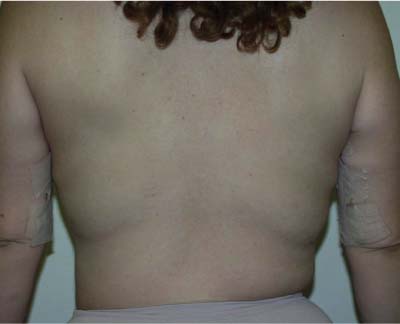
Patients requesting a brachioplasty should be evaluated for upper lateral chest wall excision. Very few MWL patients with redundant skin and fat of their arms will not also have redundant skin and fat of their torso. During the initial evaluation for a brachioplasty, it is important to examine the entire chest area and to consider the lateral excision at least as far as the inframammary fold as part of every brachioplasty. Some weight loss patients opt for a brachioplasty as their first procedure. Extending the excision to the inframam-mary fold does not interfere with any other surgical procedure, such as breast surgery, abdominal surgery, or even the full lateral excision. This procedure can also be performed in patients who have previously undergone a brachioplasty or breast surgery. Patients are very grateful for this suggestion, as they often find that, despite the brachioplasty and breast surgery, they are still limiting their wardrobe choices to camouflage the “bra roll” ( Figs. 25.3, 25.4, and 25.5 ). In addition, MWL patients requesting an abdominoplasty should be counseled if their anatomy predisposes them to residual laxity of the upper abdominal area. When patients have carried most of their excess weight in the abdominal area, they have residual laxity of the abdominal wall in both the vertical and horizontal dimension. A traditional abdominoplasty removes excess in one dimension only. Patients who present with several rolls of abdominal skin, especially rolls above the umbilicus, also most likely have residual upper abdominal laxity despite the tightest abdominoplasty ( Fig. 25.6 ). In the initial evaluation, this laxity and the two-dimensional component of it should be pointed out, and the possibility of further excision down the lateral thorax should be discussed. Fewer patients are candidates for the full lateral torso excision than for the upper lateral chest excision, but a patient who complains of residual fullness in the upper abdomen after a traditional abdominoplasty should be considered for this procedure.



The advantage to the lateral excision is that it not only removes the excess fat and skin of the upper lateral chest area, but also can improve the appearance of the breasts by correcting the downward slope of the inframammary fold. Aly7 describes the changes that occur in the chest as MWL occurs. The normal or “ideal normal” inframammary crease has a semicircular shape, with its lateral aspect rising superiorly as it progresses laterally.

After weight loss, the lateral aspect of the inframammary crease descends as it traverses from medial to lateral because the lateral thoracic tissues are located at the greatest distance from the medial fascial attachments. The medial attachments are fixed and do not change with weight gain or loss. The fascial attachments are located over the sternum and over the spine. As the weight loss occurs, the stretched skin is suspended from these fascial attachments, causing a lateral descent of the inframammary fold. Excision of the excess thoracic tissue can help correct this lateral descent of the inframammary fold. The excision of this excess tissue also immediately improves the appearance of the breast by defining the lateral extent of the breast ( Fig. 25.7 ).
This technique can be used in stages. If a patient is to undergo a brachioplasty, then the lateral chest wall should be evaluated. Patients can be classified as requiring an extended brachioplasty, which includes the lateral chest wall excision, or a brachioplasty ending in the axilla. If the patient has undergone an extended brachioplasty and an abdominoplasty and still has residual laxity of the abdominal wall, then the upper lateral thoracic excision can be extended to make continuous the extension of the brachioplasty down to the lower abdominal incision. This procedure should not be done at the same time as the abdominoplasty, as the blood supply would be interrupted to the anterior abdominal wall. A lateral excision at a later time is safe, however, as no undermining is done.

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


