21. Upper Eyelid Blepharoplasty
21.1 Introduction
The goal of this chapter is to show surgeons, practitioners, and perhaps the occasionally interested layperson how to transform bothersome and unattractive eyelids and orbital regions into lovely, handsome, well-functioning eyes. Although we limit our discussion primarily to the upper orbital region, truly successful “upper eyelid” rejuvenation demands consideration of much more than just the upper lid and orbital area. We therefore must briefly deal with these additional areas, as required, in the appropriate places.
Unfortunately, the vast majority of practitioners approach the eye region by focusing on what seems to be excessive eyelid skin, especially on the upper lids, and then promptly schedule a date for its simple removal. Yet such “simple” operations typically have such predictable, and ultimately undesirable, outcomes, such as plummeting eyebrows assuming a much lower resting position, exaggerated frown lines dispensing dissatisfaction and an appearance of anger, and the return of “extra” upper lid skin that seems just as prominent as it was before the initial eyelid surgery (Fig. 21.1).
The resulting patient dissatisfaction typically leads to one or more reoperations, each of which further deforms the eye region. The result is profoundly low brows, vision-threatening excessive skin excision of the upper lids, and an overall saddened and angry appearance—all from surgery designed to enhance one’s appearance (Fig. 21.2).

It is hoped that most of us who understand this message will vow to “reverse the process” before the surgeon’s second or third misinformed attempt to correct. Often the first and main element missing is a thorough preoperative eyelid and surrounding facial area examination, which we will describe and reinforce shortly.
21.2 Photographic Deception and Photo-Flattery
Photography itself is a common source of deception. Photographers (and some surgeons) are masters at manipulating photographs to create the desired result—as well as to hide deformity. Deception is also immensely widespread among the lay population, especially women. They are constantly altering their appearance, both to others and to themselves in mirrors. We have labeled this concept photo face and photo flattery.
Also, know that many of the photos of “nice-looking” results from presumed independent upper lid blepharoplasty, as published in textbooks and journals and shown at medical meetings, are of patients who have also undergone frontal lifts of one sort or another, counteracting those negative effects commonly seen after isolated upper eyelid blepharoplasties. Other “undisclosed improvements” can be administered by other maneuvers, like botulinum toxin injections or corrugator muscle excisions. Rarely are such details mentioned in the lecturer’s text or in published essays where “incomplete” operative descriptions find their way beneath the “before” and “after” patient photographs.
There are clues to deceptive photography, however, and every surgeon should look for the telltale signs commonly used by patients and photographers, especially head tilting, brow contracting, and forcing a smile.
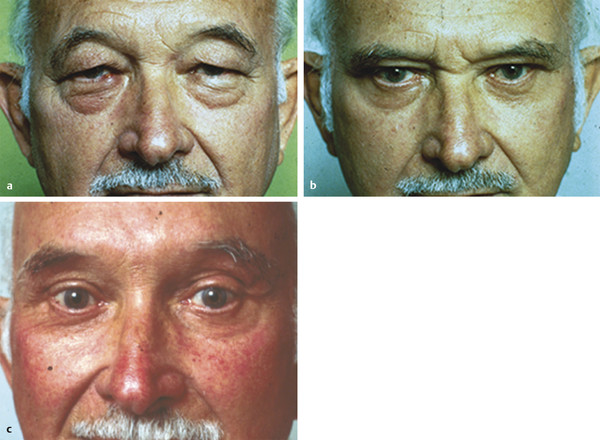
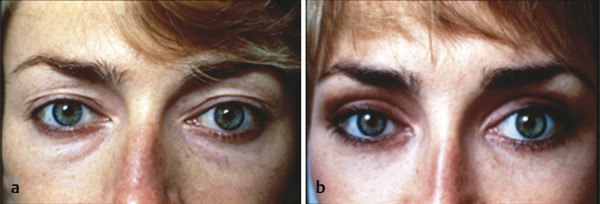
Because both age and an isolated skin excision blepharoplasty often result in a brow drop, two of the ways to disguise the lowered brow are to have the patient tilt the head slightly backward and to have him or her arch the brows. The arching can be easily detected by a furrowed forehead—if the patient’s skin is thin enough and the forehead is not cropped out of the picture or covered with bangs (Fig. 21.3).

An unmonitored patient “on his or her own” can unknowingly hide deforming or unnatural surgical outcomes by maximally raising his or her own eyebrows, tilting the head backward before mirrors or photographers’ cameras, and smiling to create the best possible look. This occurs before cameras and photographers, when women especially know they are being looked at, and also when they are in the process of looking into a mirror. This unconscious reaction is so consistent; we have labeled it the photo-face reflex, which we discuss more fully later in this chapter.
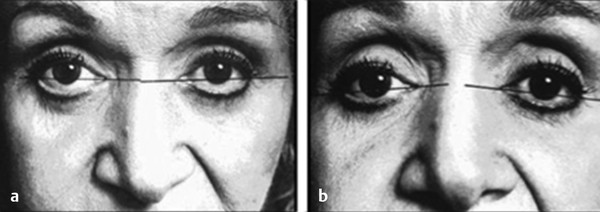
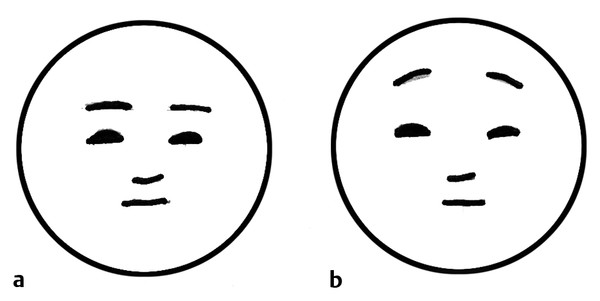
One way to discern head tilting influencing that is photography is to observe the intercanthal angle (Fig. 21.4). Draw a line precisely between the medial and lateral canthi in both eyes in the preoperative and postoperative photos. If they do not match, then the angle at which the photos were taken is different for the preoperative and post-op pictures. If the medial line tilts higher than the lateral half, then the head is likely tilted backward, which is ideal for disguising brow ptosis (from a skin excision blepharoplasty) and lower lid scleral show (from an isolated skin excision lower lid blepharoplasty) (Fig. 21.5). Each degree of alteration of the intercanthal line will represent approximately 1 mm of covered scleral show if the line is laterally tilted downward or 1 mm of uncovered scleral show for each millimeter tilted upward (that tilt is rarely seen medically but is often encountered in “ladies’ magazines”).
21.3 Do People (and Patients) Really Know What They Look Like?
20.3.1 The Photo Face
Over our years of practice, patients asking for some cosmetic surgical correction often bring a casual photograph . It is always an unexpected snapshot that some family member, acquaintance, or other person took without the patient’s knowledge.
The patient was amazed that the “unposed” picture of their face showed a feature (or features) that appeared to them as surprising and disgustingly unpleasant. By far, the two most common views brought were slightly off-center anterior photographs of the face and eye region (and of course, side views of prominent noses, which we will not be discussing). These “snapshot” experiences have increased profoundly since the advent of iPhone cameras, Facebook, and other “high-tech” developments.
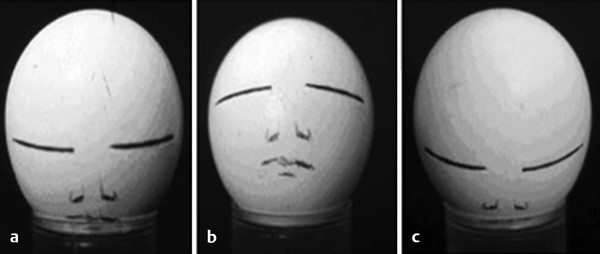
Most women have an altered idea of what their true at-rest face looks like. The same is true of men, but to a lesser degree, because they typically pay less attention to their appearance. When a woman becomes even “semiconsciously” aware that someone is looking at her, or going to look at her, she immediately and unconsciously does three things to improve her appearance and make it more youthful: (1) raises her eyebrows, (2) tilts her head slightly backward, and (3) generates at least a slight smile. 1
As mentioned, this reflex is so consistent that we have labeled it the photo face reflex (Fig. 21.6). It occurs not only when a camera approaches her face (or she perceives she might be looked at or photographed) but unconsciously every time she looks at herself in a mirror. The effect of this triple bit of transformational mischief is to dramatically alter her perception of her own appearance without being aware of what she is doing—until an unposed photo is presented.

Not only does the brow drop after an isolated skin excision blepharoplasty, but the relaxing frontalis muscle allows the (frown creating) corrugator muscles to contract unopposed, resulting in more prominent frown lines. The key factor here is that the vast majority of adults are constantly (but subconsciously) elevating their eyebrows to some degree (by activating the frontalis muscles) to maintain unobstructed vision.
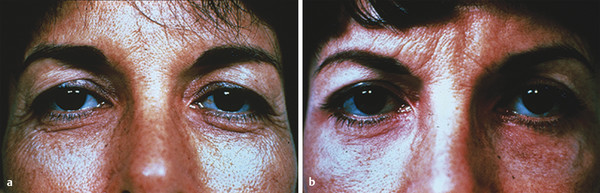
In most of the world’s adult population, removal of any upper eyelid tissue (without maximal forehead or frontal elevation) results in some frontalis muscle relaxation. That relaxation means the eyebrows both descend to a lower position, generally more medially than laterally. It was this epiphany that led the senior author on a lifelong quest to improve eyelid and periocular surgery (Fig. 21.7).
Frontalis muscle relaxation from upper eyelid surgery (or surgeries) will continue to drop the brows until they reach “rock bottom” or cannot stretch anymore. Each time they drop, it seems to add more “excess skin” to the patient’s upper lids, obliterating the positive results of the previous skin excision. This typically embarrasses the blepharoplasty doctor into reoperating and removing more of the visible upper eyelid skin “accidentally” left behind. 2
This repeatable process becomes more problematic with the passing years, even among those fortunate patients in whom frontalis contraction and brow elevation were not essential anatomical events in their youth and young adult years (see group 1 description to follow).
It is interesting that skin excision upper eyelid surgery is so commonly deforming to the appearance when it is performed independently, and yet it is tagged by the media as an “eye lift.” That seems hardly appropriate for an operation that lifts nothing and actually drops and deforms the brows (Fig. 21.8). The senior author best described it decades ago as an “eye-aging operation” that makes people look older, more tired, and angrier to boot!

21.4 Exceptions
21.4.1 Good Candidates for an Isolated Upper Lid Blepharoplasty
In some situations, however, the age-old skin excision blepharoplasty is indicated. There are three indications where an isolated upper eyelid blepharoplasty can be extremely beneficial and nondeforming. In addition to these, we discuss a special, fourth group of patients who already underwent isolated upper eyelid blepharoplasty and were in profound need of an “early after” bailout operation to restore their appearance to normalcy, near normalcy, or even attractiveness.
Group 1: Nicely Positioned Natural Eyebrows with No Frontalis Muscle Activity
A small percentage of people have eyebrows resting at a comfortable, nearly symmetrical position, attractively separating the thick forehead skin and the thinner cephalic upper-eyelid skin. These patients, like everyone contemplating eyelid surgery, must first be tested with the brow position carefully controlled: eyes closed, with forehead, frontalis muscles, and eyelid muscles in a total resting state. If the brows still have a nice brow position and posture even when relaxed, this patient is a good candidate for an isolated blepharoplasty and requires no eyebrow elevation.
In the true group 1 patient, an isolated upper eyelid blepharoplasty does not result in the eyebrows descending with eye closure (Fig. 21.9); however, this patient is far rarer than the vast majority, who, after the eyelid skin is excised or invaginated, have eyebrows that will drop significantly, but only when the eyes are closed and the forehead is relaxed.
Group 2: East Asian and Similar Eyelid Surgery
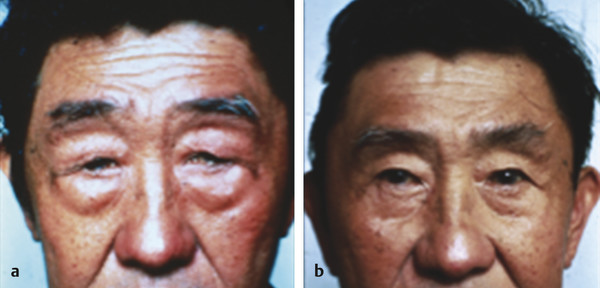
Group 2 comprises a large group, predominantly East Asians, who are born with and retain marked eyebrow elevation, which perhaps may be effected by shorter bony foreheads and shallower orbits with less protruding orbital rims and ridges (Fig. 21.10). These group 2 people, with their highly elevated eyebrows and long upper eyelids, can often benefit immensely from a well-done isolated upper blepharoplasty, preferably with combined upper lid fold creation, often referred to as “double eyelid surgery” by East Asians and as “anchor” or “invagination” blepharoplasty by non–East Asians (Fig. 21.11). With the lid surgery comes the simplified and comfortable ability to open the eyes widely and to enjoy comfortable forward vision. Fig. 21.11 shows the essence of these types of Asian blepharoplasties.

Even though this extreme brow elevation is common in East Asians, many others of similar ethnicity have eyebrows that are much lower, with less powerful frontalis muscles. These eyebrows are destined to drop profoundly after simple or classic East Asian lid surgery, destroying the presurgery teenager’s, young adult’s, or elderly person’s appearance. Blepharoplasty in these people demands contemporary browlifts with resection of the corrugator frown muscles to avoid the profound eyebrow and lid drop with immense frown exaggeration that makes these teenagers—and all others, including seniors—look vastly older and far less attractive.
Group 3: Elderly Patients
Middle-aged and elderly persons traditionally have a generous excess of stretched-out upper eyelid and forehead skin hanging over the eyes, often blocking vision, even with maximal brow elevation through frontalis muscle contraction. Their visual obstruction is generally improved by inconveniently tilting the head backward (if the aging cervical spine permits it); but in this “aging” group, even all the preceding steps are often insufficient to clear their vision because there is too much excess skin and overhang, especially laterally, making driving safely more difficult because the frontalis muscle, which characteristically inserts more securely into the medial brow, raises that area far more effectively, which clears medial eye vision a bit better than laterally.
Whether in East Asian or elderly white patients, the relatively long forehead skin and muscle with its caudad-positioned (when resting) eyebrows will require an exceptionally robust forehead muscle elevation, even in childhood, just to have unblocked vision. The raised-brow position is achieved by the fiercely hardworking and contracting frontalis muscle, which remains active throughout all waking hours. This condition does disfigure facial features that would otherwise appear more attractive, but the elevated eyebrows are absolutely necessary to lift the eyelids high enough to allow forward vision. In this population, however, proper frontal-lift surgery might not be desirable or possible for many reasons, including poor health, financial constraints, lack of insurance coverage, or simply aesthetics not being a high priority.
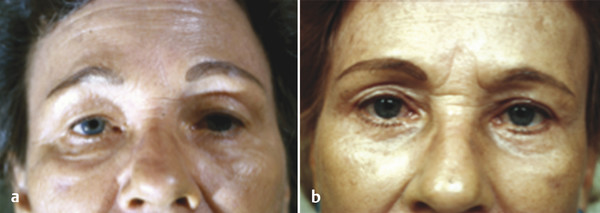
In these elderly patients, significant visual improvement still occurs with removal of a considerable amount of old, stretched upper eyelid skin, which commonly results in removal of the patient’s eyelid “creases” or “lid folds.” Re-creating the creases by invagination or anchor surgery offers slightly improved vision, and the invaginated lid crease usually makes the eyes more attractive while conserving a significant amount of skin to help protect the globe from exposure (Fig. 21.12). The eyebrows in these situations remain in the maximal elevation possible but seldom drop further because it obstructs vision. The corrugator frown muscle rarely activates sufficiently against the fiercely working and powerful frontalis muscle to thrust the corrugator frown into problematic presence.
Simple resection of considerable eyelid skin in these elderly people generally enhances the efficiency of the brow elevation task in clearing lid overhang, leaving far too little frontalis relaxation to cause significant frown exaggeration. Be sure you understand that the more skin removed from upper eyelids, the more the brow is inclined to drop, which generally makes both elderly women and men look older and less attractive. In people whose eyebrows are sufficiently elevated, and they are uncomfortable keeping them so positioned, the isolated upper lid excision can be quite beneficial (Fig. 21.13). This fact also applies to certain relatively young people who are able to keep their brows elevated. Understand, of course, that almost all the individuals referred to in group 3 can also benefit considerably more by combining their eyelid surgery with brow elevation procedures.
Related posts:
 6. Facial Sculpting and Facial Slimming with Neurotoxins
6. Facial Sculpting and Facial Slimming with Neurotoxins
 20. Comparison of Midface Rejuvenation Techniques
20. Comparison of Midface Rejuvenation Techniques
 22. Lower Eyelid Blepharoplasty
22. Lower Eyelid Blepharoplasty
 23. Lateral Canthal Complications in Aesthetic Eyelid Surgery: Prevention and Reconstruction
23. Lateral Canthal Complications in Aesthetic Eyelid Surgery: Prevention and Reconstruction
 5. Energy-Based Treatments for Facial Aging
5. Energy-Based Treatments for Facial Aging
 12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


