2 Techniques
2.1 Fundamentals
The choice of technique for covering a genital defect essentially depends on the location and size of the defect. The range of plastic and reconstructive techniques, in increasing order of surgical complexity, includes:
Primary closure.
Skin grafting (mesh graft, split-thickness graft, full-thickness graft).
Local flaps (random pattern flaps).
Pedicle flaps (axial pattern flaps).
Free flaps with microvascular anastomosis.
2.1.1 Skin Grafting
Skin grafts are indicated for defects which, by their nature, are either no longer conducive to closure with a primary suture or which do not require a flap.
Skin grafts are cut off from their original blood supply when harvested. From the time they are placed until sufficient revascularization has occurred 3 to 5 days later, they are supplied by diffusion from the wound bed. A graft that heals in place undergoes constant changes in appearance over the next few weeks, yet it will never look identical to the surrounding healthy skin.
Note
Generally favorable conditions for skin grafting include extensive even wounds with a well-vascularized wound bed or granulation tissue with little secretion.
Appropriate wounds should be debrided prior to grafting and should be free of infection. Exposed fatty tissue, bone without periosteum, or tendons without peritendineum will pose a risk to the graft’s vascular supply and integration. In these cases, other options for closing the defect should be considered.
Split-thickness skin grafts, usually in the form of mesh grafts measuring 4 cm2 or larger, are used to close wounds in the genital region. They are used where approximating the edges of the wound for a primary suture would not be feasible or where secondary healing would produce extensive, debilitating scarring and infection. Suitable donor sites for split-thickness skin grafts include the lateral or anterior thigh, or other regions of the body as required, depending on the location of the defect. After harvesting the split-thickness graft with a dermatome (e.g., 0.2 mm), the tissue is fed into a machine that processes it into a mesh graft that can be used to cover one and one-half to three times the original size of the defect. This makes it possible to satisfactorily cover even large and secreting wounds with a limited supply of skin. The graft is fixed with a suture or tissue adhesives, in applicable cases used in combination with a vacuum-assisted closure device to prevent shear forces for occurring on the graft. Because of the location in the genital region, some surgeons recommend their patients additional oral or intravenous antibiotic prophylaxis with a cephalosporin. After the first bandage has been changed (usually after 5–7 days), the patient can be switched to daily ointment gauze treatment or local antibiotic therapy where the progress of healing and the local situation permit it.
Full-thickness skin grafts are autologous skin grafts that include the dermis and epidermis. The range of applications for full-thickness skin grafts in the external genital region may be regarded as rather limited. They are more often used for the reconstruction of defects in the vaginal wall or in cases of vaginal aplasia. Donor sites include the lower abdominal and inguinal region, both medial thighs, and the scrotum. Whenever possible, the dimensions of the full-thickness skin graft should be such that they allow primary closure of the donor site. When the graft is harvested, all subcutaneous fatty tissue must be carefully removed. Hemostasis must be obtained in the wound prior to placing the graft to ensure that it will be properly integrated. Once the graft has been fixed, it is recommended to apply an elastic compression bandage for 3 to 5 days.
2.1.2 Flaps: Fundamentals
Flaps are differentiated according to their vascular supply as either local flaps, meaning flaps with a random dermal and subdermal vascular network (random pattern flaps), or pedicled flaps, meaning flaps with a defined vascular axis (axial pattern flaps). In random pattern flaps, this supply pattern greatly influences the design options of the respective flap. A ratio of length to width that does not significantly exceed 2:1 will ensure that the flap is sufficiently perfused. In contrast, the length-to-width ratio need not be restrictively maintained in axial pattern flaps; here the length depends on the area supplied by a defined vascular axis. Axial flaps, in which a cutaneous island is created by dividing the bridge of connecting skin, de-epithelializing the flap close to the base, or mobilizing the vascular pedicle to allow subcutaneous tunneling, are referred to as island flaps.
Vascular branches that ascend from the deep layer and supply the subcutis and cutis via an epifascial vascular plexus ensure the perfusion of what are known as fasciocutaneous flaps. Such a flap is supplied according to the classification of Mathes and Nahai 3 either by a single cutaneous perforating artery (type A), a septocutaneous perforating artery (type B), or one or more musculocutaneous perforating arteries (type C).
Perforator flaps consist of skin and subcutaneous fatty tissue supplied by isolated perforating arteries which pass through deeper layers after arising from their parent vessel. When such a perforator courses through a muscle before penetrating the fascia, it is known as a musculocutaneous perforator and when it courses through a septum, it is referred to as a septocutaneous perforator.
Muscular flaps are classified according to Mathes and Nahai 3 (▶Table 2.1) and are based on their respective vascular anatomy.
Type | Designation | Example |
I | Dominant vascular pedicle | Tensor fascia latae |
II | Dominant pedicle with nondominant vessels | Gracilis |
III | Two dominant vascular pedicles | Rectus abdominis |
IV | Segmental arteries | Sartorius |
V | Dominant pedicle with segmental arteries | Latissimus dorsi |
Local Flaps
If the surgeon decides to use a local flap to cover a defect, then careful preoperative planning is essential. To avoid creating a too large flap, the section to be debrided or excised is outlined first, then the appropriate flap. Everything else is done only after this.
Z-Plasty
The basic principle of the Z-plasty is a gain in length at the expense of width by shifting and transposing two pedicled triangles of skin. For this reason, it is commonly used in lengthening for prevention and treatment of scar contractures and strictures. Careful geometric planning must precede defect coverage; the respective limbs should always be equal. Although any angle between 30 and 90 degrees is possible, the triangular dissection of two or more flaps with an angle of 60 degrees each is regarded as optimal for transposition of the flaps at the expense of the transverse axis. In the presence of extensive findings, multiple Z-plasties are preferable to a single long-limb Z-plasty; the gain in length remains the same, yet multiple Z-plasties reduce the tension.
Pedicled Cutaneous Flaps
Simple skin grafts usually do not suffice in cases where not only skin but deeper lying tissue must also be replaced. Local cutaneous flaps include the full thickness of the skin and the subcutaneous fatty tissue, and they can be raised in the immediate vicinity of the defect while maintaining the vascular supply to the base of the flap.
There are three basic types:
Advancement flaps.
Rotation flaps.
Transposition flaps.
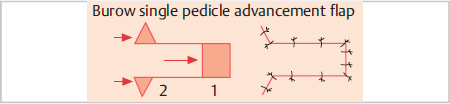
Advancement Flaps
Simple pedicled advancement flaps involve the dissection of cutaneous flaps that can be advanced into the defect parallel to their axis. The dimpling of the skin that occurs at the base of the flap, as it is advanced, can be compensated for by excising what are known as the Burow triangles at the base of the flap (▶Fig. 2.1). With the bipedicled advancement flap, also known as a bridge flap, the advancement is 90 degrees to the axis of the flap. Here, additional measures, such as skin grafting, may be required to cover the donor site defect.
V-Y Advancement Flap
The principle of the V-Y advancement flap (▶Fig. 2.2) is a gain in length at the expense of width. A V-shaped cutaneous flap with equal limbs is raised, mobilized, and approximated to the shape of a Y. The axis of the V-shaped flap must correspond to the axis of the advancement. A Y-V flap is the opposite. Here width is gained at the expense of length. After a Y-shaped incision is made, the central triangular tissue flap is approximated to the end of the vertical incision, forming a V.

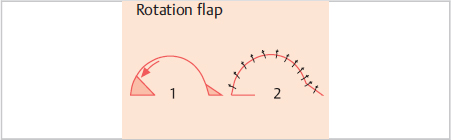
Rotation Flap
Rotation flaps are based on a defined axis of rotation around which the arc-like flap is swung into the adjoining defect. This requires integrating the respective existing defect into a triangular arc along the semicircular incision made to raise the rotation flap. This incision must be at least 5 times as long as the necessary advancement. The choice of the arc and the course of the incision should be determined by the available tissue and its vascular supply (▶Fig. 2.3).
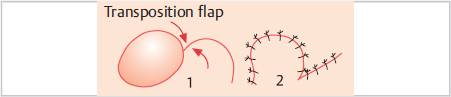
Transposition Flap
With axial pattern transposition flaps, the ratio of the flap’s length to its width is of decisive importance. To ensure sufficient perfusion, it should be between 2:1 and 2.5:1 in the genital region. Proper choice of the point of rotation and the length of the flap are also particularly important for successful treatment, as these factors significantly influence postoperative tension in the wound. The length of the flap should invariably be at least one-third longer than the length of the equivalent limb of the triangle to be covered.
With the transposition flap (▶Fig. 2.4), the axial cutaneous flap can be raised without regard to the defect to be covered and then rotated into the defect. Double transposition flaps involve a combination of two transposition flaps. The portion close to the defect is used to cover the defect, whereas the somewhat smaller portion farther away is used to cover the gap created by the closer portion as it is advanced into the defect. Such flaps are used particularly in cases in which the donor site of the first flap cannot be closed without tension simply by approximating the edges of the wound.
Rhomboid Flap
Rhomboid flaps are combinations of advancement and transposition flaps. The Limberg rhomboid flap (▶Fig. 2.5) is an axial pattern cutaneous flap that can be used to cover rhombus-shaped defects. In the shape of a parallelogram with four equal sides, it is raised as the extension of the short axis of the defect rhombus on the longitudinal side of the defect. The angle close to the defect is 120 degrees at maximum. The outer incision is made at an angle of 60 degrees parallel to the edge of the wound, and the length of the side corresponds to the dimensions of the defect. The flap is mobilized and rotated into the defect.
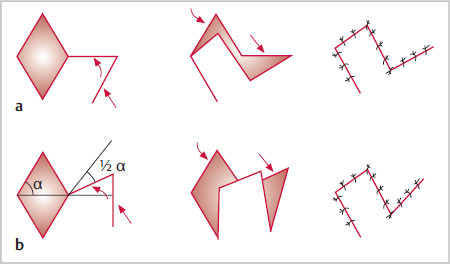
With the Dufourmentel flap, the flap angle close to the defect is 155 degrees. At a distance of about the length of one defect side, the outer incision is made parallel to the longitudinal axis of the rhombus-shaped defect at an angle of 60 degrees. Its length depends on the size of the defect and the tension at the site.
2.1.3 Fillers and Lipofilling in Genital Surgery
Treatment with injectable filler substances now accounts for a large share of all nonsurgical interventions. The materials in use today are high-molecular-weight compounds that exhibit significant differences in their physical and chemical behavior and are integrated into a complex matrix.
Therefore, a fundamental requirement for using fillers is to acquire a comprehensive understanding of the materials, their structure, their effect in tissue, and their longevity. In addition, the surgeon must of course have sufficient knowledge to correctly apply these materials and to manage any over- or undercorrection (▶Fig. 2.6).
Autologous fat transfer is a surgical procedure that involves not only harvesting the material but also processing and transplanting it. For this reason, it is necessary for the user to be proficient not only in the application but also in the technique of liposuction and the subsequent processing of the fatty tissue. This is important because these factors (i.e., the selection of the donor sites, quality of the fat cells, type of processing of the fatty tissue, transfer technique) all significantly influence the later result (▶Fig. 2.7).
Possible indications for the use of synthetic fillers or autologous fat transfer (lipofilling) include:
Tissue atrophy or dystrophy.
Congenital malformations or asymmetries.
Post-traumatic defects such as those secondary to genital mutilation, birth injuries, cancer surgery, or radiation therapy.
Desire (possibly for aesthetic reasons) to have the labia majora and minora augmented or the vagina narrowed.
Acute disease, especially infections in the region to be treated, coagulation disorders, or anticoagulant therapy are regarded as contraindications.
Planning Surgery and Treatment
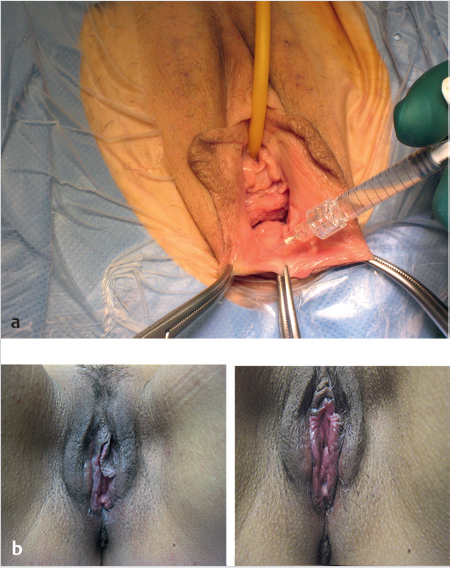
After appropriate examination, photographic documentation, and planning of the procedure, the patient must be thoroughly informed about the effect, the time of the onset of action, and the anticipated long-term effect. The patient’s expectations must be carefully documented, and the extent to which they can be fulfilled should also be discussed. In addition, the surgeon should of course discuss the possibility of complications in some detail and should inform the patient of the possible necessity for corrective or revision procedures (▶Fig. 2.8).

Given the broad range of fillers in the market, the final decision for one product or another must be made by the respective user. The surgeon should work with products that he or she is familiar with and should adapt the injection technique to the specific region to be treated. In most cases, superficial or local anesthesia will be sufficient for treatment in the vaginal or vulvar region. The injection should be done via a stab incision with atraumatic needles using a tunnel, fan, and tower technique.
Note
The medial aspects of the knees, medial and lateral thighs, the lower abdominal region, and to a certain extent the upper abdominal region and flanks as well, are regarded as suitable zones for harvesting autologous fat for transplantation.
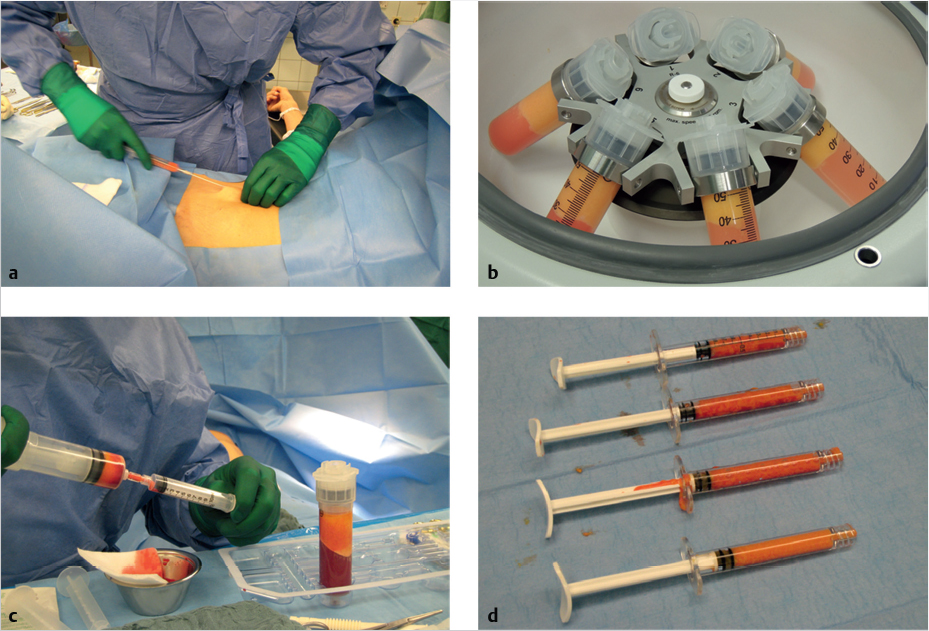
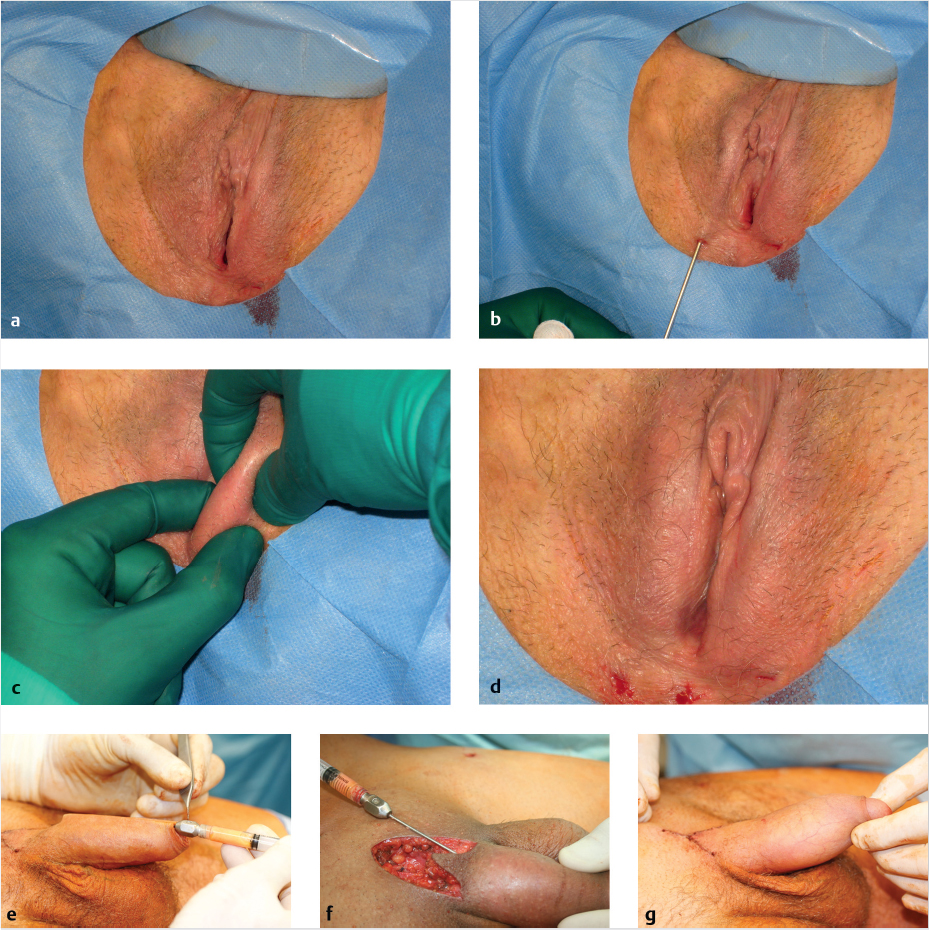
In the hospital, fatty tissue is usually removed under tumescent anesthesia. Different tumescent solutions are used here, but their basic ingredients include a 0.9% saline solution, a vasoconstrictor (such as epinephrine), a local anesthetic, and, in applicable cases, sodium bicarbonate. The solution can be adapted to different needs by varying the component substances. After introducing the tumescent solution into the donor site and waiting for an appropriate interval for the medication to take effect, the surgeon begins with the actual liposuction. This should be done with particular care, using constant low-intensity suction (− 0.5 bar) and a suction cannula with a diameter < 3 mm. Various systems are available for processing the harvested fatty tissue for further transplantation. All of them seek to optimize the quality of the aspirate in order to ensure a high rate of integration into the target tissue. After processing, the fatty tissue is injected through atraumatic needles into the target tissue, wherever possible in several layers, and distributed in a fan-shaped pattern (▶Fig. 2.9). The transplanted material can then be gently massaged into the tissue. Compression therapy of the donor site for 4 to 6 weeks postoperatively is recommended.
Caution
Compression therapy for the penis or in the vaginal or vulvar region has not proven to be effective for the integration of the transplanted tissue.
Complications
Aside from general complications, such as hematomas and local infections, the use of fillers may also be associated with short- and long-term incompatibility reactions such as itching, swelling, erythema, or foreign-body granulomas. With lipofilling, surface irregularities can occur at both the donor site and the recipient site. Severe infections such as necrotizing fasciitis are as rare as fat embolisms or extensive skin necrosis, yet these risks must be discussed prior to surgery when obtaining the patient’s informed consent. As the final result of lipofilling depends significantly on the speed of healing of the grafted fatty tissue, the patient should be informed that the procedure may have to be repeated in certain cases.
Further Reading
[1] Burke TW, Morris M, Levenback C, Gershenson DM, Wharton JT. Closure of complex vulvar defects using local rhomboid flaps. Obstet Gynecol. 1994; 84(6):1043–1047 [2] Lister GD, Gibson T. Closure of rhomboid skin defects: the flaps of Limberg and Dufourmentel. Br J Plast Surg. 1972; 25(3): 300–314 [3] Mathes SJ, Nahai F. Classification of the vascular anatomy of muscles: experimental and clinical correlation. Plast Reconstr Surg. 1981; 67 (2):177–187 [4] Moschella F, Cordova A. Innervated island flaps in morphofunctional vulvar reconstruction. Plast Reconstr Surg. 2000; 105(5):1649–1657 [5] Rutledge F, Sinclair M. Treatment of intraepithelial carcinoma of the vulva by skin excision and graft. Am J Obstet Gynecol. 1968; 102(6): 807–818 [6] Salgado CJ, Tang JC, Desrosiers AE, III. Use of dermal fat graft for augmentation of the labia majora. J Plast Reconstr Aesthet Surg. 2012; 65 (2):267–270 [7] Sterry W, Burgdorf W, Worm M. Checkliste. Dermatologie. 7th ed. Stuttgart: Thieme; 2014 [8] Vogt PM, Herold C, Rennekampff HO. Autologous fat transplantation for labia majora reconstruction. Aesthetic Plast Surg. 2011; 35(5):913–915 [9] vom Dorp F, Rübben H, Krege S. Free skin grafts as alternatives in reconstructive plastic surgery of the genitalia. Urologe A. 2009; 48 (6):637–6442.1.4 Laser Therapy
Laser therapy has enjoyed increasing popularity in dermatology over past two decades. Looking at the applications of this technique, we can identify quite clearly defined, proven scenarios for noninvasive laser therapy. These include:
Reduction of wrinkles.
Skin lift.
Vascular therapy.
Hair removal.
Removal of undesirable tattoos or even pigmented lesions. These applications illustrate, rather comprehensively, the effect of laser energy on the skin; at least the noninvasive techniques of hair removal and treatment of pigmented layers of skin can also be applied without modification to the genital region. Both the procedure and the mode of action are identical in these cases. Added to this are the recently developed colporrhaphy techniques and procedures for treating slight to moderate stress incontinence. They bear a certain similarity to dermatologic nonablative skin-lifting procedures. However, the applicators and the application are so dissimilar that we can justifiably speak of a new application of laser energy.
The basis for all these applications is the effect of laser energy. Laser energy can produce quite different effects depending on its wavelength. A laser application can be classified by its mode of action as either ablative or nonablative.
Ablation
Ablation of skin is performed almost exclusively with Er:YAG lasers with a wavelength of 2,940 nm or CO2 lasers with a wavelength of 10,600 nm.
Er:YAG Laser
The Er:YAG (erbium:yttrium–aluminum–garnet) laser is a solid medium laser that generates its laser light by means of an Er:YAG crystal intensively excited by flashing lamps. The Er:YAG laser usually delivers its energy in pulses. Typical pulse repetition frequencies lie between 2 and 20 Hz whereby some units can achieve pulse frequencies of up to 50 Hz. The duration of the individual pulses is often about 300 µs. With structural modifications it is possible to produce Er:YAG lasers with variable pulse durations. By varying the frequency and pulse duration, it is possible to achieve a very finely adjustable ablation characteristic with an Er:YAG laser. Accordingly, units with a broad frequency range and a variety of pulse duration settings are superior to those with fixed pulse durations and a narrow frequency range.
CO2 Laser
The CO2 laser produces its laser energy in a tube filled with a CO2 gas mixture that is excited by high-frequency electric current. The CO2 laser is a continuous beam laser that delivers its energy continuously. To operate a CO2 laser in pulsed mode, the energy delivery is switched on and off. This makes it possible to produce pulses even in the millisecond range.
Water as the Target Structure
Both types of lasers have a common target structure. Their energy is absorbed by the water molecules in the tissue, causing them to immediately heat up and vaporize. This makes it possible to remove tissue in extremely fine layers. The effects of wavelengths in tissue are unspecific. The difference between them consists in their affinity to their target structure, water.
Varying Absorption Coefficients
The Er:YAG wavelength with an absorption coefficient of 12,800 cm−1 corresponds to the maximum absorption of water. The CO2 laser has an absorption coefficient of 800 cm−1. As a result, the absorption of Er:YAG laser light in tissue is 10 times higher than that of the CO2 laser. 2 Since the Er:YAG laser as a solid medium laser has significantly shorter pulse durations that the CO2 gas laser, the pulse power values for the Er:YAG laser are also significantly higher. The optical penetration depth of the Er:YAG lasers in tissue is about 2 to 5 µm, whereas that of the CO2 laser is about 20 to 30 µm. In terms of practical application, this also means that the Er:YAG laser causes little or no thermal damage beyond the ablated tissue itself.
Nonablative Effects
Nonablative photothermic applications are based on the principle that the laser energy damages the target tissue to such an extent that it atrophies or is removed. The concept of “selective photothermolysis” plays a crucial role in the nonablative applications of laser energy in dermatology.
Selective Photothermolysis
The idea of selective photothermolysis is based on the principle of avoiding damage to any tissue other than the target structure. This also applies when the energy cannot be selectively applied, for example, in cases where the beam must first pass through superficial layers of skin before reaching the target tissue. The solution is to select a wavelength that will be absorbed well into the target structure while it will pass through the superficial layer of skin with minimal loss. 1
Thermal Relaxation Time
Another important factor in selective photothermolysis, aside from the selected wavelength, is the “thermal relaxation time.” The thermal relaxation time is the exact time required to produce maximum heat in the target structure without causing damage to surrounding tissue due to heat conduction. The thermal relaxation time varies according to the volume and nature of the target structure (▶Table 2.2).
Homogeneous Photothermolysis
In contrast to selective photothermolysis, the effect of homogeneous photothermolysis is unspecific as in hyperthermia. This describes the phenomenon that even laser wavelengths that do not act selectively can be used to produce targeted thermal effects.
Noninvasive Laser Therapy in the Genital Region
Hair Removal
Primarily, alexandrite lasers (755 nm), diode lasers (810 and 980 nm), or Nd:YAG (neodymium:yttrium–aluminum–garnet) lasers (1,064 nm) are used for hair removal. All of these lasers emit their energy in pulses of different wavelengths. The thermal relaxation time of a hair follicle is specified as 90 ms. Hair removal lasers emit their energy in long pulses corresponding to this time span. Pulse lengths between 20 and 50 ms are typically used for this purpose. Although the energy densities used in therapy reflect the different absorption coefficients of the individual wavelengths, they all are of the same order of magnitude. The therapeutic spectrum ranges from 20 to 30 J/cm2 with the alexandrite laser, 20 to 50 J/cm2 with the 810 diode laser, and up to 30 to 60 J/cm2 with the Nd:YAG laser.
It is not possible to give a clear recommendation for a wavelength on the basis of clinical results. One may consider giving preference to the Nd:YAG laser due to the higher proportion of pigmented skin in the genital region. Compared with the shorter wavelengths, this laser is best even for use with darker types of skin.
Note
With all the wavelengths mentioned, it is important to cool the skin during the application.
Although the energy densities required for hair removal are tolerable for the patient, they are not pleasant. Furthermore, an instant of carelessness can lead to thermal damage to the epidermis.
Tattoos in the Genital Region
Removing tattoos with lasers represents a minimally invasive and efficient form of therapy. Given the size of the pigment particles ranging between 0.1 and 10 µm, the thermal relaxation time is accordingly short. Therefore, lasers with pulse durations in the picosecond and nanosecond range should only be used when removing tattoos. Common types of lasers used for this include the ruby, alexandrite, pulsed dye, Nd:YAG, and potassium titanyl phosphate (KTP) lasers. All systems used for removing tattoos have high pulse power (up to several hundred megawatts). Undesired side effects cannot be ruled out because the composition of the respective pigment to be removed is usually unknown and how it reacts becomes apparent only after the first attempt at treatment. Pigments have also been known to change color after laser treatment. Scarring can also occur, especially if several successive layers of pigment are found at the site.
Removal of Pigmented Lesions
There are two therapeutic options for removing pigmented lesions. One is to use an appropriately adjusted laser such as those used for removing tattoos. Due to its wavelength, the KTP laser with 532 nm of energy may be considered, because this wavelength is absorbed well by melanin. The energy goes directly into the pigment and destroys it. This procedure has the advantage that this type of laser acts selectively on the pigment, leaving the adjacent tissue largely unaffected. The effect is totally different when pigmented lesions are removed with an ablative laser. The action of both CO2 and Er:YAG lasers on biologic tissue is unspecific due to its water content. Thus, it is ultimately up to the physician to remove as little tissue as possible. For this application, the Er:YAG laser has the advantage of being able to remove tissue without leaving behind an area of thermal tissue damage.
Complications and Complication Management
Patients often describe a brief sensation of pain accompanying treatment. However, this sensation is limited to the duration of the laser pulse. This can be addressed by cooling before, during, and after therapy or with topical anesthesia. Cooling wraps or a cold air fan are suitable for this purpose. Some units also include an integral cooling device. Suitable cooling not only reduces pain but also prevents epidermal injury. Transient side effects include swelling, erythema, blistering, and crusting. Manipulation of the treated area by the patient in such cases can lead to infection, pigment changes, and scarring. In such cases, antimicrobial or disinfectant topical agents are recommended to manage the crusts and prevent bacterial superinfection.
Other possible side effects that, in rare cases, can become permanent include pigment changes (hypopigmentation or hyperpigmentation) that can occur when the light parameters are not properly adapted to the skin type. Patients who must avoid exposure to UV light because of their skin type, a known hypersensitivity to light, an existing suntan (whether from sun or indoor tanning), should not be treated. Scarring is theoretically possible but has rarely been described. Usually it is a sequela of unsuitable light parameters or manipulation where crusting has occurred. Any nevocytic or melanocytic lesions located in the target area to be treated should be spared. Thorough abstinence to UV light or adequate protection against it must be ensured during the entire duration of treatment.
Further Reading
[1] Anderson RR, Parrish JA. Selective photothermolysis: precise microsurgery by selective absorption of pulsed radiation. Science. 1983; 220(4596):524–527 [2] Kaufmann R, Hartmann A, Hibst R. Cutting and skin-ablative properties of pulsed mid-infrared laser surgery. J Dermatol Surg Oncol. 1994; 20(2):112–118 [3] Kaufmann R, Hibst R. Pulsed Erbium:YAG laser ablation in cutaneous surgery. Lasers Surg Med. 1996; 19(3):324–330 [4] Landthaler M, Hohenleutner U. Lasertherapie in der Dermatologie. 2. Aufl. Berlin: Springer; 19992.2 Flaps from the Lower Abdominal and Inguinal Region
2.2.1 Myocutaneous Rectus Abdominis Flaps (VRAM, TRAM)
Anatomy
The deep inferior epigastric artery provides the vascular supply to rectus abdominis flaps. This artery arises from the external iliac artery at the level of the inguinal ligament, then courses superiorly together with the inferior epigastric artery medial to the deep inguinal ring in the lateral umbilical fold. Then it passes through the fascia of the transversus abdominis and courses along the posterior aspect of the rectus abdominis, into which it gives off numerous perforators in the direction of the abdominal wall. It continues until it reaches the level of the umbilicus where its branches anastomose with the branches of the superior epigastric artery.
A paired muscle, the rectus abdominis has its origin on the anterior surface of the fifth to seventh costal cartilages and the xiphoid process. Its insertion is between the pubic tubercle and symphysis. The superior epigastric artery and vein provide the vascular supply to the superior portion of the muscle, the inferior epigastric artery and vein supply its inferior portion (▶Fig. 2.10).
Technique
The procedure is performed with the patient in supine position under general anesthesia. In applicable cases this is done with the option of placing the patient in the lithotomy position to facilitate simultaneously raising the flap and preparing the vulvoperineal region.
Rectus abdominis flaps (Mathes–Nahai type II) lend themselves to covering large, deep defects from the groin and into the perineal region as well as the entire pelvic floor. With or without a skin island, the flap pedicled on the deep inferior epigastric artery can be passed over the symphysis to cover vulvoperineal defects as well as delivered through a transpelvic route to cover defects of the pelvic floor.
For covering defects in the vulvoperineal region, the rectus abdominis can either be used as a muscle flap, in applicable cases in combination with a split-thickness skin graft, or as a myocutaneous flap. The decision in each case is based on the size of the defect and the thickness of the subcutaneous fatty tissue. In cases where the subcutaneous tissue is quite pronounced and the dominant perforators are not spared, reduced perfusion can result and, in rare cases, partial necrosis of the skin island may occur. In addition, the size of a myocutaneous flap can necessitate secondary correction and level adjustment of the flap by means of liposuction and/or thinning of the flap.
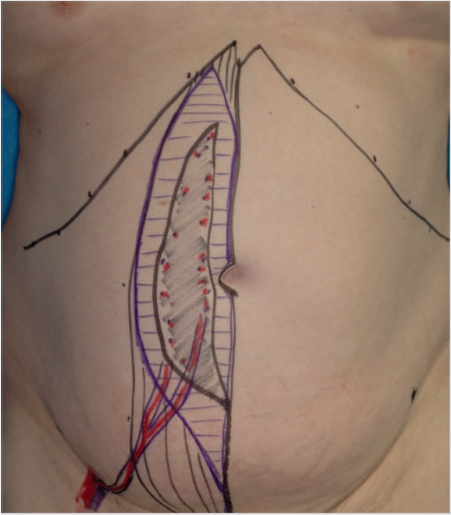
Where conditions require a myocutaneous flap, the alignment of its skin island is determined by the size and position of the defect to be covered. Transverse rectus abdominis muscle (TRAM) flaps, vertical rectus abdominis muscle (VRAM) flaps (▶Fig. 2.11), and angled skin islands are used for this purpose.
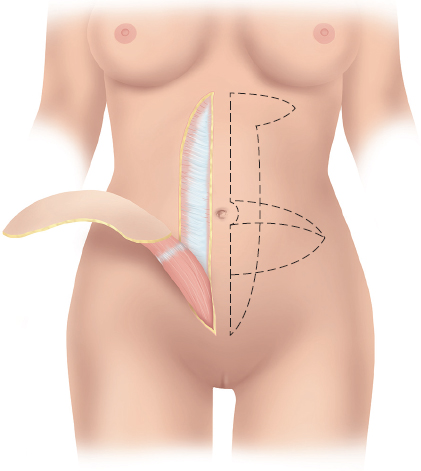
A TRAM flap is raised taking along a skin island bounded inferiorly by the pubic bone (Pfannenstiel incision) and the inguinal ligaments, laterally by the anterior superior iliac spine (ASIS), and superiorly by a line just below or above the umbilicus. With the VRAM flap, longitudinal paramedian skin islands aligned with the rectus abdominis are dissected.
In all these cases, the flap is raised by beginning laterally and carrying the dissection medially. As soon as enough perforators have been exposed at the level of the rectus sheath, the sheath is incised longitudinally lateral to the perforators. In the subsequent dissection from the opposite side, the medial perforators of the ipsilateral muscle are also spared by means of a longitudinal incision in the fascia medial to the perforators. After this, the rectus abdominis with the skin island superficial to it are dissected off the posterior rectus sheath. Superiorly, the muscle is then divided at the superior margin of the respective skin island, and the superior epigastric artery and vein supplying it are ligated. The dissection then continues inferiorly. Inferiorly, the inferior epigastric artery usually enters the lateral rectus sheath with two accompanying veins.
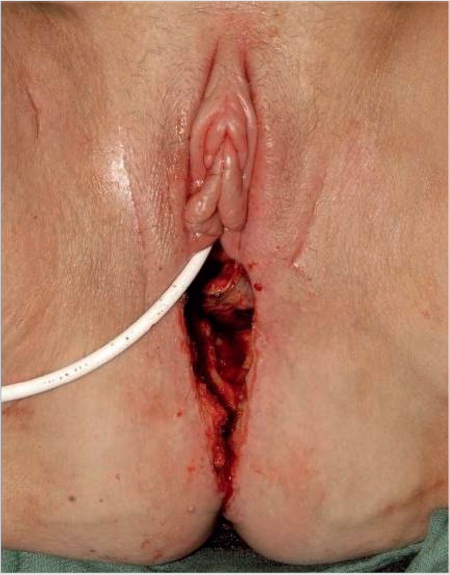
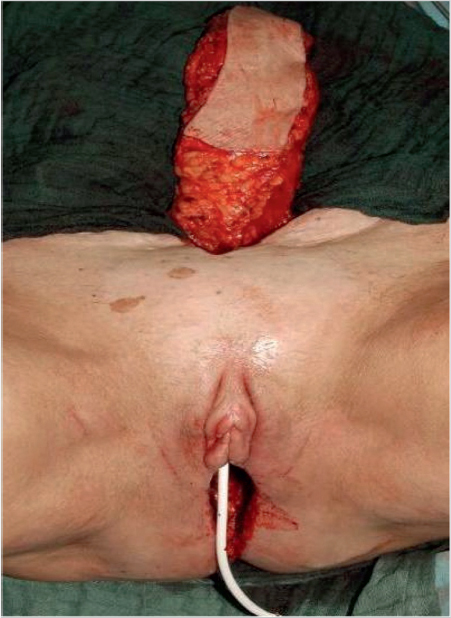
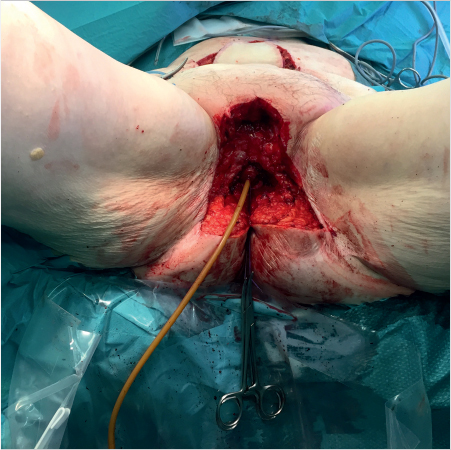
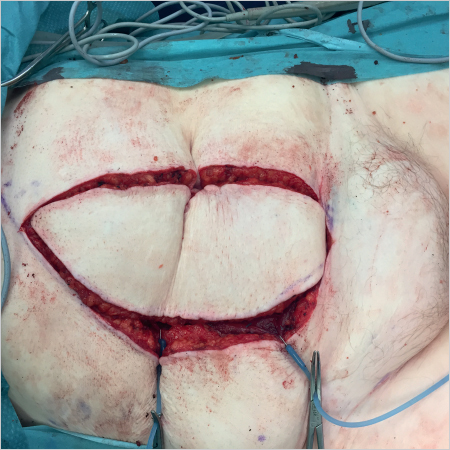
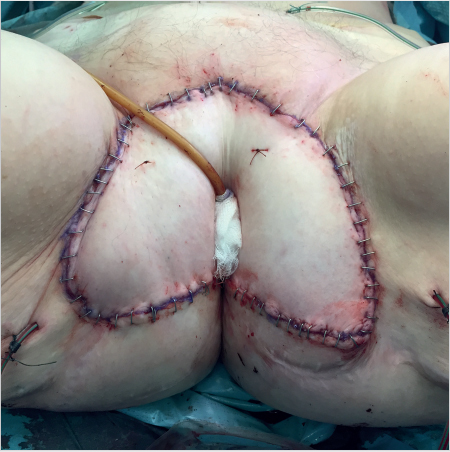
After the flap has been completely dissected and mobilized, it can be passed beneath the skin over the pubic symphysis or through a transpelvic route and rotated into the respective defect. This second option is particularly suitable for covering defects from exenteration that require reconstruction of the posterior vaginal wall (▶Fig. 2.12, ▶Fig. 2.13, ▶Fig. 2.14, ▶Fig. 2.15, ▶Fig. 2.16, ▶Fig. 2.17). The rectus sheath is closed with a running suture, or with addition of a mesh (e.g., Vicryl mesh) if a larger section of fascia was removed. Closing the donor site defect of a TRAM flap requires undermining the remaining abdominal wall to a point inferior to the costal arch. This is done to allow placement of suction drains and primary closure of the wound in layers. The donor site defects of some VRAM flaps and angled flaps can be closed without further dissection of the abdominal wall, which in the remaining cases in undermined laterally. In the presence of extensive superfluous abdominal skin, closure can be combined with a fleur-de-lis abdominoplasty (▶Table 2.3).



Possible Complications
General complications that can occur secondary to a rectus abdominis flap include:
Hematoma.
Seroma.
Infections.
Impaired wound healing.
Partial necrosis in the region of the skin island can occur in rare cases, as can late scarring problems with stenosis of the introitus.
Caution
Additional problems may occur due to the weakening of the abdominal wall, particularly when the reconstruction was done without mesh.
2.2.2 Deep Inferior Epigastric Artery Perforator Flap
The operation involves dissecting one to three perforators of the inferior epigastric artery while sparing the abdominal wall musculature. In contrast to pedicled VRAM and TRAM flaps, no weakening of the anterior abdominal wall is to be expected with this method.
Anatomy
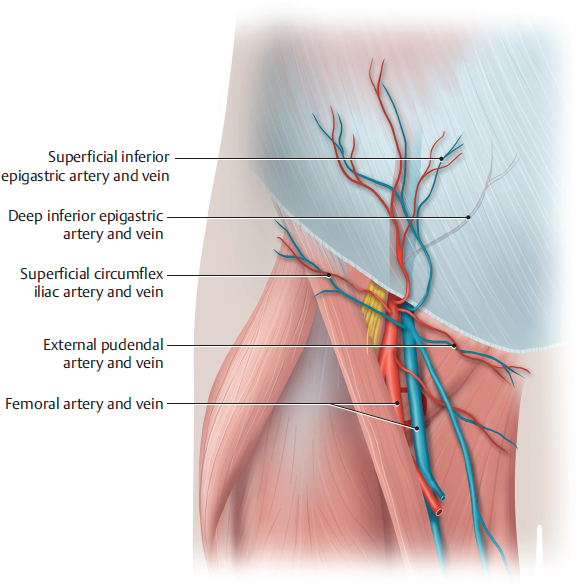
The blood supply to the skin and subcutaneous tissue of a deep inferior epigastric perforator (DIEP) flap is provided by perforators of the inferior epigastric artery that arises from the external iliac artery. The artery usually gives off an anterior branch and a lateral branch and then courses along the underside of the rectus abdominis. Other than the inferior epigastric artery, the superficial inferior epigastric artery (SIEA) also supplies the skin and subcutaneous tissue from the lower abdomen. This artery has its origin about 3 cm inferior to the inguinal ligament, arising directly from the femoral artery or from a common trunk with the superficial circumflex iliac artery. The SIEA courses through the Scarpa fascia superior to the inguinal ligament within the superficial subcutaneous tissue. Along its entire course, the artery lies parallel to and beneath an accompanying vein that drains directly into the venous confluence. The superficial epigastric vein is the largest vein that drains blood from the DIEP flap. With ideal vascular caliber, the superficial epigastric artery and vein will also provide adequate blood supply to the adipocutaneous lower abdominal flap for vulvar reconstruction.
Given the variability of the perforators’ exact location, diameter, and blood flow, preoperative visualization by means of color duplex sonography or computed tomography (CT) angiography is recommended. Alternatively, their location can be marked preoperatively with the aid of Doppler ultrasound.
Like the rectus abdominis flap, the DIEP flap can be raised with a horizontal or vertical skin island. The greater portion of the future flap should lie within the area supplied by the selected perforator. The size and shape of the skin island should be adapted to individual patient.
Technique
The operation is performed with the patient in the lithotomy position with arms at the sides. The technique is identical to that of a perforator flap for breast reconstruction. The flap is incised according to the preoperative marking. The superficial epigastric vein in the region of the inferior incision can often be spared. This ensures additional venous drainage from the flap. If the caliber of the SIEA appears sufficient, it can be dissected and mobilized along a length of 5 to 6 cm together with the accompanying vein. A lower abdominal flap as large as a DIEP flap can then be raised, which will be supplied by these vessels (▶Fig. 2.18, ▶Fig. 2.19, ▶Table 2.4).
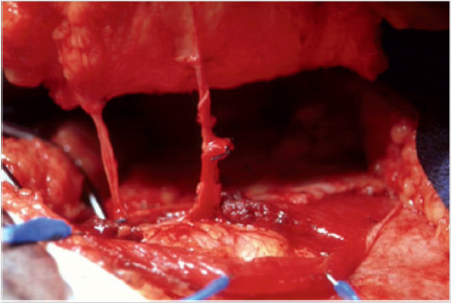
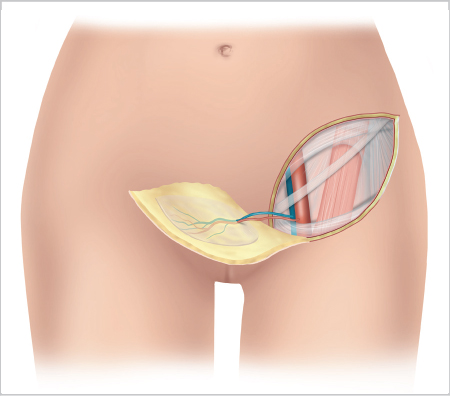
The skin and subcutaneous tissue are dissected off the fascia of the external oblique as far as the lateral margin of the rectus abdominis. After this the dissection must be performed with greater caution. Further dissection progressively exposes smaller vessels that arise from the perforator (▶Fig. 2.20). If preoperative color duplex sonography or CT angiography was performed, then the dissection can be quickly carried to the respective perforator. If not, then as many as possible of the lateral row of perforators should be exposed before selecting the largest or two larger ones. As a rule, larger gaps in the fascia are indicative of a larger perforator. If several perforators appear suitable then their size will be the decisive criterion. The largest perforator should be selected in each case. The vessels should be at least about 1.5 mm in diameter. Also note whether there are two or more perforators in a row arising from a common trunk of the inferior epigastric artery. Exposing two perforators has an advantage: A bilateral vulvar defect can then be covered by dividing the flap in the middle, with each half receiving its blood supply from one perforator.
After a suitable perforator has been identified, the anterior rectus sheath is incised parallel to the rectus abdominis close to where the vessels pass through it. A small gap often present in the fascia in the inferior portion of the perforator foramen facilitates entry. If the gap in the fascia is very small and the vessel is adherent, the fascia can be incised lateral to the perforator and a small piece of fascia can be left around the artery. If there are several perforators in a row, the incisions can be combined with each other. When mobilizing the anterior aspect of the rectus sheath, it is important to proceed with an adequate view because the vessels can course immediately beneath it for a variable distance before entering the muscle. The perforator can now be completely exposed, partially by blunt dissection and partially by bipolar diathermy. The dissection continues in this manner until the perforator reaches a main branch of the inferior epigastric artery on the posterior aspect of the rectus abdominis. The further procedure is identical that for a rectus abdominis flap (▶Fig. 2.21).
Possible Complications
The general complications, such as hematomas and seromas, impaired wound healing, infections, and scarring problems, are the same as those that can occur with a rectus abdominis flap. Partial necrosis of the flap can also occur where it is supplied by small-caliber perforators (< 1 mm). No significant weakening of the anterior abdominal wall is to be expected with a standard DIEP flap. Pedicled flaps supplied by a very superior proximal perforator are an exception to this rule. Dissecting them to expose a long vascular pedicle may require dividing motor nerve branches. Any nerves divided during the dissection should be immediately coapted using microsurgical techniques.
2.2.3 Mons Pubis and Suprapubic Flap
Anatomy
Flaps from the region of the mons pubis and the suprapubic abdomen receive their vascular supply via the superficial external pudendal artery (SEPA) and the SIEA. The SEPA arises from the common femoral artery, passes through the fascia below the inguinal ligament, and branches into the subcutaneous tissue of the lower abdomen and anterior perineum. Their terminal branches anastomose in the lower abdomen with the contralateral SEPA and the terminal branches of the superficial epigastric artery, and in the anterior perineum with those of the superficial and deep perineal arteries. The SIEA also arises from the femoral artery below the inguinal ligament, but after passing through the fascia it courses above the inguinal ligament and continues superiorly within the abdominal fascia.
Technique
The mons pubis transposition flap (▶Fig. 2.22a), because of its reliable vascularization as an axial pattern flap, is suitable for covering unilateral defects of anterior vulvoperineal region, the anterior commissure, and the labia majora and minora. The median line extending from the anterior commissure of the labia provides a guide for the base of the flap. The flap can be raised either ipsilateral or contralateral to the defect. The inferior limb of the flap is invariably dissected parallel and superior to the inguinal ligament. In the deep layer, the dissection extends beyond the Scarpa fascia as far as the superficial abdominal fascia. This makes it possible to raise adipocutaneous transposition flaps measuring 9 × 3 cm (length × width) and rotate them into the respective defect. It should be possible to close the donor site defect with a primary suture. If necessary, the mons pubis transposition flap can also be dissected as a transpubic island flap. To do so, the flap pedicle in what will be the subcutaneous regions is de-epithelialized and rotated into the defect.
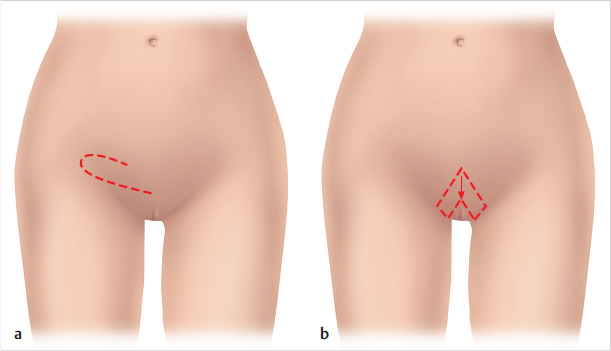
The mons pubis V-Y flap (▶Fig. 2.22b) can be used to cover an oval, preferably symmetrical, defect in the anterior vulvoperineal region, anterior commissure, and the labia majora and minora in which the urethra and vaginal introitus remain intact. The flap borders anteriorly on the defect and is raised as an adipocutaneous inverted V flap, whereby its posterolateral extensions must cover the entire width of the defect yet only two-thirds of its length. After incising around the skin island, the surgeon mobilizes it from the underside and dissects the posterolateral limbs. Then the skin island is advanced and the posterolateral limbs are rotated medially into the defect. Both the donor site on the mons pubis and the two lateral limbs can be closed with primary sutures.
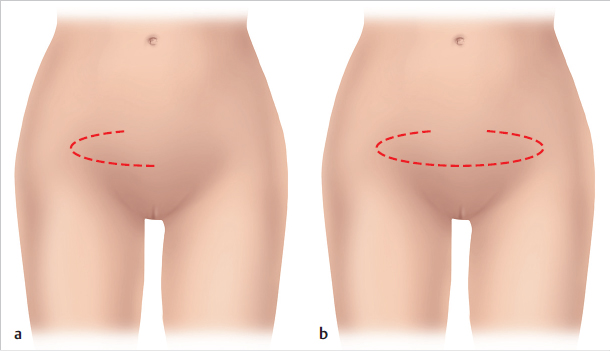
The suprapubic transposition flap, which is supplied primarily by the SIEA, can be used to cover defects of the anterior vulvoperineal region, anterior commissure, and labia majora and minora. The flap can be raised and used unilaterally and even bilaterally, especially after flap delay. With this flap, the inferior limbs of the flap extend laterally along the border of the pubic hair. In the deep layer, the dissection extends as far down as the superficial abdominal fascia. Flaps measuring 10 × 4 cm (length × width) can be raised, whereby the donor site defect can usually be closed with a primary suture. Particularly for isolated reconstruction of the labia majora, this flap can be used both unilaterally and bilaterally as a transpubic island flap (▶Fig. 2.23a, b). Here as well, the portion of the pedicle that will be in the subcutaneous region is de-epithelialized and the resulting distal skin island is used to reconstruct the labia majora (▶Table 2.5).
Possible Complications
General complications that can occur secondary to all variations of an external pudendal artery flap include:
Hematoma.
Seroma.
Infections.
Impaired wound healing.
Partial necrosis of the flap can occur, as can scarring problems.
2.2.4 Groin Flaps
Anatomy
The arterial supply to the groin (inguinal) flap is provided by the superficial circumflex iliac artery. This artery arises from the femoral artery about 2 cm distal to the inguinal ligament, penetrates the fascia at the medial margin of the sartorius, and then courses through the subcutaneous tissue to the iliac crest (▶Fig. 2.24).
Technique
The flap design uses the inguinal ligament as its longitudinal axis, from the palpable pulse of the femoral artery to the anterior superior iliac spine. A long vascular pedicle is required for paragenital or perineal reconstructions. To do this, the incision is extended inferiorly and medially, and the fascia of the sartorius is divided and integrated into the flap. Presence of a large circumflex iliac artery will allow the surgeon to raise a correspondingly long flap. The lateral portion of the inguinal flap is supplied by a vascular network corresponding to the lateral extension of the superficial circumflex iliac artery. This allows dissection of flaps measuring 30 × 10 cm (length × width). The dissection is initially epifascial and is carried from superolateral to inferomedial. Upon reaching the lateral margin of the sartorius, the surgeon incises the muscular fascia longitudinally and continues the dissection, taking along the fascia, until the vascular pedicle arises medial to the sartorius. The flap is then further mobilized on this pedicle. The flap raised in this manner can then be rotated 120 to 180 degrees inferiorly on its vascular pedicle and sutured into the defect. Secondary adaption and shaping with thinning by liposuction may be required (▶Fig. 2.25, ▶Table 2.6).
Principle | Pedicled adipocutaneous flap |
Vascular supply | Superficial circumflex iliac artery |
Maximum size (length × width) | 30 × 10 cm |
Indication | Unilateral defects in the vulvoperineal region |
Further Reading
[1] Bertani A, Riccio M, Belligolli A. Vulval reconstruction after cancer excision: the island groin flap technique. Br J Plast Surg. 1990; 43(2): 159–161 [2] Buchel EW, Finical S, Johnson C. Pelvic reconstruction using vertical rectus abdominis musculocutaneous flaps. Ann Plast Surg. 2004; 52 (1):22–26 [3] Cardosi RJ, Hoffman MS, Greenwald D. Rectus femoris myocutaneous flap for vulvoperineal reconstruction. Gynecol Oncol. 2002; 85(1): 188–191 [4] Carlson JW, Carter JR, Saltzman AK, Carson LF, Fowler JM, Twiggs LB. Gynecologic reconstruction with a rectus abdominis myocutaneous flap: an update. Gynecol Oncol. 1996; 61(3):364–368 [5] Cheng A, Saint-Cyr M. Split and thinned pedicle deep inferior epigastric perforator (DIEP) flap for vulvar reconstruction. J Reconstr Microsurg. 2013; 29(4):277–282 [6] Fang BR, Ameet H, Li XF, et al. Pedicled thinned deep inferior epigastric artery perforator flap for perineal reconstruction: a preliminary report. J Plast Reconstr Aesthet Surg. 2011; 64(12):1627–1634 [7] Hatoko M, Okazaki T, Tada H, et al. Vulval reconstruction using rectus abdominis musculocutaneous flap transfer with secondary liposuction in extramammary Paget’s disease. Ann Plast Surg. 1997; 38(2): 179–183 [8] Haynes DF. Trans-pubic abdominal flap for reconstruction of the labia majora. J Plast Reconstr Aesthet Surg. 2011; 64(11):1537–1539 [9] Höckel M, Schmidt K, Bornmann K, Horn LC, Dornhöfer N. Vulvar field resection: novel approach to the surgical treatment of vulvar cancer based on ontogenetic anatomy. Gynecol Oncol. 2010; 119(1):106–113 [10] Kuokkanen H, Mikkola A, Nyberg RH, Vuento MH, Kaartinen I, Kuoppala T. Reconstruction of the vulva with sensate gluteal fold flaps. Scand J Surg. 2013; 102(1):32–35 [11] Lazzaro L, Guarneri GF, Rampino Cordaro E, et al. Vulvar reconstruction using a “V-Y” fascio-cutaneous gluteal flap: a valid reconstructive alternative in post-oncological loss of substance. Arch Gynecol Obstet. 2010; 282(5):521–527 [12] Lee PK, Choi MS, Ahn ST, Oh DY, Rhie JW, Han KT. Gluteal fold V-Y advancement flap for vulvar and vaginal reconstruction: a new flap. Plast Reconstr Surg. 2006; 118(2):401–406 [13] Lee JH, Shin JW, Kim SW, et al. Modified gluteal fold V-Y advancement flap for vulvovaginal reconstruction. Ann Plast Surg. 2013; 71(5): 571–574 [14] Moschella F, Cordova A. Innervated island flaps in morphofunctional vulvar reconstruction. Plast Reconstr Surg. 2000; 105(5):1649–1657 [15] Muneuchi G, Ohno M, Shiota A, Hata T, Igawa HH. Deep inferior epigastric perforator (DIEP) flap for vulvar reconstruction after radical vulvectomy: a less invasive and simple procedure utilizing an abdominal incision wound. Ann Plast Surg. 2005; 55(4):427–429 [16] Nakamura Y, Ishitsuka Y, Nakamura Y, et al. Modified gluteal-fold flap for the reconstruction of vulvovaginal defects. Int J Dermatol. 2010; 49(10):1182–1187 [17] Nelson RA, Butler CE. Surgical outcomes of VRAM versus thigh flaps for immediate reconstruction of pelvic and perineal cancer resection defects. Plast Reconstr Surg. 2009; 123(1):175–183 [18] Persichetti P, Simone P, Berloco M, et al. Vulvo-perineal reconstruction: medial thigh septo-fascio-cutaneous island flap. Ann Plast Surg. 2003; 50(1):85–89 [19] Potkul RK, Barnes WA, Barter JF, Delgado G, Spear SL. Vulvar reconstruction using a mons pubis pedicle flap. Gynecol Oncol. 1994; 55 (1):21–24 [20] Pursell SH, Day TG, Jr, Tobin GR. Distally based rectus abdominis flap for reconstruction in radical gynecologic procedures. Gynecol Oncol. 1990; 37(2):234–238 [21] Salgarello M, Farallo E, Barone-Adesi L, et al. Flap algorithm in vulvar reconstruction after radical, extensive vulvectomy. Ann Plast Surg. 2005; 54(2):184–190 [22] Santanelli F, Paolini G, Renzi L, Persechino S. Preliminary experience in reconstruction of the vulva using the pedicled vertical deep inferior epigastric perforator flap. Plast Reconstr Surg. 2007; 120(1): 182–186 [23] Spear SL, Pellegrino CJ, Attinger CE, Potkul RK. Vulvar reconstruction using a mons pubis flap. Ann Plast Surg. 1994; 32(6):602–605 [24] Ulrich D, Pallua N. Brustrekonstruktion mit dem Deep Inferior Epigastric Artery Perforator (DIEAP)-Lappen. In: Krupp S, Rennekampff HO, Pallua N, Hrsg. Plastische Chirurgie, Klinik und Praxis. 31. Erg. Lfg.6/08, VI-4.4: 1–20 [25] Weiwei L, Zhifei L, Ang Z, Lin Z, Dan L, Qun Q. Vaginal reconstruction with the muscle-sparing vertical rectus abdominis myocutaneous flap. J Plast Reconstr Aesthet Surg. 2009; 62(3):335–3402.3 Flaps from the Vulvoperineal Region
2.3.1 Internal Pudendal Artery Flaps
Anatomy
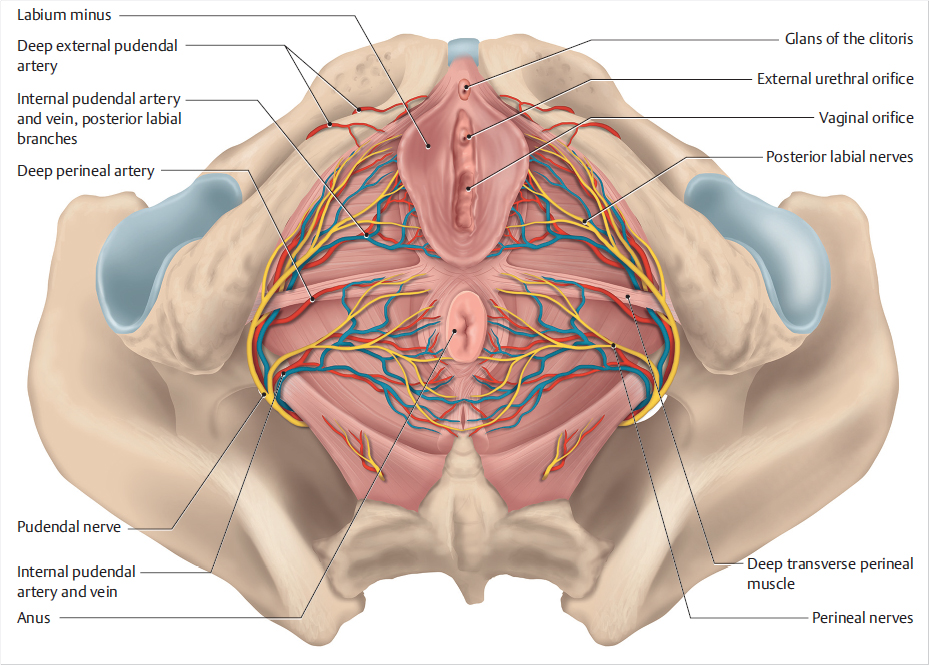
The posterior vulvoperineal region is supplied by the internal pudendal artery (IPA), a branch of the internal iliac artery. This artery enters the posterior pelvic floor through the pudendal canal (canal of Alcock) deep to the gluteus maximus. It then branches into the superficial perineal and deep perineal arteries. The superficial perineal artery courses anteriorly across the superficial transverse perineal muscle. Its terminal branches (the posterior labial branches) supply the posterior portion of the labia. The deep perineal artery passes through the urogenital diaphragm formed by the superficial and deep transverse perineal muscles and then courses anteriorly. The IPA measures about 10 to 12 cm in length with a diameter of about 1 to 1.5 mm. The region takes its sensory innervation from the pudendal nerve. This nerve follows the course of the IPA and gives rise to the perineal nerve whose superficial branch gives off the labial nerves that supply the perineum and labia (▶Fig. 2.26).
Technique
The vascularization of IPA flaps makes them suitable for covering both unilateral and bilateral defects in the entire vulvoperineal region. The base of all flaps from the posterior vulvoperineal region lies within a triangle whose apexes are defined by the vaginal introitus, anus, and ischial tuberosity. The density of vascular anastomoses and perforating arteries in this region makes it possible to raise a broad range of flaps. Even after a previous flap procedure, it is often possible to raise a second flap in the vicinity.
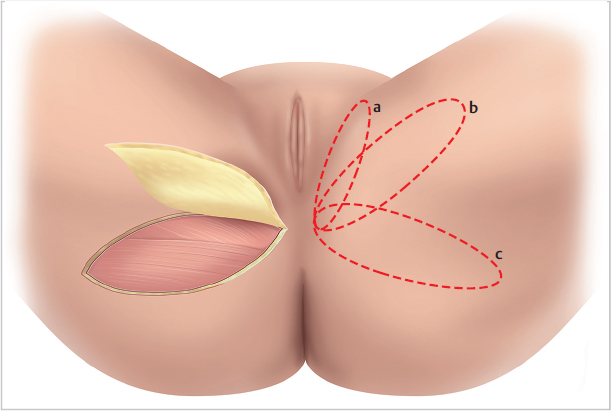
The longitudinal axes of the various possible flaps extend from here along the outer margin of the labia majora (inner lotus petal flap or pudendal thigh flap), the gluteal fold (lower lotus petal flap or gluteal fold flap), which should be drawn on the standing patient preoperatively (▶Fig. 2.27), or in the area between them (intermediate lotus petal flap).
It is best to identify the point of exit of the IPA on the base of the flap preoperatively with Doppler ultrasound. The pedicled adipocutaneous or fasciocutaneous flaps are dissected after incising the margins, beginning at the tip and carrying the incision to the base. It is not absolutely necessary to expose the vascular pedicle at the point of rotation. The angle of rotation can safely be anything up to 90 degrees. Additional incision of the skin and dissection of the subcutaneous tissue at the base of the flap makes it possible to raise a propeller flap. This greatly increases the possible angle of rotation so that the flap can be used to close a vaginal defect.
A base-to-length ratio of 1:3.5 (base width × length) guarantees reliable perfusion. However, the maximum size (length × width) should not exceed 18 × 6 cm.
In addition, the vascular pedicle can be used to create a flap with two lobes (pudendal thigh gluteal fold bilobed flap). Here, the flap design should be chosen such that the closing suture of the anterior portion of the flap lies in the inguinal fold and that of the posterior portion in the gluteal fold. After the dissection, the anterior portion of the flap will lie in the center of the defect to be closed. The posterior portion can be used either to cover a peripheral defect and the anterior donor site defect, or as a V-Y flap (V-Y gluteal fold flap) to provide additional coverage of the defect (▶Table 2.7).
Pudendal Thigh Flap
The pudendal thigh flap lends itself to covering small to medium-sized vertical defects. The flap is based on the terminal branches of the IPA and can be raised with a length-to-width ratio of 3.5:1. The flap has its origin in the junction between the perineum adjacent to the raphe and the proximal medial thigh. The convexity of the adductor magnus forms its posterior margin. The flap can be up to about 6 cm wide and up to 18 cm long. Its axis is defined by extending the line of the groin to the medial thigh.
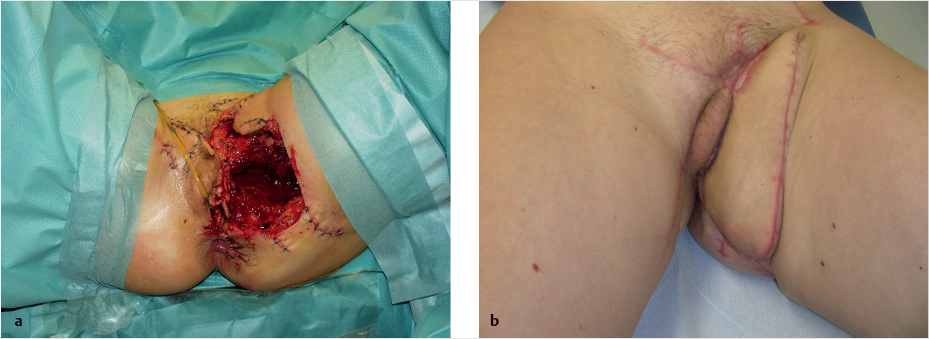
The flap has a certain degree of sensory innervation as the pedicle contains the posterior labial branch of the pudendal nerve and the perineal branches of the posterior femoral cutaneous nerve. The flap is covered with hair. The scar is conveniently located in the inguinal fold so it is not readily noticeable. Following radical vulvectomy, complete reconstruction of the vulva, which includes the vestibule of the vagina and anterior commissure of the labia majora with the frenulum of the clitoris, can be achieved with two bilateral peninsular axial pedicled IPA flaps. One of these two flaps should be about 2 cm larger than the soft-tissue defect in the vulvar region. In this manner, the transposition of the flap creates a 1 cm wide fold which simulates the protrusion of the clitoris in the midline. The flap can also be raised as a simple island flap (▶Fig. 2.28, ▶Fig. 2.29, ▶Fig. 2.30).



Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


