Abstract
This chapter explores surgically applicable anatomical, compositional, and diverse physiologic properties of adipose tissue and their effects on outcomes after body contouring procedures. Adipose is a complex, active endocrine organ. Eighty five percent of all adipose tissue in the human body is subcutaneous, arranged into apical, mantle, and deep layers. The deep layer is found deep to Scarpa’s fascia and is the target layer for liposuction. Adipose tissue is highly vascularized with low oxygen demand and high susceptibility to epinephrine in tumescent fluid. It contains a variety of cell types including a rich store of mesenchymal stem cells, adipocytes arranged into lobules, and supportive connective tissue. Now considered the largest endocrine organ in the body, adipose plays active roles in energy homeostasis, glucose metabolism, immune function, and hormonal regulation. According to the widely accepted “Lipostatic Hypothesis,” the total body number of adipocytes is set during adolescence. Centrally regulated autonomic processes work to maintain a set body weight. If these are overwhelmed by a chronic positive or negative energy balance, adipocytes will change size and eventually volume with resultant metabolic sequelae. Some studies suggest that after lipectomy procedures, the lipostatic mechanism can lead to compensatory fat growth in non-surgically resected areas, both subcutaneous and visceral, beginning 3 months postoperatively. Potential resulting metabolic changes may theoretically affect the patient’s overall health as a result. Finally, understanding the structure and biologic properties of the adipocyte will help guide surgical techniques to improve overall “take” after fat grafting procedures.
2 Clinically Applicable Concepts of Fat Metabolism
2.1 Introduction
While historically we thought that adipose was an inert tissue, capable only of energy storage, this over-simplified understanding is now a thing of the past. After extensive research in recent years, adipose is now regarded as a highly specialized, complex endocrine organ exerting widespread effects in virtually all organ systems. According to the American Society for Aesthetic Plastic Surgery, suction lipectomy has become the most common plastic surgery intervention, with almost 400,000 patients treated in 2015. Increases in this patient population further obligates surgeons of the adipose organ to master an understanding of its biology, which will in turn cultivate a deeper appreciation for liposculptural impact and afford improved results. 1
2.2 Anatomy of Adipose Tissue
2.2.1 Gross Structure
Adipose tissue exists throughout the human body providing the largest volumetric contribution to the connective tissue matrix. Total body fat in lean adults, of which 85% is subcutaneous and the remaining is visceral, contributes approximately 8–18% of total body weight in males and 14–28% in females, and can reach up to 60–70% in obese patients. 2
Markman and Barton were the first to investigate the gross anatomy of subcutaneous fat in a cadaveric study in 1987. Their findings are still commonly accepted and utilized today. 3 There are three discrete layers of subcutaneous fat: apical (or Periadnexal), mantle (or superficial), and deep.
The apical layer is most superficial, located just beneath the reticular dermis, containing yellow-appearing fat and fibrous septa running perpendicular to the skin. Other structures are present including sweat glands, hair follicles, and vascular and lymphatic channels. All these structures are susceptible to damage by the liposuction cannula if this layer is not carefully avoided (▶Fig. 2.1). Traumatic injuries were more common when larger diameter cannulas were used (8–10 mm) with sequelae including seromas, hyperpigmentation, and even skin necrosis. These complications are rare in today’s era of 2–3 mm cannulas. 3 , 4
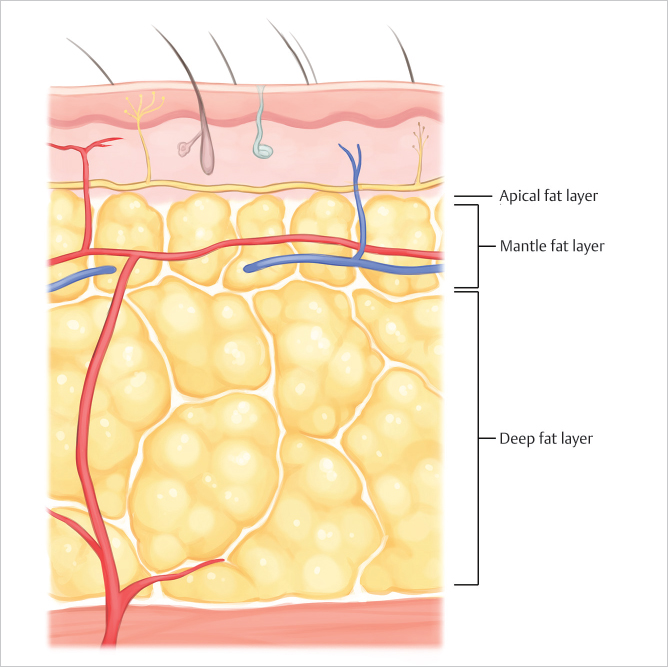
Next is the mantle layer, located everywhere but the eyelids, nail beds, bridge of the nose, and penis, and containing small fat lobules packed tightly with closely-spaced septae. It serves as a shock absorber, helping the skin resist trauma by distributing pressure over a larger field. The thickness of this layer is consistent throughout the body and correlates with the “pinch test”, a depth gauge for the liposuction cannula which should be inserted just beneath this layer. 3 , 4 , 5
Finally, the deep layer, situated just above the underlying muscle fascia, contains large, irregular, poorly organized fat lobules. It is separated from the mantle layer by a continuous fibroelastic membrane, the fascia superficialis (called Scarpa’s, Colles’, or Camper’s fascia in certain anatomic areas). This is target layer for liposuction. Its thickness varies by region based on genetics, diet, and sex, with distinct gender-specific distributions to consider during body contouring procedures. While females display a metabolically-favorable gynoid or peripheral distribution, with increased fat deposition in the gluteofemoral areas, men tend toward a metabolically-unfavorable android or central distribution with increased visceral deposition. 6
2.2.2 Cellular Components and Structure
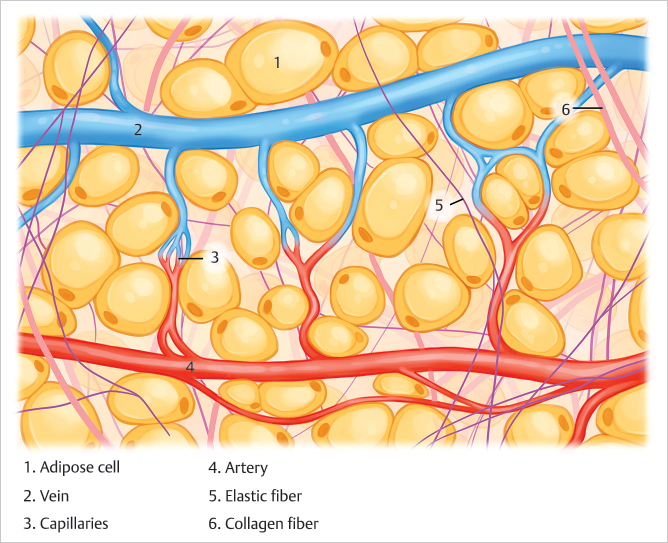
A wide variety of cell types comprise the adipose organ, of which only an estimated 50% are actually adipocytes (▶Fig. 2.2). 2 Other cells that intermingle with the predominant adipocyte, including preadipocytes, endothelial cells, smooth muscle cells, and fibroblasts, are essential to the structure and function of adipose. Stem cells also exist in quantities so rich that adipose is considered their largest known reservoir. 7 Almost every cell type in normal circulation may be present: immune, mesenchymal, vascular, and nervous cells have all been identified in lipoaspirates. 2 , 7
The adipocyte is derived from a connective tissue line of cells resembling fibroblasts. 8 , 9 Mesenchymal stem cells differentiate into spindle-shaped preadipocytes which increase their lipid droplet size, becoming more spherical, to develop into metabolically-active mature adipocytes. 8 , 9 The mature adipocyte consists of a single, large, central lipid droplet surrounded by a peripheral rim of cytoplasm containing a visible nucleus and other organelles, all encased in a thin external membrane. 9
Adipocytes in subcutaneous fat are arranged into lobules supported by septa, a stroma of loose connective tissue, containing a dense capillary network. A high osmotic pressure gradient forces the cells into a tightly packed configuration within the lobule, each supported by a web of collagen fibers known as the extracellular matrix (ECM). The ECM, contiguous with the interlobular septa, connects each cell to the capillary network and also acts as a substrate for cell growth and proliferation. 4 , 7 , 9 This high capillary density, along with low O2 demands, gives adipose has the highest partial oxygen tension of all organs. 10 The characteristic arrangement of adipose (cells compacted within rich microvasculature) and the high sensitivity of these capillaries to epinephrine allows for effective use of tumescent anesthesia and makes office-based liposuction a safe and bloodless operation. 4
2.3 Physiology of Adipose Tissue
2.3.1 Functions of the Adipose Organ
Until recently, scientific belief resigned adipose tissue to the simplistic roles of energy storage, heat insulation, and organ cushioning only. This all changed with the discovery of leptin by Friedman and colleagues in 1994 8 a ground-breaking milestone which sparked an eruption of scientific interest and subsequent knowledge that continues to evolve to this day. Adipose is now considered the largest endocrine organ in the body 11 with known significant roles in lipid transport and synthesis, insulin sensitivity, and regulation of hemostasis, blood pressure, immune function, and angiogenesis. 8
Energy homeostasis is an important function of the adipocyte, which is unique in its ability to store the most amount of calories in lipid form, readily available for rapid release. 8 At times of rest, adipocytes uptake circulating lipids (products of broken down ingested fat) and stored them as triacylglycerol droplets. When high metabolic demands increase sympathetic drive, adipocytes become stimulated via adrenergic receptors. This prompts hydrolysis of stored lipid and release of free fatty acids into the vasculature for use by other organs and tissues. 2 , 6 , 9 Perilipins on the surface of intracellular lipid droplets act as gatekeepers, preventing excessive hydrolysis. In obesity, perilipin concentrations decrease, rendering the adipocyte fragile and prone to free fatty acid release. 12
Adipose also interplays with the endocrine system by releasing two hormones specific to and highly expressed in this tissue. Leptin exerts a direct effect on the hypothalamus, signaling satiety and decreasing food intake. 8 , 13 Homeostatic hormones, such as cytokines, insulin, glucocorticoid, sex hormones, and catecholamines, modulate leptin’s release, thus implicating it in various other roles including glucose metabolism, human development, and blood pressure. 13
Adiponectin is highly involved in the mechanism of insulin resistance by enhancing insulin sensitivity in muscle and the liver. It also promotes free fatty acid oxidation in tissues, thereby decreasing serum lipid concentration. In obesity, adipose maintains a constant inflammatory state, releasing cytokines that modify release of these hormones. Adiponectin decreases while leptin actually increases creating resistance in target cells. These alterations are implicated in the metabolic derangements and disease state associations (including atherosclerosis) associated with obesity. 12
Related posts:
 1 Three-dimensional Imaging for Emerging Technologies in Body Contouring
1 Three-dimensional Imaging for Emerging Technologies in Body Contouring
 6 Noninvasive Radiofrequency Fat Destruction for Body Contouring
6 Noninvasive Radiofrequency Fat Destruction for Body Contouring
 3 Noninvasive Laser Body Contouring
3 Noninvasive Laser Body Contouring
 10 Radiofrequency-Assisted Liposuction for Body Contouring
10 Radiofrequency-Assisted Liposuction for Body Contouring
 19 FaceTite: Procedure Technique
21 High Definition Body Contouring of the Abdomen
19 FaceTite: Procedure Technique
21 High Definition Body Contouring of the Abdomen
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


