17. Ablative Laser Resurfacing
Lasers were originally employed in surgery in the 1960s as a cutting instrument in lieu of a scalpel. They originally used a continuous wave CO2 laser. As technology advanced, high-energy pulsed CO2 lasers were developed that could selectively ablate superficial tissue with minimal residual thermal damage (RTD). This resulted in improvement of many signs of photoaging, scars, and lesions on the skin. Throughout the years, newer laser technologies have been developed to include erbium:yttrium aluminum garnet (Er:YAG) lasers and fractional lasers. The goals of all these devices are to eliminate or reduce sun-damaged collagen and encourage new collagen deposition and remodeling through a combination of tissue vaporization and collagen denaturation.
Equipment
Ablative Carbon Dioxide (CO2) Laser
10,600 nm wavelength
Target chromophore: Water
Absorption coefficient = 800 cm−1
Visible helium-neon laser is projected on the skin to show the targeted treatment area.
Produces tissue vaporization and thermal coagulation 1 – 3
Pulse duration must be <1 millisecond to prevent residual thermal damage (RTD) to surrounding tissue.
5 J/cm1 needed to produce tissue ablation (fluence)
∼20-30 |jm of ablative tissue penetration per J/cm1
Nonlinear relationship between the number of passes and depth of tissue ablation
Decreasing depth of tissue ablation with each additional pass
Limits ablation to ∼200-300 |jm deep 4
Ablation limited but thermal damage is much deeper
70-120 µm area of RTD
Surface temperatures reach 120°-200° C
CO2 ablation
Produces dramatic results but requires a longer healing time because of deeper RTD compared with erbium
Immediate postprocedure edema and erythema resolve in 1-2 weeks and final results require up to 6 months.
High energy pulsed
Energy delivered in 600 microseconds to 1 millisecond
Can produce 500 mJ of energy in <900-microseconds pulse
Uses a spot size of 3 mm or a computer pattern generator (CPG) supplying a pattern of up to 80 pulses with a 2.25 mm spot size
Scanned
Energy delivered in ≤1 millisecond
Scan duration of 0.03–0.52 seconds with a dwell time of 300-1000 microseconds
Computer program scans 0.2 mm spots in a spiral design over an 8-16 mm diameter and performs the ablation.
No one spot is ablated more than once.
Ablative Erbium:Yttrium Aluminum Garnet (Er:YAG)
2940 nm wavelength
Chromophore: Water
Absorption coefficient 10 times greater than that of CO2 laser (12,000 cm−1)
Produces more precise tissue vaporization and less thermal coagulation than CO2 lasers 1
1-3 µm of ablative tissue penetration per J/cm2
5-30 µm area of RTD
Produces 1-50 mJ/cm2 of energy in 300 microseconds to 10 milliseconds
2-7 mm collimated or focused spot size
Value: Comprehensive and versatile. It can be the most superficial laser with quick healing times, or it can be much more aggressive and ablative than CO2 with less RTD and an optimal efficacy safety profile (i.e., can be as aggressive or as superficial as needed).
Three types
Single pulse
Pulse duration of 250-350 microseconds
Variable pulse
Pulse duration of 10-50 milliseconds (longer duration causes more RTD with more secondary collagen deposition); however, the RTD never reaches that of CO2
Dual ablation/coagulation mode (tunable erbium)
Er:YAG ablation 5
Most versatile ablative laser
Can produce superficial wounds from 10 µm that can give quick recovery times and usually require repeat treatments
Can produce the deepest of all wounds because of the extremely high ablation threshold of 5 J/cm2
Excellent results possible with even the deepest rhytids
Less residual thermal damage, so faster healing than with CO2, even for the same depths (5-20 nm residual thermal damage [RTD], compared with 70-120 µm RTD for CO2)
Ablative Fractional Lasers
CO2, Er:YAG, and yttrium scandium gallium garnet (YSGG) models available
Wide variety of models and handpieces provides different fluence and penetration depths.
Produces microthermal zones (MTZ) of ablation injury with surrounding layer of denatured collagen heated to 55°-62° C for optimal long-term collagen deposition/remodeling
MTZ/cm2 can be manually set. (Both depth of injury and density of MTZ can be set.)
Ablation depth up to 1.6 mm (varies based on fluence, wavelength, and spot size)
Settings relate to laser used and desired target (dyschromia, pores, rhytids).
The deeper the ablation depth, the greater zone of coagulation and denatured collagen.
Decreased postprocedure erythema and complications
Complete healing and reepithelialization by 1 week 9
For more aggressive treatments, erythema may last up to 6-8 weeks.
Fractionated lasers
Multiple treatments are needed, because only a fraction of the skin is treated per session.
Open wounds last 3-4 days, with erythema lasting 2-8 weeks for aggressive treatment protocols.
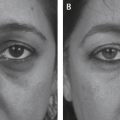
Laser of choice for lower eyelids, acne, and large pore size 5
Technique
Safety (Laser Institute, Occupational Safety)
American National Standards Institute (ANSI) 10 provides policies for laser safety.
Occupational Safety and Health Administration (OSHA) 11 provides oversight.
Proper documentation of safety training is required for all perioperative personnel.
Laser Safety Officer (LSO) provides control over administrative, procedural, and engineering controls.
Each treatment area must define the nominal hazard zone (NHZ), have proper signage for eyewear, and have limited access by trained personnel.
Windows must be covered with appropriate opaque material.
Laser must be test fired before the procedure.
Antiflammable precautions, including saline-soaked clothes, irrigation solution, and fire extinguishers
Smoke evacuation to remove laser plume
Laser kept in standby mode when not actively in use
Markings
Each aesthetic unit to be treated is outlined.
Light blending between aesthetic units provides a smooth transition.
Full-face treatment gives best blend but is not always indicated.
Anesthesia
Ablative lasers cause more pain than nonablative treatments; therefore, when treating areas not easily blocked by local anesthesia, general anesthesia may be indicated for more aggressive settings. Patient preference for comfort is also a consideration.
For very superficial laser resurfacing, topical anesthesia may suffice for limited areas.
Lidocaine cream (LMX) or lidocaine and prilocaine cream (EMLA) 30-90 minutes before procedure
15 g BLT triple anesthetic cream (20% benzocaine, 6% lidocaine, and 4% tetracaine) applied 20 minutes before procedure and again after first laser pass 12
Cold-air cooling
Note:
Use of topical agents should be limited after deepithelialization because of potential lidocaine toxicity. Topical use is limited to one or two areas; lidocaine toxicity is a known issue when large areas are treated.
Local Anesthesia
Central face, including central forehead, cheek, nose, upper and lower lips
1%-2% lidocaine with 1:100,000 or 1:200,000 epinephrine
Lateral face
2% lidocaine with 1:100,000 epinephrine, 0.5% bupivacaine, 1:10 8.4% NaHCO3, and 75 U hyaluronidase
Or, equal parts of 1% lidocaine with 1:100,000 epinephrine and 0.5% marcaine with 1 ml hyaluronidase for every 9 ml local anesthesia
Nerve blocks: 4% articaine hydrochloride
Supraoribital nerve
Supratrochlear nerve
Infraorbital nerve
Maxillary nerve
Mandibular nerve
Mental nerve
Orbital anesthesia
Three drops of 0.5% proparacaine ophthalmic solution to each eye before application of lubricated eye shields
Tumescent local anesthesia
Kessels et al 14 reported using 0.11% solution of 500 ml lactated Ringer solution, 20 ml 1% ropivacaine, 20 ml 2% xylocaine, and 0.5 ml epinephrine
Minimum of 6 ml/kg
Caution:
Tumescent anesthesia introduces water into the tissue which decreases the depth of penetration which may not be desired.
Systemic Analgesia/Anesthesia
1 , 13 (see Chapters 5 through 7)
Oral
10 mg diazepam 30 minutes before procedure
Intramuscular
100 mg meperidine 30 minutes before procedure
25 mg hydroxyzine 30 minutes before procedure
Inhalation
Intravenous 4
Propofol 1-2 mg/kg loading dose, 4–8 mg/kg/hr continuous infusion
Midazolam 0.05–0.1 mg/kg
Fentanyl 50-100 µg
Ketamine 10-20 mg (must administer glycopyrrolate 0.2 mg, propofol, and midazolam first)
Laryngeal mask adaptor (LMA) necessary with heavy sedation
Tip:
Adding NaHCO3 to the local anesthesia to the lateral face neutralizes the pH, whereas the hyaluronidase increases tissue diffusion.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


