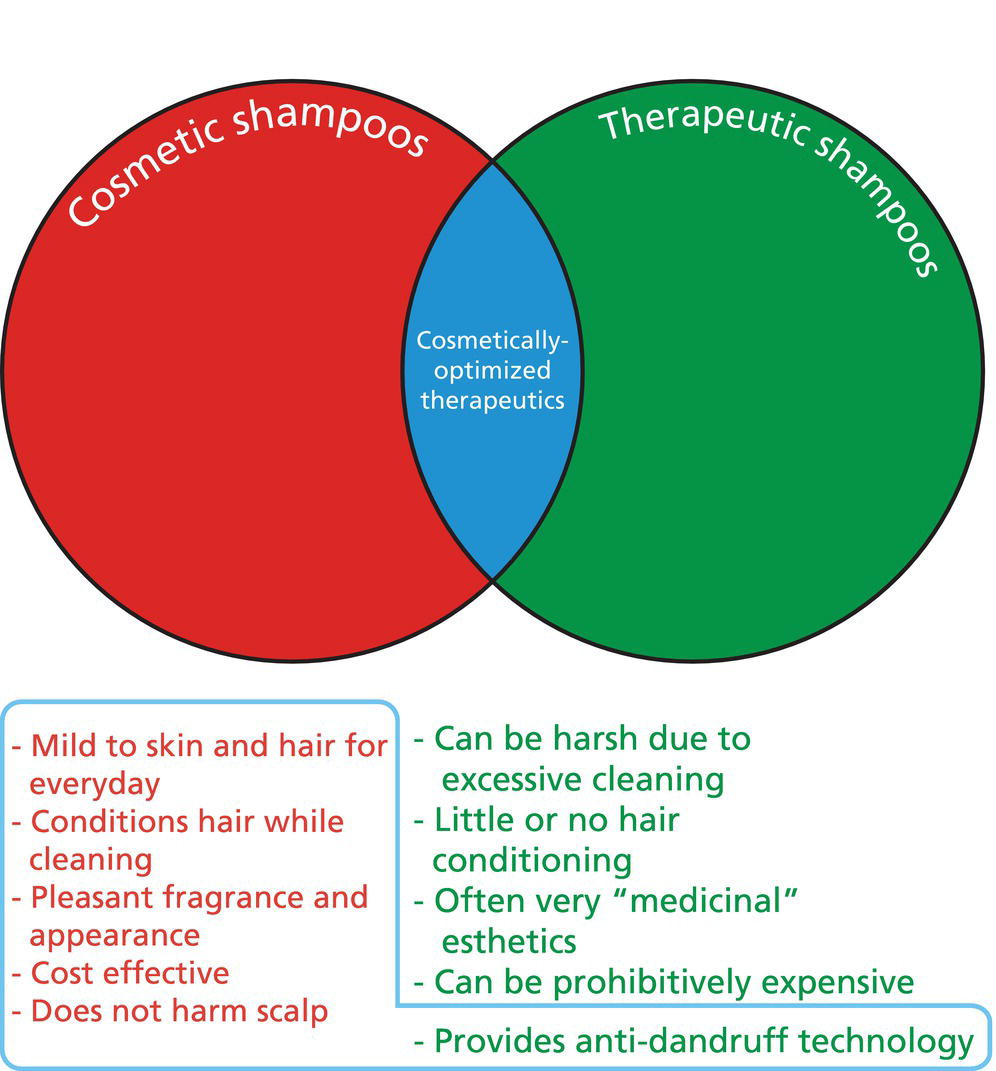
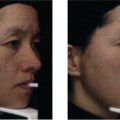
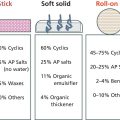
James R. Schwartz1, Eric S. Johnson1, and Thomas L. Dawson2,3 1 Procter & Gamble Beauty Science, Mason, OH, USA 2 Skin Research Institute Singapore (SRIS), Singapore 3 Affiliated Professor, Department of Drug Delivery, College of Pharmacy, Medical University of South Carolina, Mt Pleasant, SC, USA Effective scalp care includes both treatment of conditions such as dandruff and seborrheic dermatitis (D/SD) as well as prevention of these conditions among susceptible individuals. This chapter covers product choice, explanation of benefits and mechanism, and how best to maximize benefits via patient compliance and usage regimens. The scalp is a unique skin environment, combining high sebaceous lipid production with a physical hair covering. The hair physically protects the scalp from UV light, increases the skin surface temperature, and traps moisture vapor; but it can also detrimentally inhibit scalp surface shampoo cleansing efficiency. These conditions favor colonization by the lipid‐dependent commensal fungus, Malassezia. Such colonization is normal as these are commensal species and inhabit all humans [1]. Under certain conditions, Malassezia becomes pathogenic, initiating the inflammation and hyper‐proliferation [2] which lead to the dandruff symptoms [3] of itch and flakes (see Figure 16.1), respectively. Malassezia is still erroneously referred to as “dandruff‐associated, with their role as the cause and their causal mechanism remaining unclear.” However, the vast majority of technically robust literature supports a causal role [4]. Historically, the role of microbes in disease was defined by “Koch’s Postulates,” developed in 1893 [5, 6]: First, a series of experiments in the 1960s and 1970s compare antifungal with antibacterial treatment. In these experiments, dandruff sufferers were treated with a specific antifungal, an antibacterial, and their combination. The antifungal clearly showed that fungal removal decreases dandruff, while removal of bacteria does not. By contrast, removal of both is equivalent to antifungal treatment alone. Reintroduction of a resistant Pityrosporum ovale (likely Malassezia globosa) during antifungal treatment caused dandruff to return [7–9]. Figure 16.1 (a) Image of normal scalp skin. (b) Dandruff scalp image showing adherent white flakes. (c) Seborrheic dermatitis with more evidence of sebum yellowing on flakes and underlying erythema. Collectively, these data support the role of Malassezia as the “cause” of dandruff and fulfill 3 of 4 of Koch’s postulates. Only postulate 1 is not fulfilled, as all humans carry Malassezia as part of their “commensal” microflora. Even Koch himself admitted that postulate 1 could remain unfulfilled, as he observed in asymptomatic cholera carriers [10]. The Koch’s Postulate 1 failure is frequently cited as a confounding factor in defining Malassezia’s role of in dandruff. However, it is accepted that pulmonary aspergillosis is caused by aspergillus, even though it is found in many asymptomatic lungs. The difference is individual susceptibility, a fundamental susceptibility difference between dandruff and nondandruff individuals [11]. This is supported by a study where dandruff and nondandruff individuals were treated with a dandruff‐initiating toxic Malassezia metabolite [12], oleic acid [13]. Oleic acid applied to the scalp induced dandruff‐like flaking in susceptible individuals, while in those who do not get dandruff flaking was not initiated (all subjects had been treated, had Malassezia removed, and their scalp had equivalent minimal flaking). Thus, it is proposed that some, but not all individuals have an inherent “susceptibility” that predisposes them to develop dandruff [13]. The susceptibility remains unknown but many possibilities exist, including skin barrier permeability or a genetic polymorphism such as the CARD‐9 mutation in Crohn’s Disease (which, incidentally, is now shown to be a result of gut Malassezia restricta) [14]. Another important aspect of individual susceptibility is the influence on causality investigation. If individuals have an underlying susceptibility difference, then comparison of affected and unaffected individuals will be of limited value [15]. One cannot assume that the microbiome of unaffected individuals is “benign.” The entire apparatus could be present on “unaffected” individuals – they simply cannot respond regardless of whether the initiator microbe is present [11]. This is very likely the reason studies comparing affected to unaffected remain confusing, and why studies of longitudinal disease cohorts are required [16]. The best‐documented mechanism for Malassezia dandruff pathogenesis is lipase‐mediated release of unsaturated fatty acids onto the scalp [17], but this hypothesis remains somewhat controversial [18]. Malassezia lipases are secreted by the yeast into the surrounding medium to liberate fatty acids from the triglycerides of the sebaceous lipids that are constantly and copiously produced in the hair follicles and excreted onto the scalp surface. Malassezia selectively consumes long‐chain (C16–18) saturated fatty acids to live, the unsaturated fatty acids left behind can then diffuse into the upper layers of the skin and be the initiators of inflammation. Cutaneous inflammation leads to hyper‐proliferation in the epidermis resulting in immature stratum corneum cells with incompletely degraded adhesive function resulting in removal as macroscopic visible clumps – flakes [19]. The resultant condition is called either D/SD, depending on the severity of flaking and the presence of outward manifestations of inflammation (such as redness) [20]. The occurrence of the scalp condition places special requirements on effective scalp care and cleansing; in general, the lower the frequency of scalp cleansing, the greater the chances that scalp conditions such as D/SD will occur [21]. Since the sebaceous lipids are one of the key factors required for formation of D/SD, infrequent removal leads to the build‐up of the pro‐inflammatory by‐products of Malassezia metabolism. Three categories of shampoos can be delineated (Figure 16.2). Cosmetic shampoos are primarily designed to cleanse the hair, but of course, the scalp skin is cleansed simultaneously. Modern versions of these shampoos also condition the hair by depositing certain ingredients on the hair to improve cosmetic benefits such as ease of combing, shine maintenance, and other attributes important to all consumers. Therapeutic scalp care shampoos (often termed “antidandruff”) contain active ingredients to control the D/SD conditions, most often by reducing the Malassezia population on the scalp. Classical therapeutic products tend to focus on the drug active without full consideration of product in‐use esthetics. Cosmetically optimized therapeutic products also contain a drug active to achieve therapeutic benefits, but without the common esthetic trade‐offs (odor, hair conditioning) of therapeutic products. Cosmetically optimized therapeutic shampoos do not necessarily compromise on the magnitude of the therapeutic benefit. Recommendations involving the best products to use must take into consideration patient’s needs for a pleasant user experience and delivery of cosmetic hair benefits. This is because compromises on these attributes significantly reduce patient compliance. No matter how therapeutically effective a product is, benefits will be minimized if usage frequency is compromised. This is a critically important situation in the case of D/SD since the condition is chronic and prophylaxis is the most effective long‐term strategy. Figure 16.2 Representation of the shampoo segments, differentiating cosmetic from therapeutic shampoos and their key attributes. The category of cosmetically optimized therapeutics achieves therapeutic benefits without diminishing esthetic attributes. Table 16.1 Summary of common formulation components of various shampoo types. The primary component (see Table 16.1) of all shampoos is the surfactant system which helps to remove sebaceous lipids, keratin debris, particulates from the environment, and residues from styling products. The surfactants are responsible for the lathering action of a product, the volume and quality of lather are perceived as important signals of cleansing action. Most of the surfactants tend to be negatively charged (anionic), though some contain both positive and negative charges in the same molecule (amphoteric) and others are uncharged (nonionic); these latter types are considered co‐surfactants and function to optimize the lather quality and amount and cleaning ability of the primary anionic surfactant. The surfactant system is optimized to achieve two opposing objectives – cleaning effectively while minimizing irritation of the skin. All surfactants have the potential to irritate the skin to various degrees. The goal of the formulator is to achieve effective cleaning and lathering while minimizing the irritation potential of the product by using the right surfactants. The addition of co‐surfactants can synergistically decrease irritation potential without harming cleaning. Some antidandruff actives also can minimize the irritation potential of surfactants (see below); this is especially important for treatment of the D/SD condition which can be exacerbated by an irritating surfactant system.
CHAPTER 16
Shampoos for Normal Scalp Hygiene and Dandruff
Definition
Introduction

Product and formulation technology overview
Function(s)
Material class(es)
Common examples
Presence in …
Cosmetic shampoo
Cosmetically optimized therapeutic
Standard therapeutic shampoo
Lather/cleaning
Primary surfactants
Sodium lauryl sulfate, sodium laureth sulfate,
Yes
Yes
Yes
Optimization
Co‐surfactants
Cocamidopropyl betaine, cocamide MEA
Yes
Yes
Yes
Hair conditioning agents
Shine, manageability
Silicones
Dimethicone, dimethiconol, amodimethicone
Yes
Yes
De‐tangling, antistatic
Cationic polymers
Polyquaternium‐10, cationic guar derivatives
Yes
Yes
Hydration
Humectants
Glycerin, urea
Some
Some
Hair health
Panthenol and derivatives
Some
Some
Deposition aids
Benefit delivery
Cationic polymers
Polyquaternium‐10, cationic guar derivatives
Yes
Yes
Preservatives
Biocides
Isothiazalinone derivatives, benzoate, and salicylate derivatives
Yes
Yes
Yes
Fragrance
Yes
Yes
Yes
Thickeners
Viscosity
Salts
Sodium chloride
Yes
Yes
Yes
Particles
Glycol distearate
Some
Some
Some
Anti‐dandruff components
Scalp care
Antifungals
Piroctone olamine (PO),
zinc pyrithione (ZPT), selenium sulfide, ketoconazole (see Table 16.2)
Yes
Yes
Potentiators
Zinc carbonate
Some
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


