16 Complications of Blepharoplasty
Abstract
“Complications of Blepharoplasty” addresses this unfortunate reality for all surgeons undertaking such surgery. All surgeons should be familiar with the means of preventing and minimizing the risk of complications, as well as managing them. Complications in the surgical management of patients can arise from errors in preoperative patient evaluation, in diagnosis, in preoperative preparation, in surgical treatment, or in communication. By far the most serious complication of blepharoplasty surgery is blindness. This is usually related to the sudden occurrence of a postoperative orbital hemorrhage, although it can also result from a severe postoperative infection. Others include dry eye syndrome, lower lid retraction, lower lid elevation, lower lid ectropion, epiphora, lagophthalmos, diplopia, blepharoptosis, conjunctival chemosis, corneal abrasion, nerve injury, fat necrosis, infection, rounding of the lateral canthus, hollowing of the eyelids, upper lid skin crease defects, visible scarring, epicanthic folds, bulky upper eyelid, and poor lateral canthal scarring. Cardiac dysrhythmia or bradycardia may also occur during the operation through the oculocardiac reflex, triggered by traction on the extraocular muscles or orbital fat pads. Blepharoplasty surgery is most commonly performed for cosmetic indications. It is of paramount importance not to compromise the function of the eyelids with such surgery.
16.1 Introduction
A thorough preoperative patient assessment and counseling are the first important steps to be taken to minimize risks and potential complications of a blepharoplasty. A number of complications can and do occur after blepharoplasty surgery (Box 16.1). They are an unfortunate reality for all surgeons undertaking such surgery. All surgeons should be familiar with the means of preventing and minimizing the risk of complications, as well as managing them.
Complications in the surgical management of patients can arise from errors in the following:
Preoperative patient evaluation.
Diagnosis.
Preoperative preparation.
Surgical treatment.
Communication.
Box 16.1 Complications of Blepharoplasty
Visual loss
Dry eye or exposure keratopathy
Lower eyelid retraction
Elevation of the lower eyelid
Lower eyelid ectropion
Epiphora
Lagophthalmos
Diplopia
Blepharoptosis
Chemosis
Corneal abrasion
Injury to branches of the facial nerve
Periocular sensory loss
Fat necrosis
Rounding of the lateral canthus
Hollowing of the eyelids
Upper lid skin crease defects
Epicanthic folds
Visible lower lid scarring
Irregular lateral canthal scarring
Oculocardiac reflex
Good communication between the surgeon and the patient, both preoperatively and postoperatively, is essential to patient understanding and cooperation during the management of difficult, untoward problems. Patients who have been counseled very carefully preoperatively and who have been provided with accurate and detailed information are much more willing to accept unfortunate consequences and collaborate with the surgeon to try to rectify the problems. A patient who has suffered a complication of such surgery should be seen early and frequently postoperatively.
Fortunately, serious complications are rare. Most complications are ophthalmic in nature, and for this reason an increasing number of well-informed patients requesting blepharoplasty surgery seek the skills of appropriately trained and experienced oculoplastic surgeons for their surgery.
Many of the complications can be avoided by careful preoperative patient evaluation and selection of the most appropriate surgical procedure for the patient, as outlined in Chapter 15. As a general principle, undercorrections are easier to address than overcorrections.
Key Point
A patient who has suffered a complication of blepharoplasty surgery should be seen early and frequently postoperatively.
16.2 Complications
16.2.1 Visual Loss
By far the most serious complication of blepharoplasty surgery is blindness. This is usually related to the sudden occurrence of a postoperative orbital hemorrhage, although it can also result from a severe postoperative infection with the development of orbital cellulitis and orbital abscess formation.
Blindness after a blepharoplasty is typically believed to be secondary to increased intraorbital pressure resulting in ischemia because of compression of the ciliary arteries supplying the optic nerve, but a retrobulbar hemorrhage can also dramatically increase the intraocular pressure, occluding the central retinal artery.
The precise incidence of a postoperative retrobulbar hemorrhage after blepharoplasty is estimated at 1:2,000, with an incidence of 1:10,000 of permanent visual loss, although this is likely to be an underestimate because this complication is likely to be underreported. Although rare, this is a devastating complication of an operation performed most commonly to improve a patient’s cosmetic appearance.
The patient should be counseled about such a risk preoperatively. It should also be borne in mind that postoperative bleeding can occur even a few days after surgery, and therefore these patients should be advised to restrict their activity after surgery and to avoid traveling away from home for 2 weeks.
The surgery must be performed meticulously with strict attention to intraoperative hemostasis. Undue traction on orbital fat must be avoided. A lower lid blepharoplasty is associated with a higher risk of postoperative bleeding than an upper lid blepharoplasty. Particular care must be taken when debulking the medial fat pads.
It is important to ensure that all risk factors for bleeding are addressed preoperatively. No patient should undergo blepharoplasty surgery involving the removal of orbital fat if hypertension is uncontrolled, if there is a history of a bleeding disorder, or if the patient is taking anticoagulant or antiplatelet drugs.
The patient must be given postoperative instructions about restrictions on activity after surgery. The patient must be able to return to the hospital immediately in the event of any sudden orbital pain, proptosis, or decrease in vision. A patient with a retrobulbar hematoma usually complains of a steady, lancinating pain, similar to that of acute angle closure glaucoma. The patient may also report scintillating scotomas or complete visual loss and may exhibit mydriasis with a relative afferent pupil defect, proptosis with resistance to retropulsion, and hemorrhagic chemosis.
If a patient develops a sudden orbital hemorrhage with proptosis, subconjunctival hemorrhage, and decreased visual acuity, the wound must be opened immediately to drain the hematoma, and a lateral canthotomy and inferior cantholysis should be performed to achieve an emergency orbital decompression (Fig. 16‑1). This can be performed in a clinic setting under local anesthesia so that no undue delay is incurred waiting for the availability of an operating room.

Because the consequences of a retrobulbar hemorrhage are so severe, aggressive intervention is required. If possible, the surgeon should not wait for signs of optic nerve compression to arise (i.e., reduced visual acuity, visual field loss, an afferent pupillary defect), because permanent damage may have occurred by that time. Rather, excessive pain and proptosis necessitate immediate surgical orbital decompression. The incision should be opened and carefully explored.
Medical decompression of the orbit should be organized immediately:
Corticosteroids (intravenous methylprednisolone 100 mg).
Carbonic anhydrase inhibition (intravenous acetazolamide 500 mg).
Osmotic diuresis if necessary (intravenous mannitol 50–100 g infused over 30 minutes).
The patient’s intraocular pressure should be monitored using a Perkin’s tonometer or a Tonopen, and the patient’s fundus should be examined to ensure patency of the central retinal artery has been achieved.
Visual loss from inadvertent globe perforation can and has occurred during the course of a blepharoplasty, but this complication is very rare. It has also occurred after inadequate protection of the globe while using a CO2 laser as an incisional tool. It should not occur when the surgery is undertaken by a suitably trained and experienced oculoplastic surgeon.
Key Point
By far the most serious complication of blepharoplasty surgery is blindness. A discussion about the risk of this must form part of the informed consent process. A surgeon undertaking a blepharoplasty must know how to manage the complication of a retrobulbar hemorrhage.
16.2.2 Dry Eye Syndrome
A postoperative dry eye problem after blepharoplasty surgery is most common in patients who have a preexisting tear film insufficiency and is usually associated with an incomplete reflex blink or frank lagophthalmos. The patient should be carefully examined preoperatively to exclude a dry eye problem. The patient’s tear film and the tear film breakup time should be assessed along with an examination of the tear meniscus, the cornea, and the conjunctiva after the instillation of fluorescein drops. Any blepharitis should be documented and treated. A patient who is found to have any blepharitis, meibomian gland disease, or a dry eye problem must be counseled accordingly. This can be particularly important in patients who have undergone corneal refractive procedures (e.g., LASIK). The consistent continued use of frequent artificial tears is imperative in these patients, who may also require additional procedures at a later date (e.g., punctal plug placement or punctal cautery). Patients who require artificial tears more frequently than three to four times per day should be advised to use a preservative-free preparation (e.g., Xailin gel).
16.2.3 Lower Lid Retraction
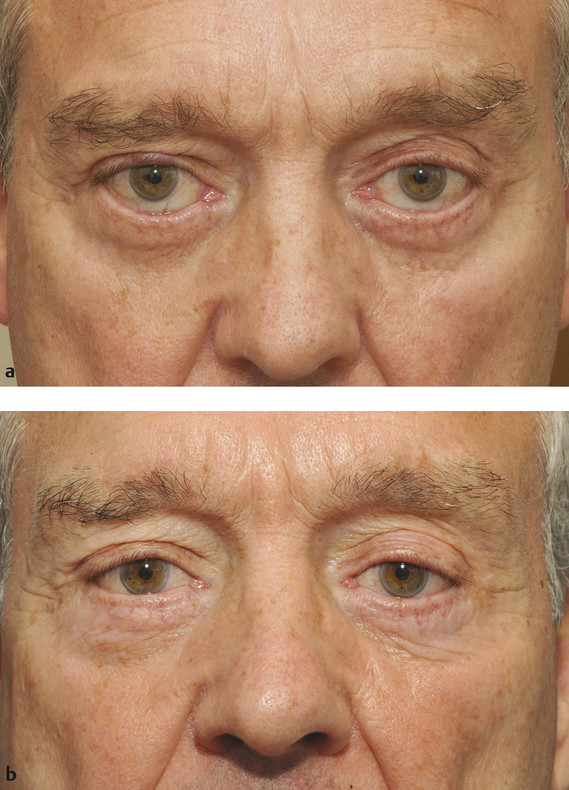
Lower lid retraction and inferior scleral show are well-recognized complications of a transcutaneous lower lid blepharoplasty (Fig. 16‑2). These complications are very rare after a transconjunctival lower lid blepharoplasty.

Lower lid retraction has several causes:
An overresection of skin leaving an anterior lamellar shortage.
Middle lamellar contracture.
The presence of a negative vector with a relative prominence of the globe.
A patient with middle lamellar contracture will have lower lid tethering, and the lid cannot be moved upward digitally over the eye by the examining surgeon. This is in contrast to a patient with lower lid retraction associated with an overresection of skin only.
A mild degree of lower eyelid retraction may be managed conservatively with postoperative vertical eyelid traction and massage. This should be commenced 10 to 14 days after surgery. The patient is instructed to push and hold the lateral two-thirds of the eyelid vertically with the pads of two fingers while looking upward, with the tips of the fingers touching the eyelid margin. After a few minutes, the patient is instructed to apply a lubricant ointment to the skin of the lower eyelid, such as Xailin Night ointment, and to massage the eyelid upward. This regimen should be undertaken for 3 to 4 minutes three to four times a day for 4 to 6 weeks. A mild degree of lower lid retraction can resolve with this treatment.
A greater degree of lower lid retraction resulting from an anterior lamellar deficiency will usually require surgical intervention. The aim is to avoid the use of a skin graft when possible. A suborbicularis oris fat (SOOF) lift or a midfacelift combined with a lateral canthal resuspension or lateral lower lid tightening (a lateral suture canthopexy or a formal lateral tarsal strip procedure, depending on the degree of eyelid and lateral canthal tendon laxity) may prevent the need for a skin graft after an overresection of skin. With these procedures skin is effectively recruited into the lower lid, but only in patients who have an associated midface ptosis. In the absence of a midface ptosis, patients who have a significant vertical skin shortage will require skin grafts combined with a lateral canthal resuspension or lateral lower lid tightening.
Soft tissue expansion can also be considered for selected patients with a vertical skin shortage with no midface ptosis, but such a procedure is associated with a significant interim of disfigurement and a lengthy recovery time.
Middle lamellar contracture requires the division of the scar tissue via a transconjunctival approach with the placement of a posterior lamellar graft (e.g., a hard palate graft or a free tarsoconjunctival graft from the upper eyelid). A dermal graft can also be used, but this will leave a donor site scar. This has the advantage, however, of providing a source of fat pearls for grafting in patients who have also developed lower lid hollowing after an overresection of lower lid fat (see Fig. 16‑2).
A lateral orbital wall decompression undertaken via a lateral upper lid skin crease incision or via a swinging lower lid flap approach, possibly combined with a medial orbital wall decompression undertaken via a transcaruncular approach, is an option for the management of a patient with postblepharoplasty lower lid retraction who has a negative vector, but the patient must be counseled very carefully about the associated risks, particularly the risk of postoperative diplopia (Fig. 16‑3).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


