14. Simultaneous Facelift and Fat Grafting
14.1 The Aging Face and the Need for Fat Injections
Recognizing the changes that occur as the face ages and appreciating the underlying anatomical problems are essential to the recommendation of appropriate treatment and proper planning of surgical procedures. In most patients, problems will fall into three general categories:
Aging and breakdown of the skin surface
Tissue sagging, skin redundancy, and loss of youthful facial contour
Facial hollowing and atrophy
Skin care and skin resurfacing procedures address changes in the first category. Our traditional “lifts” of the face, neck, forehead, and eyes address the second. 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 , 10 , 11 Fat grafting allows us to treat atrophy, 12 something we had previously been unable to do, and is a powerful technique that is now acknowledged by most plastic surgeons and other physicians engaged in treating the aging face as being the most important advance in aesthetic surgery in several decades or more. Properly performed, the addition of fat to areas of the face that have atrophied from age or disease can produce a significant and sustained improvement in appearance unobtainable by other means.
14.2 Why Perform a Facelift and Fat Injections?
Why perform a facelift and fat injections? Why not perform just the facelift? The answer to these questions lies in the multifactorial origin of facial aging mentioned already here and the fact that fat is predictably lost from the face and the face becomes hollow as one ages, in addition to sagging, drooping, and other gravitational effects. The isolated “facelift” procedure, even when aggressively and comprehensively performed, addresses only tissue ptosis and redundancy and often produces a lifted but telltale hollow and under-rejuvenated look. Fat grafting, however, allows the loss of facial fat to be treated simultaneously with the facelift. All things being otherwise equal, simultaneous facelift and fat injections will produce a better result than either technique performed alone, and when a facelift is performed in conjunction with fat injections, both loss of contour and facial atrophy can be corrected, and optimal improvement can be obtained (Fig. 14.1.

14.2.1 Volumetric Rejuvenation, Tissue Integration, and “Stem Cell” Effect
Fat injections have other advantages to the facelift surgeon as well. Fat injections provide for “volumetric rejuvenation,” a new and different means by which to improve facial appearance and a new dimension in which plastic surgeons can work. Unlike nonautologous injectable agents, fat actually integrates with facial tissues and produces an arguably more natural-appearing, sustained, and long-lasting improvement. In addition, fat injections may actually induce an improvement in facial tissue quality through an as yet not clearly defined “stem cell” effect and, performed with a facelift, may constitute, for the first time, rejuvenation in the true sense of the word.
14.2.2 Drawbacks of Fat Injections
Performing fat injections in conjunction with a facelift has certain disadvantages, including the learning curve associated with any new procedure, an increase in operating room time, increased postoperative edema, a longer period of recovery, and uncertainty of graft take. Certain patient misconceptions will also be encountered and will have to be addressed, including misguided beliefs that injected fat can migrate or fall or that fat injections will make the face “look fat.”
14.3 Why Not Just Inject Fat?
Age-related loss of facial fat rarely exists as an isolated event in the healthy patient, and thus patients troubled by it are rarely logically or appropriately treated by fat injections alone. Isolated fat injections are also arguably of questionable benefit to the patient troubled by significant facial sagging and skin redundancy. Although aggressive filling of the sagging face with fat can produce improved contour and a smoother-appearing skin surface, it generally results in an unusually large, overfilled face that appears both unnatural and unfeminine. Such an overfilled face is hard to correct in an attractive manner at a later date, and it is both more logical and more practical to perform fat injections in conjunction with formal surgical lifts, if needed, or sometime after ptotic tissue has been repositioned and redundant tissue has been removed.
14.4 Where Should the Fat Be Injected?
Areas in need of treatment will vary from patient to patient, and planning fat injections requires looking at the face in a different way, more as a “sculptor” and less as a “tailor,” as we have done in the past. Any area successfully treatable with nonautologous injectable fillers is potentially treatable with fat injections, including, but not limited to, the temple, brow, radix, upper orbit (upper eyelid), lower orbit (lower eyelid), cheek, midface, lip, perioral, nasolabial crease, geniomandibular groove, jawline, and chin areas. Experience with fillers is a useful point of reference for planning fat additions to the face. Perhaps the best way to decide where fat is needed is for the surgeon to study his or her facelift outcomes carefully and identify areas where the procedure has fallen short. In most cases, the greatest shortcoming for the experienced surgeon will be evident as the failure to replenish lost volume, and the areas in need of treatment will be obvious. In time, and after engaging thoughtfully in such study, one will gain a deeper appreciation of facial atrophy and an increasing desire to correct it. Fig. 14.2 shows a patient before and after facelift and fat injections and the areas where fat was placed.

14.4.1 Sequencing Fat Injections with Other Procedures
Although there is no consensus on when fat grafting is best performed during facelift surgery, as a practical matter, it is most expedient to inject fat at the beginning of the procedure before the facelift itself has been performed. The reasons for this include that it is easier to harvest the fat at the beginning of the procedure before the face has been prepared or draped and when the patient is typically in a deeper plane of anesthesia. Also, in the beginning of the procedure, the tissue planes of the face have not been opened, the face is not swollen, and preoperatively made pen marks and facial landmarks are easier to identify. In addition, surgical principles suggest that it is best to limit the time the graft is out of the body.
14.5 Fat Injection Technique
The basic technique for fat grafting has been described previously, 13 and the principles set forth by Coleman and Mazzola 14 are observed when fat grafting is performed.
14.5.1 Logistics of Simultaneous Facelift and Fat Injections
Fat grafting is often mistakenly thought of as a simple procedure that can be performed in a few minutes. This is rarely the case, however, and such an attitude will lead to frustration, disruption of workflow, and poor outcomes. For the procedure to be successful, fat must be harvested in a specific time-consuming manner, and it must then be processed and infiltrated in a technically demanding and time-consuming process. Fat grafting is also an artistically demanding activity that will require a considerable amount of the surgeon’s creative energy. When anything other than a few small areas of the face is being treated, the entire procedure can easily encompass an hour or longer, something that can overburden a surgical team already engaged in a long and demanding facelift operation consisting of multiple procedures. Time must therefore be planned appropriately.
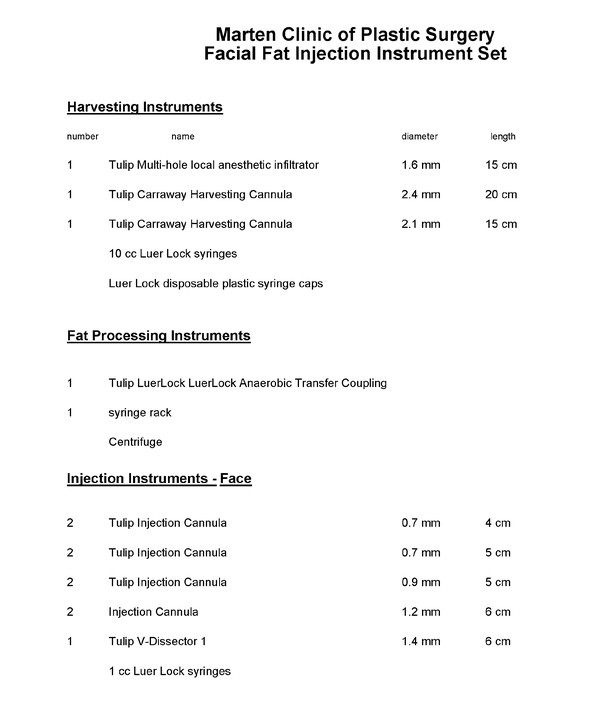
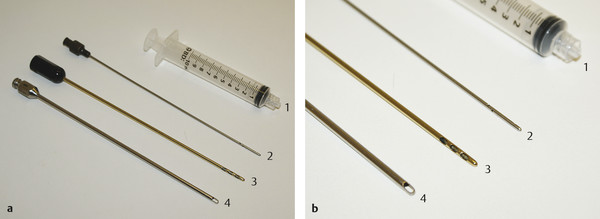
14.5.2 Needed Equipment
Special instruments are required for harvest and injection (Fig. 14.3, Fig. 14.4, Fig. 14.6, Fig. 14.7, Fig. 14.9, and Fig. 14.10), in addition to a few other pieces of equipment to process and organize the fat. If sharp hypodermic needles are used to inject fat (other than indradermally), fat embolization and serious related problems, including tissue infarction and visual impairment and blindness, can occur, and therefore their use is not recommended. Special blunt-tipped cannulas are required to safely perform fat grafting; poor outcomes are likely if sharp hypodermic needles are used. Sharp-needle injection also poses a serious risk of fat embolization and related problems.

14.5.3 Choosing a Fat Harvest Site
Currently, there is no scientific consensus as to where the “best” sites to harvest fat from are for fat grafting procedures. Harvest sites are typically chosen and marked in conjunction with the patient in such a manner as to improve his or her silhouette, although the ideal locations are arguably those areas of diet- and exercise-resistant fat collections. For women, this is typically the hip, outer thigh, and abdomen areas, and for men, it is the “love handle” and “spare tire” areas.
In thin patients, small harvests from multiple areas are typically required, including the inner thighs, inner knees, upper buttocks, and anterior axilla, and this will add more time to the procedure. It is recommended that the harvest sites and site markings be photographed preoperatively to document what was agreed on and to avoid any dispute over the preoperative condition of harvest sites after surgery.
14.5.4 Preoperative Marking of the Face
Fat grafting cannot be performed arbitrarily, and a careful plan must be marked preoperatively, with the patient in an upright position. Marking will require concentration on the surgeon’s part and is best carried out in a private area that is free from distractions. Creating an initial plan on a life-sized laser print of a photograph of the patient’s face is helpful in organizing one’s thoughts and facilitates discussions with the patient as to which areas will be treated. In most cases, marks are made in conjunction with the patient while he or she holds a hand mirror. Once markings are complete, additional photographs of the marked face are taken and printed for use during the procedure.
14.5.5 Anesthesia
Most modern facelifts are time-consuming and technically demanding, and the addition of fat injections to the procedure will test the patience and composure of almost any surgeon. It is highly recommended that one enlist the services of an anesthesiologist or competent certified registered nurse anesthetist when combined procedures are performed.
Most of our facelifts are now performed with the patient under deep sedation administered by an anesthesiologist using a laryngeal mask airway, which allows the patient to be heavily sedated without compromise of the airway, but the patient need not receive muscle relaxants and can be allowed to breathe spontaneously. The heavily sedated patient is also easier to harvest fat from, especially when fat must be harvested from multiple sites. Comprehensive treatment of the face with fat is facilitated under these conditions.
14.5.6 Harvesting Fat
Fat is harvested the day it is needed and is not frozen and stored. Fat should be harvested in a thoughtful and artistic manner that improves the patient’s figure; thus, it must generally be removed bilaterally and in a symmetrical fashion.
It is prudent to examine the thin patient at the time of consultation because thin patients with limited fat stores often present significant challenges when harvesting fat, and extra time and effort will be required to obtain fat from them. Anesthesia and operating room times, as well as the surgeon’s fee, must be calculated accordingly.
Fat is harvested after anesthesia is initiated but before preparation of the face. In all but the unusual case, a complete preparation of the torso is not necessary. Typically, a limited preparation of the marked area is made, and a sterile field is established about the prepared area. If fat is to be harvested from the hip or lateral thigh, the patient is turned into a semilateral decubitus position, prepared, and draped, and harvesting is performed. Then the patient is turned to the opposite side, where the harvest procedure is repeated. If the patient is positioned carefully, this position can be used to harvest fat simultaneously from multiple additional sites, including the upper buttocks, inner thighs, and knees (Fig. 14.5).

Areas from which fat is to be harvested are infiltrated with 0.1% lidocaine with 1:1,000,000 epinephrine solution using a multiholed local anesthetic infiltration cannula (Fig. 14.6); adequate time must be allowed for a proper anesthetic and hemostatic effect. Approximately 1 mL of dilute local anesthetic solution is injected for every 3 mL of anticipated fat removal. It is not necessary or desirable to infiltrate in a “tumescent” fashion, as overwetting the harvest site will result in an overdilute harvest and more time being spent in the harvesting process. Local anesthetic should be injected even if general anesthetic is used.
Fat is then harvested with a special harvesting cannula (Fig. 14.6 attached to a 10-mL syringe using gently applied syringe suction to avoid vacuum barotrauma to the tissue. Sharp hypodermic needles should not be used. In general, at least twice as much fat is harvested as is anticipated will be used; this is to ensure that an adequate supply of processed fat will be available for use on the face.
Once fat harvest is complete, the stab incision used to obtain the fat is closed with a simple interrupted suture of 6–0 nylon. The harvest site is then washed free of preparative solution, and the sutured site is dressed with a Tegaderm dressing (Nexcare, St. Paul, MN).
Processing Harvested Fat
Harvested fat is generally not uniform in character as extracted; some type of processing is therefore necessary to obtain uniform material for injection. Although fat can be separated simply from the oil and water fractions using a ”tea strainer”–type sieve or rolling it on Telfa gauze, most of the “stem cells,” “growth factors,” and “cellular messengers” are likely lost when this is done. Centrifugation, on the other hand, is believed to allow separation of the “oil” and “water” fractions from the fat cells while simultaneously concentrating these other potentially important components.
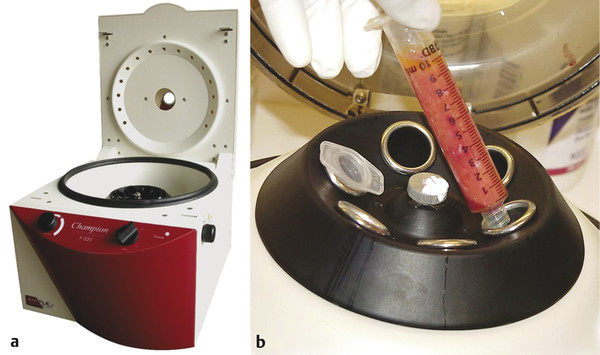
Before centrifugation is begun, a sterile Luer lock cap is placed on the end of the syringe to keep its contents inside it, and the syringe plunger is removed from the syringe barrel. Capped syringe barrels containing unprocessed fat are then loaded into the centrifuge rotor in a balanced fashion and spun for 1 to 3 minutes. Most centrifuges available for this purpose have rotors that can be sterilized so that the syringes the fat is in remain sterile and can be handled by the scrubbed surgical team. Other centrifuges have sterilizable tubes that fit into the rotor for this purpose (Fig. 14.7).
Harvested fat is generally not uniform in character as extracted from donor sites; each syringe will contain a variable amount of fat, blood, local anesthetic, and ruptured fat cells (“oil”); some type of processing is necessary to obtain uniform material for injection. Centrifugation allows separation of the “oil” and “water” fractions from the fat cells and concentrates high-density adipocytes (“stem cells”). Once centrifuged, syringe barrels containing spun fat are removed and will contain upper oil, central fat, and lower “water” components ( Fig. 14.8).
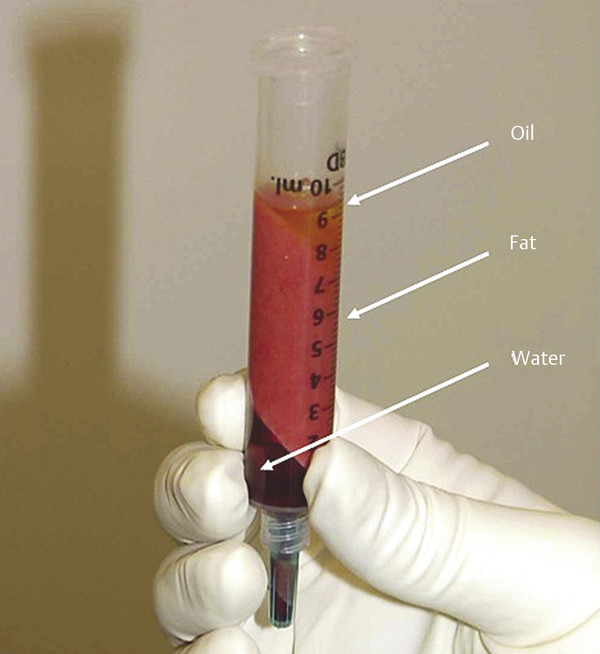
Three layers of harvested fat can be seen in the centrifuged material: an upper “oil” layer (ruptured fat cells), a middle layer of intact fat cells, and a bottom layer of blood and local anesthetic. Unlike straining of fat through a sieve, centrifugation is believed to allow separation of the “oil” and “water” fractions from the fat cells with minimal loss of “stem cells,” “growth factors,” and “cellular messengers.”
The typically blood-tinged water (local anesthetic) component is separated by simply removing the syringe tip cap and allowing it to run out. The oil fraction is then poured off out of the top of the syringe. Telfa sponges can also be placed inside the syringe barrel to “wick up” the small amount of residual oil present after most has been poured off. A “test tube”–type rack to hold the syringes containing fat greatly facilitates fat processing activities (Fig. 14.9).

A “test tube” rack to hold the syringes containing fat greatly facilitates fat-processing activities. On the left, the syringes containing unprocessed fat are present. In the center, syringes containing centrifuged fat can be seen. The rack also conveniently holds 1-mL syringes, syringe components, other equipment used in the fat grafting procedure.
14.5.7 Injecting Fat
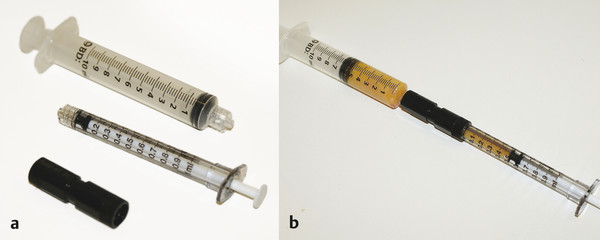
After centrifugation and discarding the oil and water fractions, the fat is transferred into 1-mL Luer lok syringes using a transfer coupling (Fig. 14.10), as proper infiltration of fat requires injection in very small aliquots that cannot be reliably made with a 10-mL, 5-mL, or even 3-mL syringe. The bottom 2 mL of fat in the syringe contains the highest concentrations of high-density adipocytes (or adipose-derived regenerative cells) and is used preferentially in the procedure and for critical areas (orbits, lips, and tear troughs). If an overharvest is made, enough high-density fat will be obtained that the whole facial fat grafting procedure can be performed with it.
Nerve blocks are then performed with 0.25% bupivacaine with epinephrine 1:200,000 local anesthetic solution and an adequate time allowed for a proper anesthetic and hemostatic effect. It is typically not necessary to directly infiltrate areas to be treated with local anesthetic in the facelift patient if nerve blocks are performed correctly and sedation has been administered.
Once nerve blocks have been administered, 0.7-mm, 0.9-mm, and 1.2-mm cannulas are used to infiltrate fat into the face through small stab incisions in the facial skin. These incisions can be made with a no. 11 blade scalpel or a 20-gauge needle and are so small that they will not require suturing at the end of the procedure.
Infiltration is made in multiple passes in planes appropriate for the area being treated, injecting on both the in and out strokes, usually from two separate injection sites, while feathering into adjacent areas. Injecting from at least two separate injection sites allows “crisscrossing” of cannula passes during graft placement and smoother fat infiltration and helps avert a “row of corn” effect that might result if injection was made from only one site.
14.5.8 How Much Should Be Injected? Is It Necessary to Overcorrect?
Deciding on how much fat needs to be injected at a given site requires empirical information, and one cannot simply rely on what one sees in the operating room. In general, there is a tendency to treat most areas too conservatively if amounts are decided by intuition alone, and some overcorrection is needed, as not all the graft will survive. It is also the case that more fat will be needed than one would use to fill a similar defect with nonautologous filler. In most cases, the amount needed can be decided preoperatively based on what is seen in the preoperative photos; as a practical matter, there is an empirical range and a “small,” “medium,” and “large” treatment within that range applicable to each site.
14.5.9 How Is the Fat Injected?
As the cannula is advanced, tissue resistance is felt for; if resistance is felt, a small injection is made. Approximately 0.5 mL or less should be injected per pass. This corresponds to 20 to 40 back-and-forth passes or more for each 1-mL syringe of processed fat. If tissue resistance is not felt as the injection cannula is advanced, a pass and injection have likely already been made in that area, injection is not made, and the cannula is directed to another area. The goal is to inject the fat in a way that optimizes its chance of developing a blood supply and surviving, and the mental model should be one of scattering tiny particles of fat into the recipient site in multiple crisscrossing fine trails in such a way that each particle sets in its own compartment and has maximal surface contact with perfused tissue. If fat is injected in a bolus, fat cells will be clumped together, and only those on the periphery of the injected area will have tissue contact and will be likely to survive. Most of the more centrally situated fat particles will have contact only with each other, will be less likely to survive, and can lead to the formation of oil cysts.
Advancement and withdrawal of the injection cannula will typically be made slowly by the beginning injector, but as familiarity with the technique is acquired, the movements can and should be made faster. Ultimately, all other things being equal, faster movements are desirable in that if the injection cannula is constantly in motion, intravascular injection is less likely, and the likelihood that an accidental bolus injection into one area will be made is reduced. Rapid back-and-forth movements ensure the smoothest and most uniform infiltration of fat.
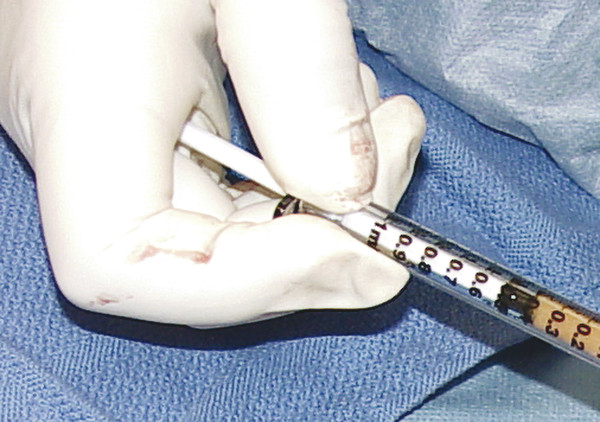
How the syringe is held is also important in avoiding overinjection and controlling the volume injected with each pass. If the syringe is held in the manner one would traditionally use to give an injection, with the thumb on the end of the syringe plunger, it is easy to inject too much fat if tissue or injection cannula resistance suddenly decreases. Generally, more control can be maintained, and overinjection can more easily be avoided, if the syringe is held with the end of the plunger in the palm of the hand (Fig. 14.11). With the syringe held in this manner, a slight closing of the hand results in only a small amount of fat being expressed from the cannula, and overinjection of any one area can more readily be avoided.
Although cannula obstruction will be very uncommon if fat is harvested and processed as described, if a cannula becomes blocked, additional injection pressure should not be applied, as this is the most common cause of a sudden and unintentional bolus injection. It is better in such circumstances simply to withdraw the blocked cannula, pass it to the surgical assistant, and continue with a different one. The assistant can then clear the obstruction while the surgeon continues to work with the second cannula. Typically, the cause of the obstruction will be a particle of fat at the interface of the cannula and the cannula hub that is most easily cleared by removing the cannula from the syringe and extracting the fat partical from inside the back of the hub with a fine forceps.
14.5.10 How Deep Should the Fat Be Injected, and in What Layers Should Fat Be Placed?
Fat grafts will necessarily be placed in different planes, depending on the areas being treated and the problem present. In many areas where multiple tissue layers exist in which to inject and overlying skin is thick, injection can be made comprehensively at the treated site from the periosteum to the subdermal layer. These areas typically include the geniomandibular groove (GMG), piriform, midface, cheek, and chin. In other areas, injections must necessarily be placed more specifically because of the anatomical characteristics of the treated sites if optimal results are to be obtained and irregularities are to be avoided. These areas include the temples, which are injected subcutaneously; the upper orbit; the lower orbit; the “tear trough,” which should be injected in a preperiosteal/suborbicularis occuli plane; the lips, which should be injected predominantly in a submucosal plane; and the jawline, which should be injected in a preperiosteal/submasseteric plane. The easiest areas for the beginning injector to treat are the sites in the former category. In the beginning, it is wise to “stay deep” and place most of the graft in a predominantly preperiosteal plane. Once familiarity with the technique has been obtained, areas in the latter category can then cautiously be treated.
Geniomandibular (“Prejowl”) Groove
Grafting of the prejowl–geniomandibular groove area with fat has a high aesthetic payoff and is a good area for the beginning injector to gain experience with the technique (Fig. 14.12). Although not immediately and intuitively obvious, filling the GMG creates a strong, uninterrupted aesthetic line from the chin to the posterior mandible that cannot be achieved by lifting the jowl alone and results in a highly desirable improvement on both the male and female face. The effect is similar to that of the placement of a Mittleman prejowl implant, but the filler fat is autologous and the filling procedure is arguably simpler to perform. Fat grafting of the prejowl–GMG area is performed with a 4-cm-long, 0.7-mm cannula, and fat is placed in all tissue layers between the periosteum and skin. Typically, 1 to 3 mL of fat is placed on each side. Level of difficulty: beginner.


Related posts:
 6. Facial Sculpting and Facial Slimming with Neurotoxins
6. Facial Sculpting and Facial Slimming with Neurotoxins
 20. Comparison of Midface Rejuvenation Techniques
20. Comparison of Midface Rejuvenation Techniques
 22. Lower Eyelid Blepharoplasty
22. Lower Eyelid Blepharoplasty
 23. Lateral Canthal Complications in Aesthetic Eyelid Surgery: Prevention and Reconstruction
23. Lateral Canthal Complications in Aesthetic Eyelid Surgery: Prevention and Reconstruction
 5. Energy-Based Treatments for Facial Aging
5. Energy-Based Treatments for Facial Aging
 12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


