14 Halfway to a Body Lift

Abstract
Abdominoplasty techniques have evolved over the past 2 decades such that the abdominoplasty procedure and its derivatives represent a cornerstone of aesthetic contouring of the trunk and lower extremities. This evolution has incorporated the concepts of selective undermining of abdominal soft tissues, which maximizes the blood supply of the abdominal flap, maintaining low scar position aesthetics and placing maximal tension at the line of wound closure laterally between the lateral pubic hair region and the mid-axillary line with anchoring of the flap to the superficial fascial system. These concepts were largely introduced and refined by Lockwood.1 Our procedure of abdominoplasty entails lipocontouring of the posterior hips and flanks in more than 95% of patients undergoing abdominoplasty to achieve a true “circumferential” contouring of the trunk. The addition of skin excision in the area of the posterior hips, including the subcutaneous adipose layer down to and through the superficial fascial system (SFS), has been performed to enhance the contouring of the hip areas. Closure of the SFS achieves a modest lateral upper thigh lift without undermining the thigh tissues further, enhancing the contouring of the lateral hip and thigh area. The incision extends to, and sometimes beyond, the posterior axillary line. This has led me to describe this procedure as “halfway to a body lift.” This procedure is particularly beneficial in the post–massive weight loss patient, who typically presents with exaggerated deformities of the lateral and posterior trunk.
Introduction
Modern abdominoplasty techniques were developed in the 1960s.2,3 Over the ensuing 30 years, modifications were introduced,4,5 but the cardinal features and surgical principles of the technique remained the same. These founding principles of the technique included a transverse lower abdominal incision; wide undermining of the abdominal skin flap often to the costal margins; tightening of the abdominal muscle girdle by means of plication sutures and resection of the excess lower abdominal skin with inferior advancement of the abdominal flap; and, finally, closure, with maximal tension at the line of skin closure occurring in the midline of the abdominal flap.5
While accepting this as the standard method of performing “full abdominoplasty,” often the long-term results were suboptimal due to overtightening of the central aspect of the abdomen with accompanying superior displacement of the pubic tissues and depressed or spread scar appearance. In addition, there was often laxity of the lateral lower abdominal tissues. These shortcomings were cited by several authors who assessed the results that were noted in the 1980s from a long-term perspective.6,7
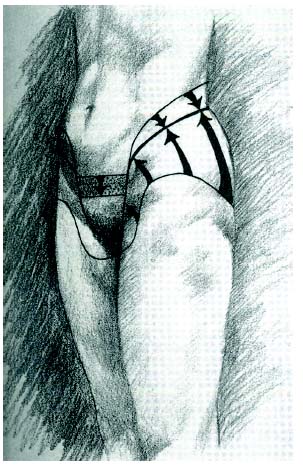
A paradigm shift in the thinking about abdominoplasty was effected by Lockwood,1 when he introduced and refined the concept of high lateral tension abdominoplasty. His insight was that the main deformity in the aging abdomen results from truncal laxity that occurred laterally in most patients, and that this was not addressed by standard abdominoplasty approaches. In addition, he recognized the need for circumferential contouring of the trunk to achieve significant aesthetic contouring and advocated liposuction of the abdomen and posterior trunk as essential elements of the procedure. He devised a procedure that entailed selective undermining of the abdominal flap, which allowed the safe application of liposuction to the flap along with an aggressive excision of tissue in the lateral lower abdomen, along with a wound closure that incorporated the superficial fascial system (SFS) ( Fig. 14.1 ) to achieve lifting of the upper thigh tissues.8 These concepts were immediately recognized as valid by surgeons around the world and were widely adopted. In addition, they gave rise to even more aggressive approaches to body contouring in the form of body-lift procedures.9,10
From a conceptual standpoint, a full abdominoplasty entails an elliptical or lenticular excision of skin and subcutaneous tissue, with more tissue still being excised centrally than laterally, thus producing some degree of lateral excess or a “dog-ear.” Very frequently, this dog-ear must be excised at the end of the procedure by extending the incision posteriorly. Depending on the preoperative deformity and the selected incision plan, this additional excision can be somewhat lengthy and, in my hands, has frequently required a patient position adjustment from the supine to a modified oblique position during the latter stages of the procedure. Furthermore, my experience has taught me that there was often more of a subcutaneous adipose tissue component to this excess than a skin component that was not completely addressed by the liposuction of the posterior hip and flank regions (done in more than 95% of these patients). Indeed, the size or amount of this tissue excess or dog-ear depends on the amount of skin and adipose tissue excess and the soft tissue laxity that the particular patient presents with preoperatively ( Fig. 14.2 ) in the lateral aspect of the trunk between the anterior and posterior axillary lines, and is independent of the technique used for closure of the lateral wound.
I began to see and treat more patients who had significant tissue excess of adipose and skin tissue in the posterior hip and flank areas that did not extend to the midline posteriorly, but nevertheless required a posterior extension of the incision and tissue resection. It became apparent that many such patients would achieve far greater contour enhancement in the hip and flank region by direct excision of skin and underlying adipose tissue after the liposuction in this area has been completed. Sometimes this excision extends to and beyond the posterior axillary line, but never to the midline of the back itself.
Because extending the dissection posteriorly at the end of the procedure is tedious and frustrating due to patient repositioning with drape modifications, I recognized that it could much more easily be done with the patient in the prone position, which is my preferred approach for the posterior trunk lipocontouring at the beginning of the procedure. Therefore, I began to perform this excision with the patient in the prone position ( Fig. 14.3 ) at the outset of the surgical operation, immediately after completing the liposuction of the posterior hips, flanks, and mid- and lower back, as deemed necessary during the preoperative planning. Following excision of the skin and subcutaneous adipose tissue, closure of the SFS begins posteriorly and proceeds in a lateral direction. This SFS tightening produces a modest lateral thigh lift without discontinuous undermining in the thigh area.
As I began to analyze the postoperative results in these patients ( Fig. 14.4 ), I noted that the scar appearance was analogous to half of the posterior scar that is seen with a body lift in many patients. I therefore began to refer to this procedure as “halfway to a body lift” because it incorporates many of the technical aspects seen with that operation. It has consistently produced the additional benefit of excellent contour improvement in the lateral hip region that I have not been able to produce with a more standard abdominoplasty and lateral hip liposuction alone. I believe it has application in many patients seeking body contouring who do not require a circumferential approach but who present with skin laxity and soft tissue excess in this area of the trunk.


Related posts:
 12 Combination Abdominal Wall Hernia Repair and Mid-Body Contouring
12 Combination Abdominal Wall Hernia Repair and Mid-Body Contouring
 11 Lower Body Lift Combined with Liposuction and Gluteal Flap Surgery
11 Lower Body Lift Combined with Liposuction and Gluteal Flap Surgery
 16 Complications and Management Following Mid-Body Sculpting
16 Complications and Management Following Mid-Body Sculpting
 10 Circumferential Abdominoplasty
10 Circumferential Abdominoplasty
 15 Lipoabdominoplasty with Progressive Tension Sutures
15 Lipoabdominoplasty with Progressive Tension Sutures
 13 Circumferential Dermolipectomy of the Lower Trunk: Lower Body Fit
13 Circumferential Dermolipectomy of the Lower Trunk: Lower Body Fit
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


