13. Submental Contouring
13.1 Introduction
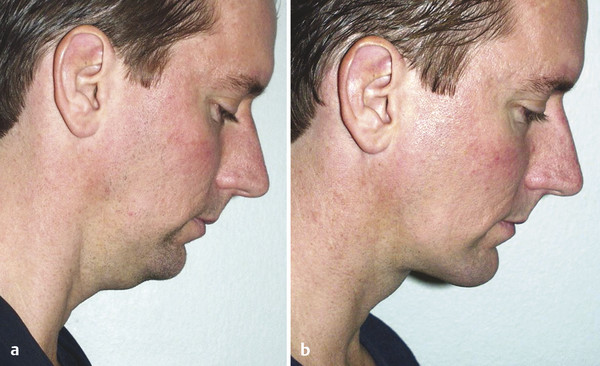
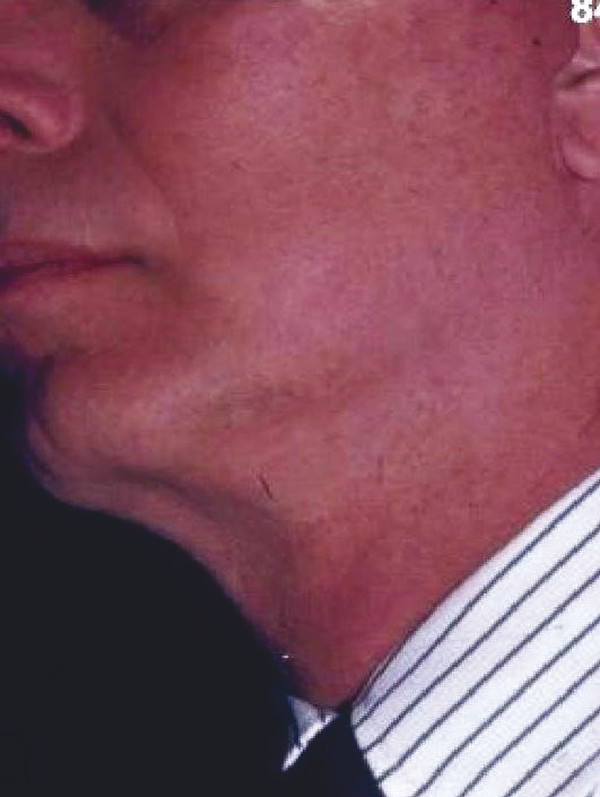
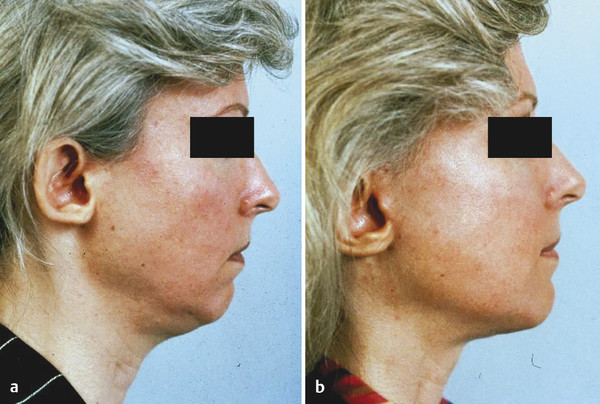
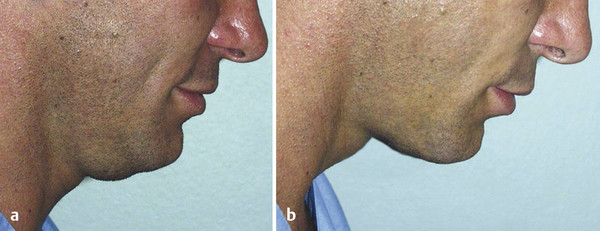
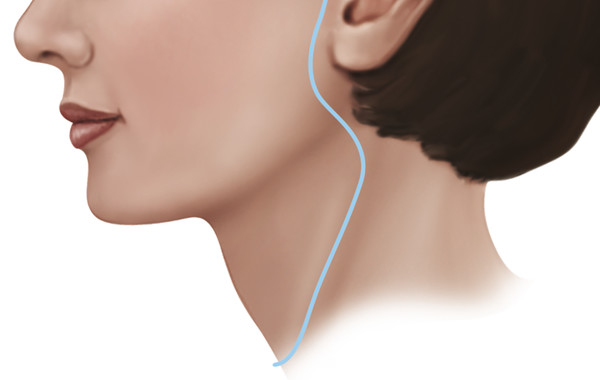
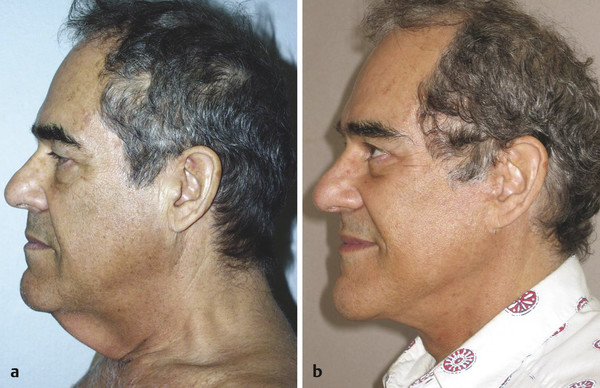
A well-contoured neck is an artistic necessity for an attractive and pleasing appearance. 1 The neck can indicate fitness or obesity, vitality, strength, sensuality, beauty or elegance, masculinity or femininity, health or disease, and age. Correction of the submental bulge produced by either submental fat or digastric muscle hypertrophy corrects the appearance of obesity and produces the appearance of fitness (Fig. 13.1). A well-defined jawline with a normal contour to the submental area results in the appearance of both beauty and sensuality (Fig. 13.2). Correction of the submental area with improvement of the witch’s chin along with a facelift can change an old appearance to one of youth and elegance (Fig. 13.3). It is not enough to perform a limited liposuction and tighten skin. Correction of the deep-layer problem and providing support can produce restoration of the contour of this area that was present 20 years ago (Fig. 13.4).



The most commonly encountered submental neck anatomical problems are excessive skin, contractile neck skin (or “nipple skin”), platysma laxity, subcutaneous or subplatysmal fat, enlarged submandibular glands, or digastric muscle hypertrophy. (See the following list.) Long-term improvement in the neck contour cannot be achieved simply by tightening the neck skin over these problems.
13.1.1 Common Anatomical Problems in the Submental Area
Excessive skin
Contractile neck skin (“nipple skin”)
Platysma laxity
Excess subcutaneous fat
Excess subplatysmal fat
Digastric muscle hypertrophy
Enlarged submandibular glands
13.2 Management of Digastric Muscles
Contour problems can be caused by large anterior bellies of the digastric muscles at rest or by decreasing the projection of the chin by looking downward or with surgical correction of prognathism, which may cause a double chin. Prominent digastric muscles may be exposed after a facelift in which fat has been removed (Fig. 13.5). Digastric muscle hypertrophy is corrected by performing a tangential resection of the anterior belly of the digastric. 2
On examination of the neck, enlarged digastric muscles may appear as a sausage shape under the skin anterior to the submandibular gland, and they become larger when the neck is flexed. When the chin is extended, the digastric muscle is placed under tension and made narrow, and the submental bulge is improved. Extension of the chin will not improve the appearance of the submental region when the bulge is due only to subplatysmal fat. Digastric muscle hypertrophy may be hidden by submental fat (Fig. 13.6and Fig. 13.7).
The technique of tangential excision of the anterior belly is relatively straightforward and is performed through the submental incision. After the submental incision has been made and the anterior neck has been dissected, a line is drawn in the submental area in the sagittal midline. To verify that the line is appropriately placed, it can be compared with the dental midline. The platysma muscle is then grasped using Allis clamps on each side of the line. The platysma muscle (or fascia in cases where the platysma does not come completely to the midline) is then opened in the midline using scissors. The edge of the platysma muscle on one side is then grasped with two Allis clamps. Cautery is then used to dissect underneath the platysma muscle.
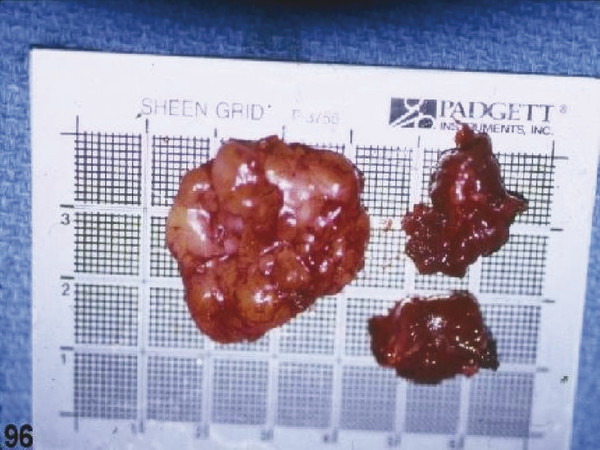
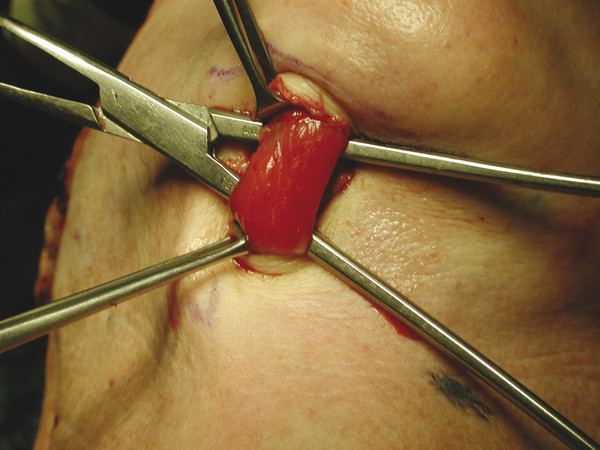
After the plane has been opened up underneath the platysma muscle, the subplatysmal fat can be removed in a graded fashion to improve the submental contour. Next the digastric muscles can be addressed. The digastric muscles are visible laterally. A tonsil clamp can be passed through the anterior digastric muscle (Fig. 13.8). Electrocautery can then be used to tangentially excise the anterior belly of the digastric muscle. Typically, 90 to 95% of the anterior belly of the digastric muscle is excised (Fig. 13.9). A clinical example showing the improvement in the neck after treatment of the digastric muscles is shown in Fig. 13.10.
13.3 Treatment Options for the Neck
Multiple options are available for treatment of the neck (submental area; see list to follow). The first option is using submental liposuction alone. A neck lift using a submental incision alone can be performed for more significant problems. The neck lift may be combined with a chin implant. A neck lift may also be performed without a skin excision, in which case the occipital incision is used for access only, and no skin is excised. An isolated neck lift may also be performed with skin excision. Finally, the neck lift may be combined with a facelift. The neck lift allows the precious subcutaneous fat to be preserved and allows problems of deep-layer origin to be appropriately treated. The following are treatment options available for the neck:
Submental liposuction
Neck lift (submental incision only)
Neck lift with chin implant
Neck lift without skin excision
Neck lift with skin excision
Neck lift with facelift
Submental liposuction is an incomplete solution for most patients. The problem is that the practitioners using this technique have assumed that the patient’s poor neck contour is the result of accumulation of subcutaneous fat only. Liposuction alone of the neck will result in some improvement in the appearance of the neck, but it will not offer complete correction. I have seen many cases in which submental liposuction created significant deformities and the patient actually looked older and worse after the procedure. The aggressive use of submental liposuction may remove all the fat between the digastric muscles and create hollowness centrally in the submental area with platysmal banding. As mentioned previously, the removal of cervical fat may unmask hypertrophied anterior belly of digastric muscles. Deflation of the submental area may also result in sagging and deflated submental skin, even with the use of newer technologies such as laser liposuction.
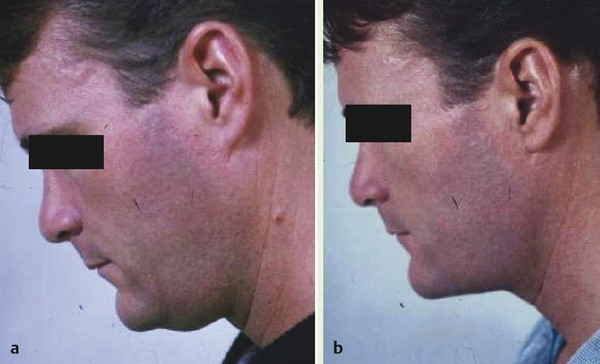
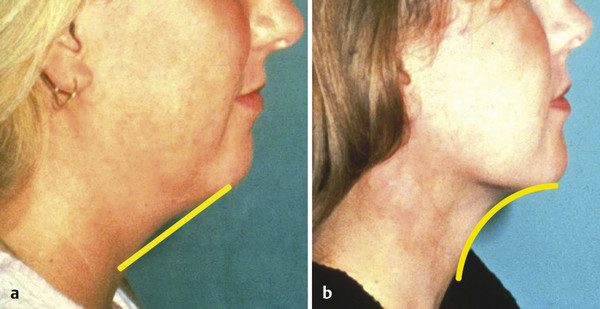
It is possible to improve the appearance of the neck without skin excision because a straight-line anterior neck can become a curved concave line with the use of excessive neck skin. A straight line between two points is shorter than a curved line. The excessive neck skin is then used to make the curved neckline concavities (Fig. 13.11). Patients who are typical candidates for this approach are younger and have good skin tone. They have isolated submental problems with excess subcutaneous and subplatysmal fat and also may have hypertrophied digastric muscles. Clinical examples of this approach are demonstrated in Fig. 13.12. After the procedure, the submental wound is dressed with Steri-Strip. No pressure dressing is necessary to establish the submental hollow. Another clinical example of this approach is shown in Fig. 13.13 and Fig. 13.14; this patient objected to his double chin, which was noticed when he looked downward. The surgical procedure involved removal of subplatysmal fat along with a 95% tangential resection of the anterior belly of digastric muscles via only a submental incision.


The combination of a chin implant and a neck lift can improve the appearance of the neck (Fig. 13.15). Chin implants can improve outcomes but by themselves cannot improve neck contour. The anterior projection of the chin can be improved using a chin implant, but a chin implant cannot put tension on the submental tissues and will not improve submental contour.

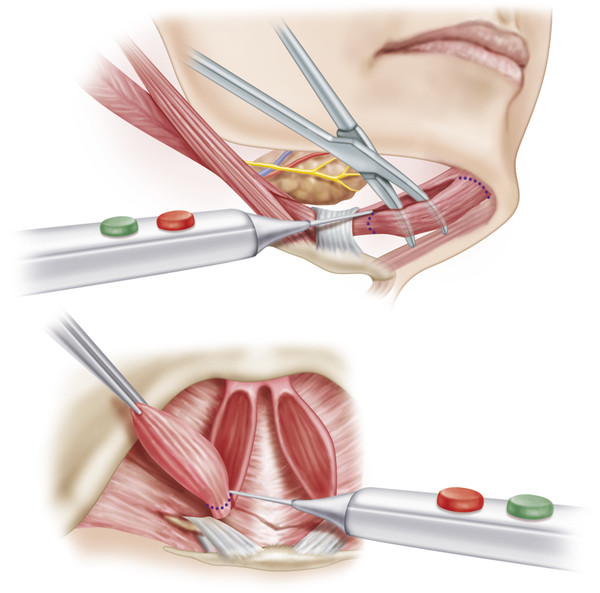
In some cases, a neck lift is performed using both a submental incision and a postauricular incision that goes into the occipital hairline without excision of any skin. This procedure is used in younger patients who have neck problems resulting from tightness of the platysma. The occipital incisions are used for access so that the platysma can be transected. The course of this transection is 0.5 cm anterior to the anterior border of the sternocleidomastoid muscle. The division is continued transversely across the platysma at or below the level of the cricoid cartilage (Fig. 13.16). Division of the tight platysma along with other maneuvers such as defatting of the neck and treatment of digastric muscle hypertrophy can markedly improve the cervical contour with a more refined jawline and submental area (Fig. 13.17). When no skin is to be excised, the occipital incision can be made into the occipital hair because there is no possibility of transposing non-hair-bearing skin into the occipital area.

Sometimes it may be unnatural to lift and improve the neck while not improving the cheeks, jawline, and brow. When the neck lift is performed along with a facelift, a more balanced and natural rejuvenation is obtained. In many cases, a significant amount of redundant skin must be excised to allow for maximal improvement in the appearance of the neck (Fig. 13.18). In these cases, the neck lift needs to be combined with a facelift using periauricular incisions to achieve maximal improvement in the neck. In these cases, the occipital hairline incision must be placed along the occipital hairline to prevent transposition of non-hair-bearing skin into the occipital scalp.
Two submental procedures that we do not use have been popularized by other surgeons. The first is excision of submental skin, which is an error in surgical judgment. The excess skin in the submental area is needed to fill in the concave contours that have been created with the submental manipulations and should not be discarded. The second procedure that we never perform is the submental Z-plasty. 3 The scars resulting from this procedure are in a poor location and are easily detected; quite simply, much better methods can be used to improve the appearance of the neck (Fig. 13.19).

13.3.1 Placement of the Submental Incision
Appropriate placement of the submental incision is critical to achieving quality aesthetic results with the neck lift. The submental crease accentuates a witch’s-chin appearance and is immobile. Placement of the submental incision in this location will deepen the crease and create a double-bubble appearance in the submental area instead of creating a smooth submental contour. A better location for the incision is 1 to 1.5 cm posterior to the submental crease and is centered on the dental midline. The incision is normally about 3 cm wide (Fig. 13.20). By incising the skin posterior to the crease and undermining the crease anteriorly, the native submental crease can be broken up, and the skin in the submental area will redrape more evenly. The incision is also mobile and allows for efficient treatment of deep contour problems (Fig. 13.21). It is important to have men grow out their beard for 2 days before the neck lift. The orientation of the hair follicles, in the beard is then easily detected, and the incision can be made precisely parallel to the hair follicles, thus minimizing scar visibility.


From the submental incision, the chin may be undermined so that the skin can redrape more evenly if a facelift is added to the procedure. In the process of undermining the chin, the native submental crease is released. The mandibular ligaments that help to form the jowl can also be released by dissecting superiorly and laterally through the submental incision.
Related posts:
 6. Facial Sculpting and Facial Slimming with Neurotoxins
6. Facial Sculpting and Facial Slimming with Neurotoxins
 20. Comparison of Midface Rejuvenation Techniques
20. Comparison of Midface Rejuvenation Techniques
 22. Lower Eyelid Blepharoplasty
22. Lower Eyelid Blepharoplasty
 23. Lateral Canthal Complications in Aesthetic Eyelid Surgery: Prevention and Reconstruction
23. Lateral Canthal Complications in Aesthetic Eyelid Surgery: Prevention and Reconstruction
 5. Energy-Based Treatments for Facial Aging
5. Energy-Based Treatments for Facial Aging
 12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


