12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
12.1 Introduction
As patients have started to live longer and longer, there has been an increasing use of cosmetic procedures to help patients look as young as they are feeling. A vast number of tools are now available to surgeons to help patients look more youthful. The use of botulinum toxin can help to soften dynamic lines. Even with paralysis of the muscles causing the wrinkles, there can be lines in the skin, essentially fold flaws that have developed after years of muscle activity. The use of various fillers can help these depressions in the skin and also replace volume in areas where there has been facial atrophy. Chemical peels and lasers may defer surgical treatments for some time, but ultimately, if patients want to be restored to a more youthful appearance, they will need surgery.
A properly performed facelift and neck lift procedure can essentially treat all the elements involved in facial aging. To address the volume loss seen with aging, fat grafting performed at the same time as the facelift can restore volume. Proper use of the superficial musculoaponeurotic system (SMAS) will provide for resuspension of the facial fat to its more youthful locations and improve the sagging and laxity seen with aging. Finally, tightening the skin with tailoring of the excess skin will improve skin tone and remove many of the rhytids.
Although many proposed facelift techniques are available to surgeons, we have used the high-SMAS facelift as the procedure of choice for rejuvenation of the aging face.
12.2 Need for the SMAS
There is no question that the use of the SMAS has improved the quality of the results in facelifts. Traditional facelift techniques have focused on the elevation of facial skin flaps with subsequent redraping and excision of redundant skin under tension. Skin is a tissue that serves to provide a protective barrier from the outside world. It is a very elastic tissue capable of stretching significantly, as can be seen in the example of the abdomen of a pregnant woman or even more dramatically in patients who are morbidly obese. Because the skin is such an elastic tissue, there are many common problems that are seen with skin-only facelift procedures.
The use of skin to lift the whole of the tissues of the face requires a significant amount of tension to be placed on the skin. This tension causes a flattening of the structures of the face and results in the “windblown” tight and drawn appearance to the face that is unfortunately associated with facelift procedures. The tension causes other problems as well, including poor wound healing with wide scars, skin necrosis, and traction on the earlobes with resulting displaced or pixie ears, retraction of the tragus, and distortion of the temporal hairline, sideburn, and occipital hairline.
Biomechanical studies have demonstrated that both skin and the SMAS demonstrate stress relaxation and creep; however, the SMAS has been shown to have significantly less stress relaxation and creep than skin. 1 The implication of this observation is that the SMAS is much better suited as a foundation that can be used to reposition the facial fat and restore a youthful appearance compared with the skin.
In addition to providing superior aesthetic results, the use of the SMAS also provides for an increased longevity to the facelift. In the first study to evaluate the longevity of a facelift procedure, Sundine et al 2 reviewed a carefully followed series of 42 patients who had their primary and secondary facelifts performed by the senior author. The average length of time from the primary facelift to the secondary facelift was 11.9 years. There were some early failures, defined by the authors as a secondary procedure before 5 years. Most of the failures were due to inelastic skin caused by sun damage or medications (corticosteroids or protease inhibitors). Another group of patients who are at risk for early recurrence of their facial laxity are patient who have had significant weight loss and also have reduced elasticity of their skin.
Another important advantage to the high-SMAS facelift is that it can provide for a harmonious rejuvenation of the midface, and the use of the SMAS can be customized to each patient’s individual needs. For further review of the various procedures available for midface rejuvenation, see Chapter 20.
The combination procedure includes appropriate release of the ligaments restraining the SMAS and use of the SMAS to resuspend the facial fat and restore the softness over the malar areas and reposition the jowls back up into the cheeks while flattening the nasolabial folds. 3 Dissection of the SMAS with release of the parotidomasseteric ligaments with a superoposterior positioning of the flap provides support to the submental area. The use of a preauricular flap of the SMAS that is transposed to the mastoid area provides support to the hyoid area and serves to define the cervicomental angle.
The use of a large SMAS flap that has been shifted posteriorly and superiorly has multiple effects that improve the regeneration of the face. By maintaining the anterior platysma cutaneous ligaments, the traction on the face will serve to support the tissues of the cheek and help to create an attractive submalar hollowing. This flap also helps to elevate the downturned corners of the mouth and marionette lines that frequently accompany facial aging. This approach to the aging mouth provides a more natural elevation to the corners of the mouth compared with procedures that excise triangles of skin above the oral commissures. 4 In contrast to previous reports 5 that use of the SMAS deepens the nasolabial crease, we have shown that using the SMAS clearly delivers improvement in the upper and lower nasolabial fold areas and does not deepen the nasolabial crease. 3 In patients with a heavy upper nasolabial fold, the addition of a third flap from the superior portion of the SMAS that is transposed up to the temple will give added support and help to flatten the upper aspect of the nasolabial fold.
The use of the high-SMAS configuration in the facelift also significantly improves the periorbital area. With transection of the SMAS at the superior border of the zygomatic arch and suspension of the flap superiorly and posteriorly, the nasojugal fold is transposed from the oblique direction seen in the aging face to run transversely along the inferior orbital rim, imparting a more youthful appearance. This same effect can also be achieved with a third flap from the superior portion of the SMAS flap transposed to the temporal area.
By virtue of the SMAS flap design, the high-SMAS flap will transect some of the lower fibers of the orbicularis oculus muscle. When this flap is transposed posteriorly and superiorly, there is pressure across the inferior aspect of the orbital septum reducing bulging of the orbital fat compartments. Patients can expect approximately 40% improvement in the appearance of their lower eyelids after the high-SMAS facelift.
12.3 Preparing for Surgery
All patients are asked to obtain preoperative medical clearance by their primary care physician before the procedure. Appropriate laboratory studies, including a complete blood count, coagulation studies, electrolytes, and an electrocardiogram, are obtained. Patients are given a list of products that may cause problems with bleeding, including products that contain aspirin, ibuprofen, and naproxen. Many patients are also taking herbal supplements and vitamin combinations that may cause bleeding problems. They are asked to stop all these products for 3 weeks before their surgical procedure. Patients may take acetaminophen for any discomfort they have before the procedure.
Patients who are smokers are asked to stop smoking for 4 weeks before the procedure. It should be assumed that smokers will not stop smoking for the procedure. Patients who are smokers are at a high risk for significant complications, including skin-flap necrosis, poor wound healing, and thromboembolic phenomena. Nevertheless, we do not cancel surgery in smokers, but the tissues must be handled very carefully (e.g., not folding over the skin or SMAS flaps to prevent ischemia to the flaps) to minimize the risk of skin necrosis.
Patients may have their hair tinted up to 2 weeks before their surgery and may tint it again 4 weeks after the surgery. There can be difficulties with hair loss if these instructions are not followed. Male patients are asked to grow out their beard for 2 days before the surgery. Analyzing beard growth helps in planning incisions and also is an aid in making the incisions parallel to the hair follicles.
Patients are told not to get tanned or sunburned for 2 weeks before the surgery. All patients are given a bottle of povidone-iodine soap and are asked to wash using this soap along the planned incision lines for 2 days before the surgery.
12.3.1 Marking
The procedure begins with marking the patient in the preoperative holding area. Marks are placed at the medial, central, and lateral brow relative to the orbital rim. The appropriate new position for the brow is marked with the brow elevated to a pleasing aesthetic position. The distances are compared with the results of the preoperative worksheet. Transverse forehead rhytids and glabellar creases are then marked. A circular mark is placed around the head of the corrugator superciliaris muscle, which will be partially removed or transected. The medial eyebrow is elevated, and the patient is asked to close his or her eyes. This maneuver will reveal the depressor superciliaris muscles as a vertical band, and a vertical line is marked on the medial and lateral aspects of the band. Transverse marks delineating the creases from procerus muscle activity in the nasofrontal angle area are then marked. The incision for the browlift procedure is then marked.
Attention is next directed to the markings for the facelift component of the procedure. A small circle is drawn at the malar pivot point, which would correspond to the peak projection of a malar implant. It is located over the body of the zygoma by dropping a vertical line inferiorly from the lateral limbus. The circle is then located about 1.5 cm below the inferior orbital rim.
The patient is then asked to close his or her eyes gently, and the crow’s feet creases are then marked. The lateral eyebrow is held elevated, and the patient is asked to smile. If a prominent band running from the lateral aspect of the eyebrow along the lateral orbital rim develops, this band is marked. This section of the orbicularis oculus muscle has been designated as the depressor orbicularis lateralis by Connell (personal communication, 2002). When this muscle is active, it is important to divide the muscle in an inferior oblique direction approximating a crow’s-feet crease, or the muscle will continue to pull down the lateral brow and defeat the effort of the browlift to raise the lateral brow.
The lines for the SMAS elevation are then marked. The superior and transverse line is marked from the center of the malar pivot point extending posteriorly along the superior edge of the zygomatic arch to a point about 1 cm from the ear. The inferior limb of the SMAS elevation is then marked about 1 cm in front of the ear extending down in the neck along the anterior border of the sternocleidomastoid (SCM) muscle. A determination is made at the time of the consultation as to whether the platysma muscle will need to be transected. If the platysma muscle is to be transected, this is done at or below the level of the cricoid cartilage to prevent a transverse line of demarcation in the neck.
Next, the mandibular ligaments are marked on the chin. The site for the ligaments is easily identified by mobilizing the cheek medially and inferiorly to accentuate the jowl. The mandibular ligaments are located just anterior to the jowl and marionette lines in the chin. The site for the submental incision (if necessary) is then marked. This incision is centered on the dental midline of the mandible and is located 1 to 1.5 cm posterior to the native submental crease. The incision is normally about 3 cm wide. The jowl area is elevated with the surgeon’s hands upward and laterally to ensure that the submental incision will not be visible on the face. An incision placed into the submental crease would result in an even deeper crease postoperatively. By incising the skin posterior to the crease and undermining the crease anteriorly, the crease can be broken up and the skin in the submental area will redrape more evenly.
The position of the cricoid cartilage in the neck is now marked, and the position of the external jugular veins is also marked to prevent injury to the veins with the dissection. The facelift markings are demonstrated in Fig. 12.1.

12.3.2 Planning the Temporal Incision
To achieve natural and harmonious results, it is absolutely critical that two elements be achieved with the facelift. The obvious element is achieving an effective lift and tightening of the tissues. The other element, which is just as important, is planning the incisions such that they are well hidden and no stigmata of the patient having had a facelift, such as widened scars, obvious scars, and displacements of the hairline or sideburns, are seen. There has been much recent interest in “short-scar” facelifts. 6 It should be emphasized that the scar should be only as long as necessary to accomplish an effective rejuvenation. The scars associated with the short-scar facelifts are not much shorter than those seen with more effective techniques, and the short-scar techniques are much less effective at providing optimal rejuvenation.
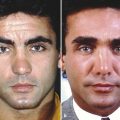
The temporal portion of the facelift has been traditionally designed to go into the temporal hair above the ear. The rationale for this incision is that the resulting scar will be hidden in the hair, and the scar will be less conspicuous. This incision is useful in cases where there is little skin laxity in the temple area and upper cheek and there is little risk of displacing the hairline significantly. Patients who are candidates for this incision are typically younger; however, when there is significant laxity in the temple skin and upper cheek and the incision is placed into the temporal hair, the temporal hair-bearing scalp will be discarded as the skin is tailored, resulting in the loss of the sideburn area along with a widened distance from the lateral canthus to the temporal hairline, which appears unnatural, is unattractive, and is a telltale sign of a poorly designed and executed facelift (Fig. 12.2). These patients are rendered “hairline cripples” and are not able to wear their hair pulled back or up because the hairline distortion is clearly exhibited with such hairstyles. Patients who are active and cannot keep their hair combed over the distorted hairline are also significantly bothered by this deformity.

The distance from the lateral canthus to the temporal hairline is 4.5 cm or less in youthful-appearing people (Fig. 12.3 a). Assessment of the laxity of the skin in the temple and upper cheek area must be made preoperatively using skin pinches. The combination of the information from the measurements and the skin pinches determines the appropriate site for the temporal incision.
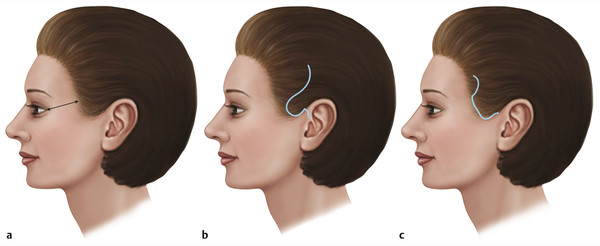
In patients with little laxity of the skin in the temple and upper cheek, the temporal incision can be designed to course into the temporal hair. When this option is chosen, it is important to design an anterior projection of hair-bearing skin on the posterior aspect of the temporal flap just above the ear (Fig. 12.3 b). The purpose of this flap is to prevent the transposition of non-hair-bearing scalp superiorly into the temporal hair. This deformity has been attributed to widening of the scar, but it is actually an error in planning the incision. This incision can be continued superiorly to join with the incision for a coronal browlift as needed.
When the determination is made that the distance from the lateral canthus to the temporal hairline will be greater than 5 cm or if there will be significant elevation of the sideburn, the choice should be made for temporal hairline incision (Fig. 12.3 c). The temporal hairline incision is able to accommodate the large posterior and superior skin shifts necessary to obtain optimal correction of the upper and lateral face without creating distortions of the hairline or sideburn. In patients with significant laxity of skin in the temporal and upper cheek area, an incision into the temporal hair will result in a posterior and superior displacement of the hairline, which results in a strange and “operated” appearance. Some patients do not have a significant amount of laxity in the temple and upper cheek area but have a naturally elevated sideburn area. These patients will not tolerate even the slightest posterior and superior displacement of the sideburn area and will also require the temporal incision to be made along the temporal hairline (Fig. 12.4). A final group of patients who are frequently candidates for the hairline incision at the temporal hairline are secondary facelift candidates who have already had the sideburn and temporal hairline displaced posteriorly with the primary procedure. At the superior aspect of the incision, an anteriorly based U-shaped extension of the incision is made posteriorly into the hairline to allow for taking out the dog-ear without distorting the hairline.

Many surgeons object to use of the hairline incision based on the belief that the scars will widen and become very visible. It is critical when performing the temporal hairline incision to adhere to these important surgical principles. When the incision is made, the bevel of the scalpel blade should be absolutely parallel to the hair follicles. The skin needs to be tailored so that there is no tension on the skin to prevent widening of the scar, and the skin should be sutured using half-buried mattress sutures with the knots tied in the hair to prevent any visible suture marks. When these principles are followed, a fine-line scar results, which is a much better trade-off compared with a distorted and displaced hairline from an incision into the temporal hair.
It is very important to discuss with the patient the placement of the temporal incision. This is framed as a choice between two imperfect alternatives. When a patient is shown in the mirror what the distorted hairline will look like if the incision is made within the temporal hair, there is usually no objection to the hairline scar. In the early healing period, when the scars are somewhat red, female patients may feather some makeup over the incision to conceal the scars.
12.3.3 Planning Incisions around the Ears
The incisions around the ears are frequently a telltale sign for those looking to see whether a patient has had a facelift performed. In the past, the incision in the preauricular area was typically a straight vertical incision starting anterior to the helix that continued inferiorly in front of the tragus to the earlobe. The incision can be used in patients who have skin that is a similar color and texture in the cheek and on the tragus, but this situation rarely occurs. In the vast majority of patients, there is a gradient of color change as well as texture change that occurs from the tragus going anteriorly to the cheek. The skin of the tragus has a more fair complexion, and more anteriorly the skin becomes redder. In these patients, when a preauricular skin incision is made for the facelift, the reddish cheek skin is now juxtaposed next to white preauricular skin. Even with perfect wound healing, there is an obvious mismatch of skin color, indicating that the patient has had a facelift performed. When the incision is placed along the margin of the tragus, there is no obvious color change noted anterior to the ear, and the scar is essentially invisible.
Marking the preauricular incisions begins at the junction of the helical rim with the head. The incision should be marked to continue the visual curve of the helical rim down into the notch between the crus of the helix and the tragus. This incision results in a naturally-appearing curve that defines the helical rim. The incision should not follow the anterior edge of the cartilage of the helical rim because the resulting scar will be too anterior and will make the skin of the helix appear wide.
A slight anterior traction should then be placed on the skin anterior to the tragus. The markings for the incision should be placed along the margin of the tragus. At the inferior aspect of the tragus, in the intertragic notch, the markings should then turn 90 degrees anteriorly. The markings continue anteriorly until the crease that runs anteriorly to the earlobe is reached. When the crease is reached, the incision turns 90 degrees inferiorly to run in the crease anterior to the earlobe. The purpose of this configuration of incisions is to create a defined beginning and ending for the tragus. If the incisions are not made in this manner and a more curved or linear approach is taken, the resulting scar contracture will result in a hidden and chopped off appearance to the tragus.
The incision is then drawn to follow the crease in front of the ear lobule. Three to 4 millimeters superior to the inferior aspect of the lobule, a cuff of 2 mm of cheek skin is left attached to the lobule. The purpose of this incision is to preserve the natural sulcus of the ear lobule (Fig. 12.5) and thus create a far superior aesthetic result compared with putting thick cheek skin directly next to thin ear lobule skin.

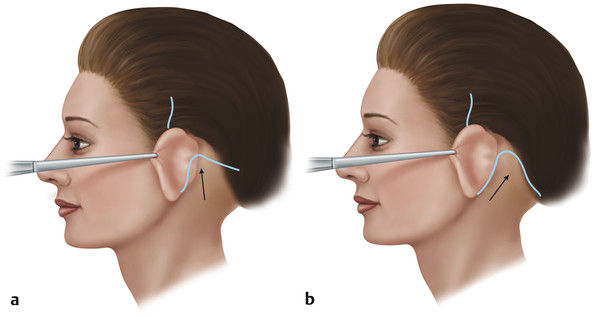
In the past, it was common to place the postauricular skin incision on the posterior surface of the concha and then turn the incision posteriorly over the occipitomastoid skin (Fig. 12.6 a). The results from this incision pattern included postauricular webbing, hypertrophic scarring, and obliteration of the auriculomastoid crease. In addition, when marking the postauricular skin incision, it is critical to consider the direction of the draping of the neck-flap skin. The skin of the neck flap should drape in a more posterior and slightly superior direction to allow for optimal improvement of the neck and the submental areas. A more vertical redraping will give more improvement to the neck and cervicomental angle but will result in less improvement in the submental area. If a thin incision is placed on the posterior surface of the concha, a more vertical redraping of the flap skin is required to get the donor site on the ear closed, thus compromising the improvement in the neck. The postauricular incision is marked such that it will fall directly into the postauricular crease (Fig. 12.6 b). At a vertical level approximating the top of the tragus, the markings turn posteriorly over the mastoid area to fall along the occipital hairline. The vertical level of the occipital incision will vary among patients, depending on their individual needs. Frequently, in patients undergoing secondary facelifts, there is not much skin to be removed in the postauricular area. In these patients, it may be wise to place the incision lower over the mastoid than the original incision. In the event there is excess skin after the skin undermining and treatment of the SMAS, the intervening tissue that is between the current incision and the previous incision can be removed.
12.3.4 Planning the Occipital Incision
In planning the occipital incision, the considerations are similar to those for temporal incisions. The key issues are displacement of the hairline and scar visibility. The occipital incision has been traditionally placed directly back into the occipital hair from the top of the postauricular incision (Fig. 12.7 a). The intent of the incision pattern is to hide the scar in the occipital hair. In patients who have a minimal amount of skin shift, this incision can give acceptable results. This is typically seen in a young patient with a mild neck deformity for whom the occipital incision is being used to access the lateral neck. In patients who have large skin shifts, the result will be transposition of non-hair-bearing skin into the occipital area. These patients end up having a notch in their occipital hairline, and they are rendered “hairline cripples” (Fig. 12.8). To hide the notch, they must wear their hair long and down.
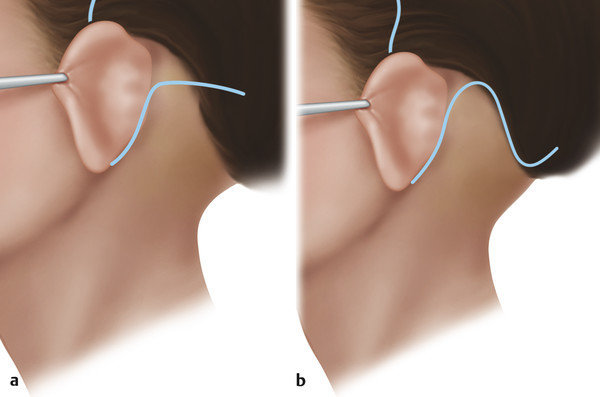

As in the temporal area, skin pinches are used to assess the amount of laxity of the skin in the neck with a posterior and superior shifting of the flap skin. When there is less than 2 cm of displacement of the skin in the occipital area, it is possible to make the “traditional” occipital incision into the hair without significantly shifting the occipital hairline. When the estimated amount of laxity is greater than 2 cm, the incision should be placed along the occipital hairline. The incision is designed to follow the occipital hairline for a short distance. The incision is then turned posteriorly into the occipital hair at the junction of the thick and thin hair to prevent an obvious scar in the fine hair over the posterior neck (Fig. 12.7 b).
To determine the posterior end of the incision, the neck is examined. A line is drawn perpendicularly from the lowest neck crease to the occipital area. This point is the appropriate end of the occipital incision. At the posterior aspect of the incision, the markings again go into the hair in a similar manner as in the temporal area; a small hair-bearing inferiorly based flap is placed into the hairline for management of the dog-ear.
12.3.5 Planning the Submental Incision
Not all patients will require a submental incision for their procedures, but most will need a submental incision. This incision has traditionally been placed into the submental crease in an effort to minimize scar visibility. The problem with placing the incision into this crease is that it deepens the crease and highlights the double-chin deformity, especially with downward gaze.
The use of the submental incision allows for completion of the dissection of the anterior neck. Dissection from the submental incision can be used to release the submandibular ligaments that are responsible for formation of the jowl. The submental incision can also be used for modifications to the neck, including neck defatting, removal of subplatysmal fat, tangential excision of the digastric muscles, excision of the submandibular glands, and suturing of the platysma muscle.
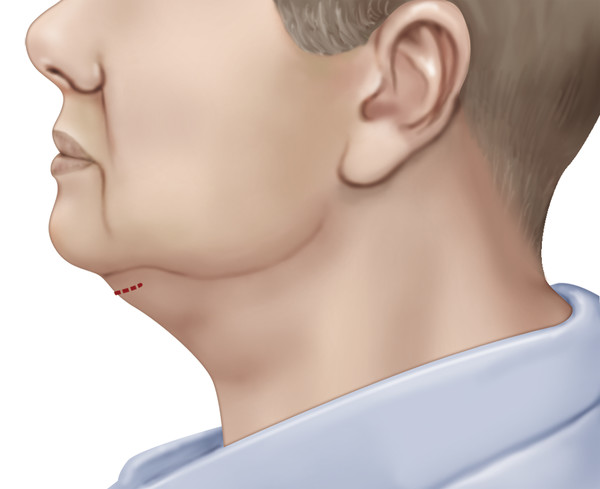
Proper placement of the submental incision is approximately 1 cm posterior to the submental crease. The incision is approximately 2.5 cm long. It is important to keep the incision as short as possible to ensure that the incision cannot move up over the mandible onto the face. The cutaneous connection to the bone responsible for formation of the crease can then be released by dissecting anteriorly to the incision and then over the chin for a short distance (Fig. 12.9).
Related posts:
 6. Facial Sculpting and Facial Slimming with Neurotoxins
6. Facial Sculpting and Facial Slimming with Neurotoxins
 20. Comparison of Midface Rejuvenation Techniques
20. Comparison of Midface Rejuvenation Techniques
 22. Lower Eyelid Blepharoplasty
22. Lower Eyelid Blepharoplasty
 23. Lateral Canthal Complications in Aesthetic Eyelid Surgery: Prevention and Reconstruction
23. Lateral Canthal Complications in Aesthetic Eyelid Surgery: Prevention and Reconstruction
 5. Energy-Based Treatments for Facial Aging
5. Energy-Based Treatments for Facial Aging
 10. Foreheadplasty: Recognizing and Treating Aging in the Upper Face
10. Foreheadplasty: Recognizing and Treating Aging in the Upper Face
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


