12 Designing the Oncoplastic Operation
Careful patient selection and preoperative planning are key components to the success of any oncoplastic operation for breast cancer. An accurate preoperative evaluation of the clinical and biologic features of the tumor and the morphologic aspects of the breast allows the surgeon to determine whether a radical or conservative approach is preferable and to select the most effective surgical technique. The available options are discussed with the patient, highlighting the advantages, disadvantages, and technical challenges of each procedure.
Breast-conserving surgery (BCS) is our treatment of choice and is used in all patients who have a favorable tumor diameter/breast size ratio and when optimal local control can be achieved without compromising the cosmetic result. 1 – 3
Oncoplastic skills may be incorporated in the surgical planning in less favorable cases, when traditional breast-conserving techniques may expose them to a higher risk of local deformity. Total mastectomy is considered mandatory only for multicentric disease, T4 and inflammatory tumors, extensive malignant mammographic microcalcifications, or when clear surgical margins cannot be achieved without generating a significant risk of local deformity, even with the use of oncoplastic techniques. 4 , 5 Oncoplastic skills are incorporated in the surgical planning for breast-conserving surgery and a total mastectomy. 2 , 3 , 6
Preoperative Planning for Breast-Conserving Oncoplastic Procedures
When a breast-conserving approach is feasible, the selection of the most appropriate technique is guided mainly by the location of the tumor, the volume and shape of the breast, the size of the lesion, and the morphologic changes that the surgery is likely to cause. For cancers that are small (relative to the breast size) and do not require extensive parenchymal excisions, traditional techniques of BCS can be applied with excellent cosmetic results.
If more than 20% of the parenchymal volume is to be resected to achieve adequate local control, particularly for cancers located in the central, medial, or lower pole of the breast, using oncoplastic techniques helps to avoid the risk of an unpleasant cosmetic outcome. 7 – 11
The planning for oncoplastic BCS includes the following:
Placing accurate preoperative skin markings according to the technique selected for parenchymal excision
Evaluating the risk that the parenchymal excision may displace the NAC and adapting the skin drawings to ensure that it may be repositioned to the center of the breast mound, if significantly displaced
Evaluating the most appropriate volume displacement or volume replacement technique to be used to reshape the defect after resection
Evaluating the need for symmetrization of the contralateral breast and selecting the most appropriate technique
Planning for oncoplastic BCS includes selecting the most effective technique for parenchymal excision and placing accurate preoperative markings on the skin. The breast size and the patient’s age, general health status, and personal wishes are also taken into account.
Planning The Oncoplastic Approach by Tumor Location: Volume Displacement Techniques
Periareolar Lesions
Oncoplastic volume displacement techniques provide excellent outcomes in the treatment of periareolar lesions. For breasts with minimal or moderate ptosis, we prefer a donut mastopexy or a batwing mastopexy, and for breasts with severe ptosis or redundant skin we favor a reduction mammaplasty pattern.
Patient Example
Donut Mastopexy
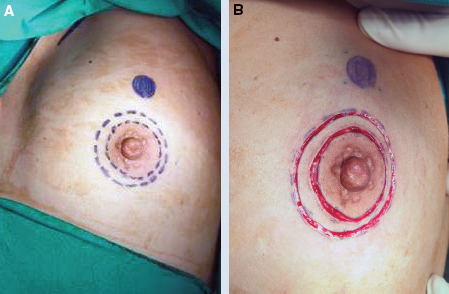
The donut mastopexy approach provides comfortable access to any lesion in the periareolar region compared with traditional breast-conserving techniques. Two concentric circles with different diameters are designed around the nipple (A). The areolar skin is stretched only mildly when the inner circle is designed to avoid the potential for the final areolar diameter being too small. The diameter of the inner circle is usually from 4 to 4.5 cm, depending on the size of the breast. The diameter of the outer circle should not exceed the diameter of the original areola by more than 20 to 25 mm to prevent widening the circumareolar scar or excessive flattening of the breast.
The initial step is the incision of the inner circle, which will represent the new border of the areola (B).
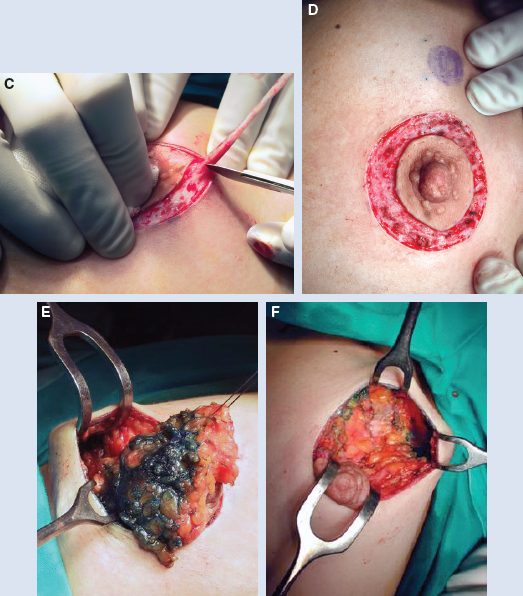
The outer circle is incised, whereas the donut of skin between the two circles is excised. Through this incision, any periareolar lesion can be easily accessed (C and D). Quadrant resection of the breast parenchyma can be performed through a wider incision that extends to the pectoralis fascia, allowing better control of the tumor removal than when the resection is performed through conventional conservative skin incisions (E and F).
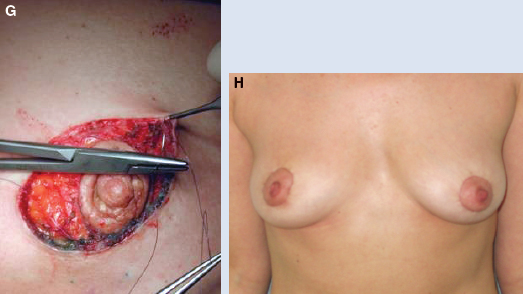
The breast can be reshaped appropriately by displacing the residual gland. To do this, we normally separate the residual gland off of the pectoralis fascia using electrocautery, paying attention to limit the number of major perforating vessels that are sectioned to avoid interference with the blood supply to the residual glandular tissue. After hemostasis is achieved, the residual breast parenchyma is reapproximated to facilitate a natural-appearing breast. Sutures are placed in the deep portion of the residual gland, just above the fascia, to secure the posterior edges in their new position. We normally use 2-0 Vicryl sutures for this purpose and 4-0 absorbable sutures in the dermis to reapproximate the superficial portion of the breast. If needed, a purse-string suture is used to reduce the diameter of the larger circle and is then sutured to the new border of the areola, leaving only a periareolar scar at the end of the procedure (G). The patient is shown 6 months after surgery. Only a periareolar scar is visible (H).
Axillary dissection is usually performed through a separate incision, but occasionally through the same periareolar incision. If the two circles are concentric, the NAC is not elevated; if the outer circle is centered around a point located higher than the existing nipple, the nipple-areola complex can be elevated slightly as a consequence of the procedure. After the skin is closed, the thorax is wrapped in an elastic bandage to reduce the risk of hematoma formation.
Patient Example
Batwing Mastopexy
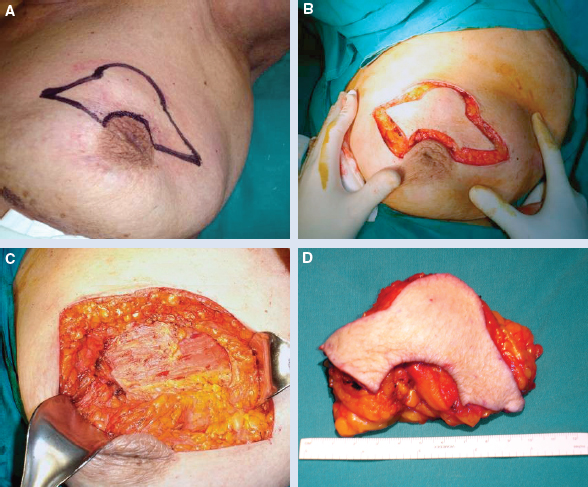

The batwing mastopexy approach is ideal for cancers located in the upper periareolar region, particularly when the lesions are in close proximity to the skin. Two semicircles are designed, one on the border of the areola and one 20 to 25 mm above it, connected with angled wings on each side of the areola (A). The skin incisions should be designed with the patient sitting upright. The areolar semicircle is incised first, followed by the upper semicircle and the wings (B). A full-thickness lumpectomy is performed (C and D), and the residual gland is lifted off of the pectoralis fascia, allowing adequate tissue advancement and defect remodeling. Breast defect remodeling requires skills similar to those needed for the donut mastopexy.
The procedure allows ample removal of the skin overlying the lesion and therefore can increase the safety of the oncologic control of cancers located superficially. Some uplifting of the NAC may result at the end of the procedure, but normally this does not cause significant asymmetry.
The patient is shown 4 months after surgery (E).
Reduction Mammaplasty
For patients with severe ptosis, reduction mammaplasty patterns may offer better results.
The resection of the tumor with wide macroscopically clear margins can be achieved easily in combination either with an inferior or superior pedicled flap to recreate a normally shaped breast and to shift the NAC to an appropriate position.
Related posts:
 6 Breast-Conserving Therapy: Decision-Making and Anticipating the Unfavorable Aesthetic and Functional Result
6 Breast-Conserving Therapy: Decision-Making and Anticipating the Unfavorable Aesthetic and Functional Result
 10 Breast Radiotherapy in Oncoplastic Surgery
10 Breast Radiotherapy in Oncoplastic Surgery
 11 Indications and Benefits of Oncoplastic Breast Surgery
11 Indications and Benefits of Oncoplastic Breast Surgery
 9 Improving the Quadrantectomy Defect
9 Improving the Quadrantectomy Defect
 14 Psychosocial Aspects of Oncoplastic Breast Conservation
14 Psychosocial Aspects of Oncoplastic Breast Conservation
 13 Timing of the Oncoplastic Reconstruction: Immediate, Delayed, and Delayed-Immediate
13 Timing of the Oncoplastic Reconstruction: Immediate, Delayed, and Delayed-Immediate
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


