10. Foreheadplasty: Recognizing and Treating Aging in the Upper Face
10.1 Introduction
The foundation for rejuvenation of the upper face published by Dr. Jose Vinas has produced excellent results for many decades. 1 Unfounded criticism of the procedure of forehead surgery caused the application of these techniques not to keep up with the procedures for the face and neck.
Surgeons who erroneously used pressure dressings instead of precise hemostasis during surgery could expect loss of hair, loss of blood supply to the forehead flaps, and failure to obtain the desired results.
Patients with male pattern baldness were not considered for foreheadplasties by surgeons because of visible scars on bald or balding scalps. In addition, patients might be disappointed as a result of bizarre expressions from overresection of forehead muscles, contour irregularities after imprecise muscle sculpting, inappropriate appearances resulting from eyebrow malposition, and hairline shifting. This chapter relates concepts and techniques that have eliminated these problems and pleased many patients.
10.2 Facial Aging
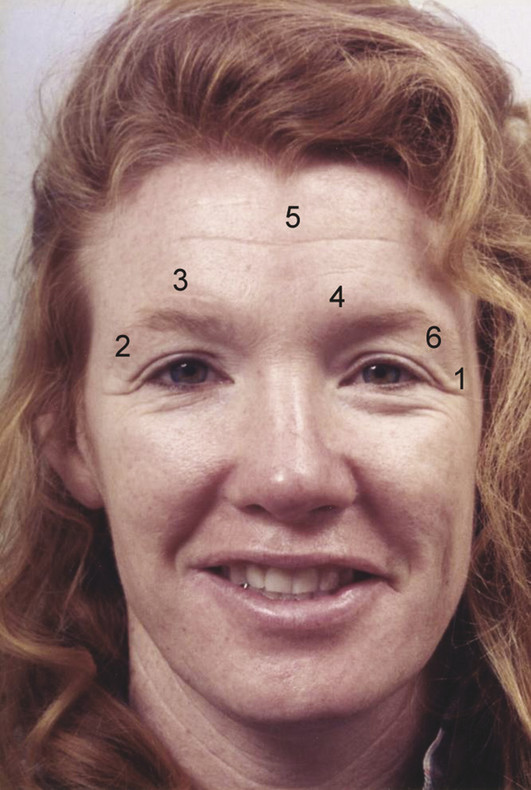
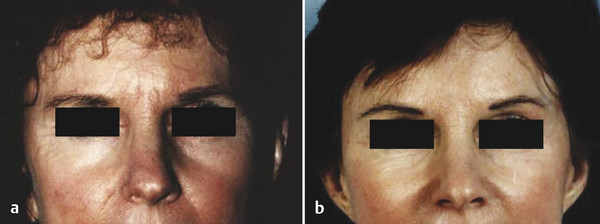
The terms browlift and forehead lift imply that aging in the upper face consists only of eyebrow ptosis. Forehead rejuvenation is a better term. Descent of the eyebrow does occur; however, it is only one component of aging. Fig. 10.1 demonstrates changes seen in the aging upper face, including an upper eyelid skinfold laterally off the lid, glabellar frown lines, transverse forehead creases, large corrugator muscles, transverse nasal creases, low-lying eyebrows, a low lateral brow, and pseudoblepharochalasis.
10.2.1 Inappropriate Expressions
Actors, artists, and cartoonists are well aware of the effect of the eyebrows, glabella, and forehead in communicating feelings. Everyone can recognize expressions of fear, anger, sadness, surprise, and fatigue when shown only the upper face. Often changes of upper facial aging show these expressions, which may be misinterpreted by others. A face may appear inappropriately tired, bored, or sad.
10.2.2 Upper Facial Analysis
Many features of the upper face show sex differences, and it is an error to apply the same aesthetic goals to both men and women. The male eyebrow generally is lower on the brow than is the female eyebrow and is nearly horizontal with less of an arch. An arched eyebrow is a feminine characteristic that appears unnatural on the male face. Transverse forehead creases and glabellar frown lines, which are thought of as old or objectionable on female foreheads, may give the appearance of strength, power, or wisdom on the male face. Often it is better to soften these features rather than eliminate them. Differences exist between men and women in their upper eyelid appearance. The male upper eyelid is fuller, with a fold, and this is a reason to not overelevate the male brow.
10.2.3 False Appearance of Eyelid Excessive Skin
A frequent error is performing an upper lid blepharoplasty when a foreheadplasty is needed. This mistake is due to using a memorized technique rather than anatomical analysis. As the upper face ages and the brow descends, brow skin will move into the orbit, producing an illusion of eyelid skin redundancy known as “pseudoblepharochalasis” (Fig. 10.1). Attempts to treat pseudoblepharochalasis with traditional blepharoplasty techniques will result in a sad, tired-appearing patient with smooth eyelids and a visible scar extending onto the lateral periorbital region, and it may cause difficulty closing the eyes during sleep.
Brow ptosis should be suspected in all patients who appear to have a redundancy of eyelid skin, even if the brow and forehead initially appear normal. Frequently, patients will be holding up their eyebrows while asking, “Can you fix my eyelids?” The surgeon should reposition the patient’s brow and observe the effect produced. Often it is obvious that eyelid surgery is unnecessary. Sometimes a combined problem is present.
An upper lid skinfold that runs off the eyelid is brow ptosis. Often it is evident only after the forehead is relaxed.
Deep transverse forehead creases and frontalis hyperactivity indicate that a patient has brow ptosis (Fig. 10.1). These effects are the result of the patient trying to clear partial visual obstruction in the superior-lateral fields. Repositioning the brow will relieve brow skin encroachment on the upper lid and eliminate frontalis action and thus produce diminution in forehead wrinkling.
10.3 Complete Facial Rejuvenation
Many patients fail to recognize changes in their upper faces and focus the surgeon’s attention on their necks. In other instances, surgeons fail to appreciate upper facial aging, the inappropriate expressions these changes produce, or the distinction between eyelid excessive skin and brow ptosis.
Often changes of the forehead, and not of the lower face and neck, produce the most significant improvements in appearance. Rejuvenating only the lower face may produce the facelift deformity of “young face–old forehead.” Some patients are unable to recognize specifically that as such, but they feel general disappointment with the lack of improvement in their appearance after a facelift. Others are aware of it and able to articulate it eloquently.
10.4 Patient Understanding
Many are not aware of the changes that occur in their upper faces as they age, and most are unaware that a procedure exists to correct them. A surgeon seeking a happy patient must help the patient recognize these changes and explain their significance.
The consultation starts by giving the patient a hand mirror and asking him or her to consider how others interpret the message of his or her appearance: a pleasant face, an annoyed face, a stern face, an angry face, or a tired face? Often the patient will say, “I look tired even when I’m not” or “I need to smile all the time or everyone thinks I’m angry.” The patient may also say, “I look sad, and my friends are always asking me if something is wrong.”
Elevate the eyebrow and place it in a pleasing, appropriate configuration. Then allow the patient to observe the change in his or her appearance. Point out the improvements in the upper lid, in the lateral periorbital region, and in the upper third of the nose. Most patients will begin to understand the distinction between brow ptosis and excessive eyelid skin.
10.5 Anatomical Surgical Planning
Planning rejuvenation of the upper face includes the desired elevation and configuration of the eyebrows. These decisions are made in conjunction with the patient. The supraorbital rim is used as the reference. The skin overlying it is marked medially, laterally, and centrally with the patient seated and forehead at rest. The eyebrow is then elevated to the desired level and positioned in a pleasing and appropriate configuration. The skin overlying the supraorbital rim is then marked again. The distance between the marks is equal to the needed elevation at each location. 2 , 3 , 4 , 5
Evaluation and configuration of the eyebrow are artistic determinations. Marks and measurements serve only to quantify the artistic judgment and allow it to be recorded. The amount of elevation needed is usually not the same on each side of the face because proper position of the eyebrow reflects a balance between the eyebrow and the rest of the face. Most faces are asymmetrical. Facial asymmetry should be considered an inherent characteristic of beauty. All attractive faces are asymmetrical to varying degrees, and on close inspection, the surgeon should be able to identify a large and small side of the face, a large and small eye, and a large and small cheek, jaw, brow, and so on. 5 Failure to recognize this and attempts to force symmetry surgically will create aesthetic imbalances that are unusual, uninteresting, or unnatural. Surgeons able to help patients appreciate the beauty of their own asymmetries preoperatively can avert unnecessary concern postoperatively, when asymmetry is first noticed, as the face comes under more detailed scrutiny.
10.5.1 Incisions
When the amount of elevation of the eyebrows has been determined, the location of the incision can be selected. Often the surgeon can improve the balance between forehead, face, and hairline. 3 Several basic incisions are used (Fig. 10.2). 6 It should be remembered that 1 mm of eyebrow elevation can produce 1.4 mm of displacement of the anterior hairline. For patients with low hairlines or in whom the predicted shift will be aesthetically acceptable, a coronal (Fig. 10.2 b) or vertex (Fig. 10.2 c) incision is chosen. In bald or balding men, other incision patterns will minimize detectability.
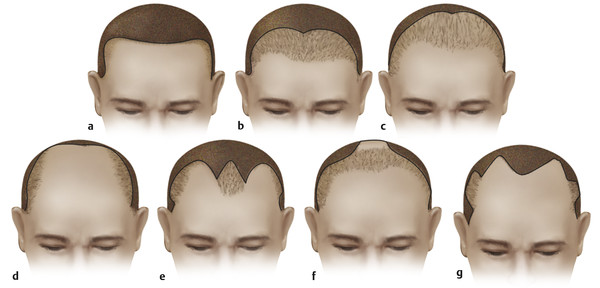
For bald men, the foreheadplasty incision should be placed posteriorly near the lambdoidal skull suture (Fig. 10.2 d). The scar will not be visible in photographs or during conversation. For most bald patients, healing of the skin in this location is excellent, and the scar is usually inconspicuous even on close inspection. Scar depression is prevented by trimming the scalp skin only and leaving the galea.
For men with occipital baldness and sparse anterior hairlines, the preceding incision is modified to a “paddle-type incision” (Fig. 10.2 f). This incision pattern allows reduction of the balding area at the crown by simultaneous excision of the bald scalp and advancement of hair-bearing scalp. For men with thicker anterior hairlines who prefer its preservation, an anterior hairline incision pattern (Fig. 10.2 a, e, g) is selected.
Several incision patterns are useful in men with frontotemporal balding. The most commonly used is the hairline incision (Fig. 10.2 a). This incision will prevent retrodisplacement of hairlines and can shorten the forehead. Some surgeons have avoided using this incision because they consider the scar unacceptable 7 ; however, this will not be so if the incision is made properly and closed without tension. To obtain optimal results, the incision must be made precisely parallel to the hair follicles and the flap suspended from three points only. All points in between these suspension points should be trimmed with 2 to 3 mm of excess and closed under no tension. Suture marks are avoided by use of half-buried vertical mattress sutures of 4–0 nylon tied on the scalp side.
When a hairline incision is used in men with marked temporal thinning, it is usually better to run the temporal portion of the incision through the thinning area rather than along the more posterior interface of thin and thick hair. If the incision is made at the interface of thin and thick hair, this interface will be exaggerated which can appear unnatural. Keeping the incision within the thinning hair is the proper choice for incision location.
For men and women with temporal recession of the hairline, but with low central forelocks (Fig. 10.2 e), a W incision is used. This pattern will shorten the forehead laterally but lengthen it centrally, creating a more uniform and youthful-appearing hairline. The tips of the posterior flap must be “toed in” against the central hairline in a Y-to-V fashion.
An “interlocking M’s” incision is used for men with both central and temporal hairline recession (Fig. 10.2 g). This pattern allows shortening of both central and lateral forehead but keeps scars off the lateral portion of the temporal hairline, where hair inclines posteriorly and the scars are usually obvious. V–Y advancements are usually possible at the apex of the balding temporal triangles. As is the case with any anterior incision (Fig. 10.2 a, e, g), it should be inconspicuous. Patients should be warned they will experience postincisional paresthesia for as long as 4 to 6 months after surgery.
If the temporal portion of the foreheadplasty incision is turned posteriorly (Fig. 10.3, solid line A), proper shift of the forehead flap (superiorly only) will result in a defect that cannot be closed (Fig. 10.3, defect X). Such an incision will force compromised elevation of the lateral brow and necessitate undesirable posterolateral shift of the flap and the temporal hairline. A postauricular positioning of the temporal portion of the forehead lift incision (Fig. 10.3, pink dashed line B) will result in a compromised effect on the temple and upper lateral face owing to tethering of the flap at the ear. A short preauricular incision (Fig. 10.3, dotted line C) has a similar drawback.
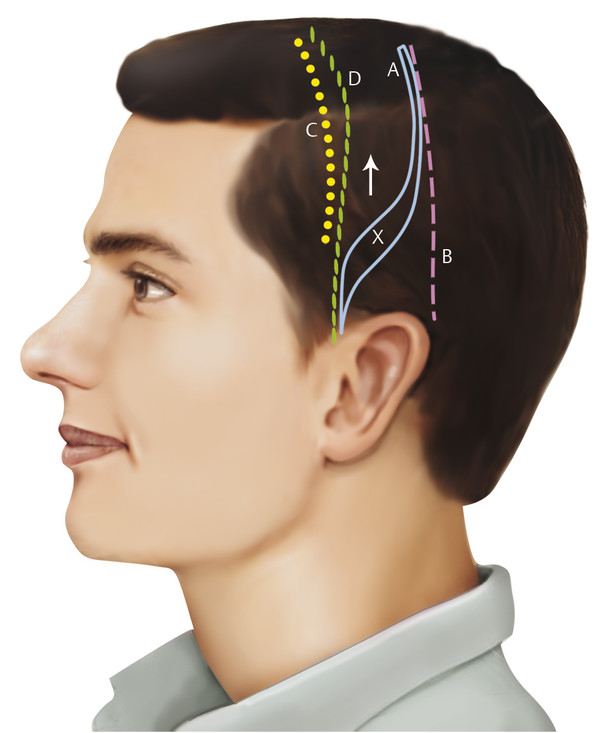
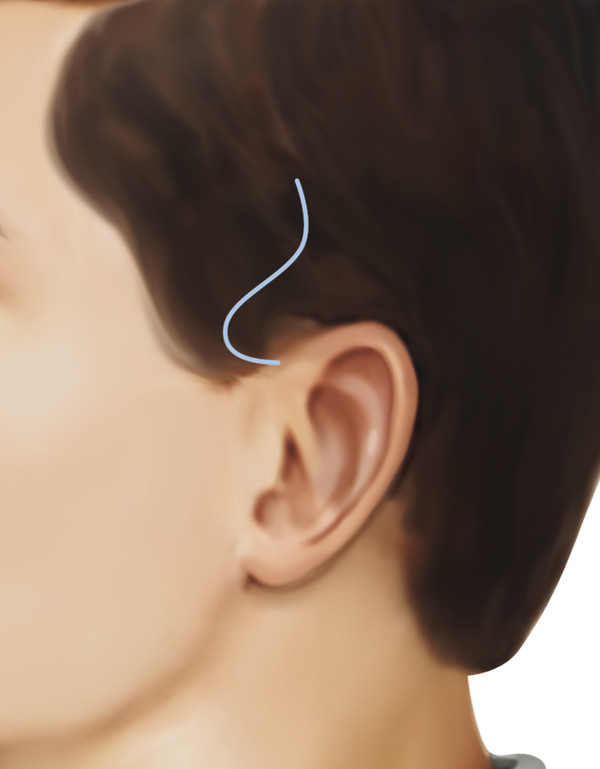
A preauricular positioning of the temporal portion of the foreheadplasty incision beginning anterior to the root of the ear and extending directly superiorly eliminates these problems (Fig. 10.3, green dashed line D). If a facelift is to be performed concurrently with a foreheadplasty (or subsequent to it), a small hair-bearing projection of the temporal scalp is preserved to prevent a shift of hairless preauricular skin into the temporal hair (Fig. 10.4). Frequently, this occurrence is mistakenly interpreted as “a wide scar.”
10.6 Modification of Corrugators
After selecting the appropriate pattern of incision, an estimate of the size and volume of the corrugators should be made by asking the patient to scowl or frown. Frequently, surgeons fail to appreciate the extent of muscle hypertrophy laterally, which can result in inadequate resection of these areas that can produce the appearance of small “horns.”
Reducing corrugator muscles often improves a heavy brow and helps to eliminate an angry appearance. In some patients, however, a “Neanderthal” appearance due to a heavy or prominent supraorbital ridge requires improvement by bony contouring.
10.6.1 Deep Glabellar Creases
The creases should be evaluated with the patient at rest and with the patient frowning. Mild deformities require only attenuation of corrugators. For moderate creases, incisions are made through muscle to subcutaneous fat 10 to 15 mm on each side of the crease on the inside of the flap. With healing, the muscle will contract behind the crease and support it. In severe cases, a graft of galea or temporalis muscle fascia is placed beneath the muscle flap after release and sutured into place for maximum muscle contraction that produces filling.
10.6.2 Frontalis Muscle Hyperactivity
Frontalis modification is determined preoperatively by the severity of transverse forehead wrinkling and the degree of “resting” muscle contraction. Some patients with brow ptosis may be unable to relax their foreheads fully, even when asked to do so, and require more extensive muscle thinning. Never is all muscle excised. Proposed frontalis modification is usually recorded as the predicted percent reduction in its activity.
10.6.3 Facial Incisions
Making incisions properly is a key step in which the surgeon exercises direct control over the detectability of the resultant scar. To minimize detectability, all incisions within hair-bearing scalp or at a hair–scalp, hair–forehead, or beard–skin junction are made parallel to hair follicles to prevent injury to them and will not result in alopecia appearing as a “wide scar.” Hair follicles are inclined to the same direction as the hair shafts, and therefore incisions should begin parallel to the hair shafts.
Hair shaft–hair follicle inclination will be different at different places along the planned incision. The angle of the scalpel blade needs to change as the direction of the hair follicles changes (Fig. 10.5). It is impossible to determine changes in hair shaft–hair follicle inclination if hair has been shaved, trimmed, covered with surgical lubricants, bundled in rubber bands, or distorted by head drapes.

10.6.4 Forehead Flap Elevation
For the rare patient needing eyebrow elevation only, simple excision of forehead skin or scalp without elevation of a forehead flap may suffice. Most patients, however, will benefit from correction of inappropriate expressions, modification of muscles, and elimination of expression lines. These corrections require a flap to be raised.
The plane beneath which the forehead flap is elevated has been the subject of much debate, and various authors have reported good results using subgaleal, 1 , 6 , 8 subperiosteal, subcutaneous, 9 , 10 and dual-plane dissections. 11 Subgaleal dissection is preferred. The subgaleal plane is easy to identify and dissect and is bloodless and allows excellent access to hypertrophic muscles. Dissecting beneath the frontalis creates a myofasciocutaneous flap that provides maximal protection of hair-bearing areas. A subgaleal dissection also leaves the pericranium (cranial periosteum) intact, which provides for adhesion of the flap after scalp repositioning, thereby minimizing recurrent ptosis. The subgaleal approach will result in transection of some sensory nerve branches, creating numbness posterior to the incision. A subcutaneous dissection, although it avoids the sensory changes, is technically demanding and places the flap at a greater risk for slough and hair loss. These risks outweigh the rarely troublesome paresthesia associated with deeper-plane techniques.
The scalp incision goes down to the galea, which is divided with scissors. Bleeding will be encountered laterally over the temporal region. Cautery should be used carefully at superficial levels and avoided near the plane of hair follicles to prevent peri-incisional alopecia. Bleeding from superficial areas of the edge of the posterior flap is best managed by applying a hemostat to the galea and allowing it to drape posteriorly, which compresses the flap edge (Fig. 10.6). Neurosurgical hemostatic clips work well on the anterior flap but in practice are a bit more cumbersome to use posteriorly. Cautery can be used along the edge of the anterior flap where skin or scalp will be resected. Scalp is never excised from the lateral portion of the anterior or posterior flaps, and cautery should not be used near follicles in these areas.

A combination of blunt and sharp technique in conjunction with gentle traction is used to elevate the forehead flap in a subgaleal plane. Sharp dissection is usually necessary centrally and at the supraorbital ridges. Blunt dissection centrally or at the brow will result in pericranial stripping and painful avulsion of tiny pericranial sensory nerve branches.
Lateral dissection proceeds directly beneath the frontotemporal branch of the facial nerve, 12 , 13 , 14 , 15 which is sometimes visible in the anterior flap. It can be injured at the lateral brow, where the flap becomes more adherent to the bone. Cautery should be avoided in this area. Dissection inferiorly over the zygomatic arch is dangerous and unnecessary.
Dissection over the brow and supraorbital rim is best carried out with blunt-tipped Iris scissors using the technique of “parallel dissection” with one blade of the scissors inserted beneath a thin layer of tissue. If no structures of importance are identified, the scissors are closed and the action repeated. With the use of this technique, the flap is released from the supraorbital ridge and the dissection carried to the orbital septum. Complete release can be obtained in this manner, and the dissection need not proceed beneath the periosteum.
As the flap is raised centrally, the supraorbital nerves can usually be identified on the posterior surface of the flap. As the brow is approached, the foramen through which this nerve exits can be palpated through the skin as a notch along the supraorbital rim at the level of the pupil in most patients. 16 In patients in whome a notch is not palpable, the nerve usually exits through the foramen more superiorly. 7
Flap elevation is completed by undermining the soft tissue overlying the nose. This maneuver does not contribute to flap release, but if done correctly, it will produce considerable improvement using a Metzenbaum scissors with the tips slightly opened in the manner in which one would use a periosteal elevator. With the tips down, the subperiosteal plane is entered at the root of the nose. The tips are then turned upward, and a tunnel 10 mm wide is dissected along the dorsum to the nasal tip. This dissection allows a subtle elevation of nasal soft tissue when the forehead flap is repositioned and thus counteracts, to some extent, soft tissue aging of the nose. Equally, if not more, important, however, is the creation of the tunnel along the dorsum itself. Postoperatively, this tunnel and the nasal tip will fill with edema fluid, giving the illusion of softness, refinement, and narrowing (Fig. 10.7). Examination of last postoperative photographs has shown this effect to persist to some degree; in most patients, this narrowing effect will be lost if the tunnel was made too wide.
Related posts:
 6. Facial Sculpting and Facial Slimming with Neurotoxins
6. Facial Sculpting and Facial Slimming with Neurotoxins
 20. Comparison of Midface Rejuvenation Techniques
20. Comparison of Midface Rejuvenation Techniques
 22. Lower Eyelid Blepharoplasty
22. Lower Eyelid Blepharoplasty
 23. Lateral Canthal Complications in Aesthetic Eyelid Surgery: Prevention and Reconstruction
23. Lateral Canthal Complications in Aesthetic Eyelid Surgery: Prevention and Reconstruction
 5. Energy-Based Treatments for Facial Aging
5. Energy-Based Treatments for Facial Aging
 12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


