1 Surgical Principles
Abstract
“Surgical Principles” provides a step-by-step overview of the treatment of the ophthalmic plastic surgery patient, from preoperative patient evaluation through postoperative care. The fundamental principles and techniques essential to success in ophthalmic plastic surgery are similar to those that underlie other branches of surgery. Careful attention to detail, meticulous surgical technique, and an utmost respect for the functional requirement of the eye are of paramount importance. A surgeon who is well versed in fundamental surgical principles and techniques will avoid unnecessary complications and the requirement for secondary procedures.
1.1 Introduction
The fundamental principles and techniques essential to success in ophthalmic plastic surgery are similar to those that underlie other branches of surgery. Careful attention to detail, meticulous surgical technique, and an utmost respect for the functional requirement of the eye are of paramount importance. A surgeon who is well versed in fundamental surgical principles and techniques will avoid unnecessary complications and the requirement for secondary procedures.
1.2 Preoperative Patient Evaluation
The surgeon should develop a routine for questioning and examining patients to avoid omitting important questions or crucial aspects of the examination. Obtaining a careful detailed history about the presenting problem from the patient is essential. Details should also be obtained about the past ophthalmic history, past medical and surgical history, current medications, allergies, family, and social history. Time spent in obtaining the history has additional benefits:
It provides the surgeon with information about the patient’s potential expectations.
It provides an opportunity for the surgeon to establish a rapport with the patient.
It allows the surgeon to simply observe the patient and detect subtle physical signs, which may otherwise be overlooked, such as signs of aberrant reinnervation of the facial nerve, blepharospasm, hemifacial spasm, an abnormal head posture, frontalis overaction, and facial asymmetries.
The patient examination should be methodical. A record of the patient’s corrected visual acuity and a basic ophthalmic examination should form part of the assessment of every patient presenting with an eyelid, orbital, or lacrimal disorder. The detailed examination methods for various conditions are discussed in their respective chapters. Any ancillary laboratory or imaging investigations should be selected on the basis of the clinical evaluation of the patient and not simply performed as a blind “workup.”
It may be helpful to obtain copies of patient records from other institutions where the patient has previously been treated. The details of previous surgical procedures, the results of previous investigations and imaging, and original histology slides should be sought wherever this is relevant. A review of previous imaging and histology slides rather than a reliance on previous reports can prove to be invaluable.
1.3 Documentation
The surgeon must ensure careful and accurate documentation of the history and examination findings as well as the diagnosis, management plan, and preoperative discussion with the patient.
High-quality preoperative photographs should always be taken. These are essential for patients who will be having ophthalmic plastic and reconstructive surgery. They serve a number of useful and important purposes:
A learning and teaching aid for the surgeon.
A verification of the patient’s disorder for health care insurance companies.
An aid to defense in the event of a medicolegal claim.
An aid to the patient in legal proceedings after accidents and assaults.
To jolt the postoperative memory of a forgetful patient.
Key Point
Written patient consent should be obtained before the photographs are taken. It should be made clear to the patient how the photographs may be used.
The treatment options should be discussed with the patient. This should include the option of not being treated. The advantages, disadvantages, risks, and potential complications should be discussed with the patient and relatives if possible. The risks and the incidence of complications need to be outlined in an open and honest manner. Serious or frequently occurring risks must be discussed and documented. This should be undertaken in a manner that neither frightens nor offends. The consequences of complications and their management should also be outlined. If the patient expresses a wish not to be given this information, this must be clearly documented. The consultation should be followed by a detailed letter summarizing this information, which should be sent to the patient’s family practitioner with the patient’s permission, and a copy should be sent to the patient or, in the case of children, to the parents.
Any periocular surgical procedure can be associated with serious ophthalmic complications. The surgeon should therefore avoid describing any periocular procedure as “basic,” “straightforward,” “simple,” “minor,” or “routine.”
Key Point
For purely elective procedures, the patient should be encouraged to consider the information carefully before making a decision to proceed. This may necessitate a further consultation or attendance at a preassessment clinic to obtain fully informed consent and to answer any residual queries. This is particularly important for a patient seeking aesthetic surgery. The patient should not be asked to sign a consent form for an elective procedure on the day of surgery. The risks and potential complications that have been discussed should be documented in the patient’s records.
A surgeon who is fully conversant with the nature of the surgery and who is qualified to take informed consent from a patient should complete the surgical consent form. The consent form must be legible and must document the correct side and the precise details of the surgical procedure to be undertaken without the use of abbreviations. All known risks, particularly serious or common risks, must be documented on the consent form and in the patient’s records, and it is wise to include these in the postconsultation correspondence.
1.4 Selection of the Appropriate Surgical Procedure
The surgical procedure that is best suited to the individual requirements of the patient should be selected; for example, a patient whose other eye has poor visual function should not be subjected to a Hughes tarsoconjunctival flap procedure for the reconstruction of a lower eyelid defect. An alternative surgical procedure should be selected.
An operation that is not indicated will not benefit a patient no matter how skillfully it is performed. For example, a patient whose blepharoptosis is related to giant papillary conjunctivitis that has been overlooked by the failure to evert the upper eyelid will not benefit from any surgical procedure.
The patient’s age and general health must be taken into consideration. Under certain circumstances the patient’s best interests may be served by advising against surgical intervention.
1.5 Surgical Planning and Communication
Each procedure should be planned carefully. The timing of surgical intervention may be crucial to the outcome (e.g., an orbital floor blowout fracture with signs of orbital tissue entrapment in a child should be managed without delay, whereas for the same clinical scenario in an adult a delay of 10 to 14 days or more is usually advisable). Any significant delay in the management of a child could result in an ischemic contracture of the inferior rectus muscle with a poor prognosis for the restoration of a satisfactory field of binocular single vision.
Preoperative planning ensures that the surgical team is aware of the required instrumentation and materials. For elective operations, it is ideal to run a preassessment clinic in conjunction with a specialist oculoplastic nurse who can coordinate preoperative investigations, ensure that investigation results are communicated to the anesthetist, communicate potential problems such as undiagnosed hypertension to the general practitioner, and liaise with the operating theater nursing team regarding factors such as ensuring that the required range of orbital implant sizes and socket conformers is available. The operating list should be detailed and should not contain abbreviations referring to surgical procedures.
The scrub nurse needs to be aware of the required preparation and draping of the patient, including the proposed site for the harvesting of a skin graft or dermis fat graft. This ensures that the procedure can be performed efficiently, minimizing tissue exposure and operating and anesthetic time, and thereby minimizing risks to the patient. Preoperative planning is essential when operating as a team with other surgical disciplines.
The lead surgeon who will be responsible for coordinating the preparations for surgery should be determined in advance.
The details of the planned surgical approach should be communicated to the anesthetist. The anesthetist is an essential member of the team and should know details about the following:
The anticipated duration of the operation.
Special positioning of the patient, such as to harvest a dermis fat graft from the buttock.
The potential sites for harvesting autologous tissue (e.g., upper inner arm sites may affect the siting of intravenous lines and a blood pressure cuff).
The requirement for hypotensive anesthesia.
The potential blood loss.
The potential risk of an oculocardiac reflex (e.g., during an enucleation or secondary orbital implant procedure).
Vasoactive agents to be used intraoperatively, including their concentration and volume (e.g., subcutaneous local anesthetic agent injections with adrenaline, topical intranasal cocaine solution).
The potential for postoperative pain (e.g., severe pain may be experienced after an enucleation with placement of an orbital implant, requiring opiate analgesia, whereas severe pain after a lateral orbitotomy may indicate a retrobulbar hemorrhage, which should be investigated and not merely suppressed with opiates).
The necessity to avoid anti-inflammatory agents for a patient after intraorbital surgery.
The requirement for a throat pack.
The requirement to position the endotracheal tube in a specific location (e.g., to one side of the mouth or intranasally when harvesting a mucous membrane graft or hard palate graft).
These details should also be discussed at the time of the World Health Organization (WHO) surgical safety checklist in the operating department before the commencement of the operating list and again at the “time out” discussion before the initiation of anesthesia and for each individual patient.
1.6 Selection of the Most Appropriate Type of Anesthesia
Several types of anesthesia are available:
Topical anesthesia.
Local anesthesia.
Local anesthesia with intravenous sedation.
Regional anesthesia.
General anesthesia.
The selection of the type of anesthesia for an individual patient depends on multiple factors:
The age of the patient.
The general health and emotional status of the patient.
The extent and anticipated duration of the surgery.
The requirement for intraoperative patient cooperation.
The chosen anesthesia should allow the surgeon to complete the surgery in a safe and controlled manner while providing the best possible degree of comfort for the patient. This should be discussed with the patient in advance.
1.6.1 Topical Anesthesia
Local anesthesia may be applied topically (e.g., Minims proxymetacaine by pledget in the inferior fornix to perform a forced duction test). Proxymetacaine causes a minimal degree of discomfort and acts very rapidly. For this reason it is preferred over other topical anesthetic agents for surface anesthesia of the cornea and the conjunctiva. Topical anesthetic agents last for only a short time and should be instilled at regular intervals during surgery on a conscious patient. Care should also be taken to ensure that the anesthetized cornea is protected during the course of surgery (e.g., Lacri-Lube ointment should be instilled into both eyes after the application of the topical anesthetic agent if a traction suture has not been used to close the eye).
Topical agents applied to the skin are very useful to reduce the pain of injections, such as EMLA cream, which contains lidocaine and prilocaine, and is applied to the eyelids before the injection of a local anesthetic agent. A minimum delay of 10 to 15 minutes should be allowed before injection, and great care should be taken to ensure that the cream does not enter the eye. The same topical agent can be very effective for other procedures, such as the injection of a soft tissue filler for the cosmetic improvement of nasolabial folds associated with a midface ptosis. However, a minimum period of 30 to 45 minutes is required for the topical agent to take effect in an area of the face where the skin is significantly thicker.
Topical cocaine 5% is a very effective topical anesthetic agent for use in intranasal surgery, such as a dacryocystorhinostomy (DCR). Co-Phenylcaine (a phenylephrine–lidocaine mixture) nasal spray is a very effective topical anesthetic agent for use in intranasal examinations and minor intranasal procedures in the clinic.
1.6.2 Local Anesthesia
Local anesthesia is most commonly achieved by local infiltration with either lidocaine 2% containing 1:80,000 units of epinephrine for relatively short procedures or bupivacaine (0.5% for adults and 0.25% for children) containing 1:200,000 units of epinephrine for longer procedures. For some procedures, it is preferable to use a 50:50 mixture of lidocaine and bupivacaine. A period of 5 to 10 minutes should be allowed for the local anesthetic agent and the adrenaline to take effect. The duration of action of lidocaine is approximately 45 to 60 minutes, whereas that of bupivacaine is approximately 2 to 3 hours. The amount of local anesthetic agent used in relation to the age and body weight of the patient should be noted and care taken not to exceed safe levels, particularly in children. The anesthetic agent should be warmed before use to reduce the pain associated with its injection.
Subcutaneous injections in the eyelid should be placed just beneath the skin, avoiding injection into the orbicularis muscle. This reduces the risk of causing a hematoma, which can distort the tissue planes and cause a mechanical ptosis in the upper eyelid, making ptosis surgery more difficult to perform. The volume used in the eyelids should rarely exceed 1 mL per eyelid for most procedures. A 25-gauge, 24-mm needle is used to avoid the need for multiple injections, which further predispose to bleeding and hematoma. If only a small central area of the eyelid needs to be injected, it is preferable to use a 30-gauge needle. Injections into the eyelid should be performed from the temporal side of the patient, with the needle parallel to and not toward the eyelid. This reduces the risk of perforation of the globe in the event of sudden inadvertent movement of the patient. Immediate pressure and massage should be applied over the injection site for 5 minutes.
Additional local anesthetic agent should be kept available in a sterile syringe on the scrub nurse’s cart in case it is required during the surgical procedure.
The use of subconjunctival injections is preferable for some procedures, such as a posterior approach Müller’s muscle resection, because this minimizes the risk of an upper lid hematoma, but great care must be taken to protect the eye during the course of such injections.
1.6.3 Local Anesthesia with Sedation
Many oculoplastic procedures can be safely and satisfactorily performed with the use of a combination of local anesthesia and neuroleptic sedation. An anesthetist can provide safe conscious sedation and monitoring and management, if required, of a variety of medical conditions (e.g., hypertension, arrhythmias) while providing safe intravenous sedation, which can be titrated to the individual patient’s requirements and rapidly reversed. The agent most commonly used for this purpose is propofol. This drug is ideal for an anxious adult patient who requires a levator aponeurosis advancement or a Müller’s muscle resection. The patient is sedated during the administration of the injections but is fully cooperative during the intraoperative assessment and adjustment of the eyelid height and contour. For a more invasive, potentially painful procedure in an elderly patient, such as an enucleation, midazolam and an opiate can be used in addition (e.g., remifentanil, a potent ultra-short-acting synthetic opioid analgesic drug). The agents selected by the anesthetist should take into consideration whether the patient is undergoing the procedure on an outpatient or an inpatient basis.
Great care must be taken when administering periocular local anesthetic injections to a sedated patient. Such a patient may lose all inhibitions and become aggressive during a painful injection. This should be anticipated and assistance sought to prevent the patient from moving or raising his or her hands toward the face. This is particularly important in younger, strong patients. For such patients only light sedation should be used. In addition, the operating team and the anesthetist should be fully aware of the risk posed by the sternutatory (sneeze) reflex. This reflex affects a large proportion of patients sedated with midazolam and propofol. The reflex is suppressed by deep sedation and by the additional administration of an opiate such as remifentanil. The reflex may occur without warning and poses a risk during the administration of local anesthesia around the eye.
Key Point
Safe conscious sedation for oculoplastic procedures requires skill and experience on the part of the anesthetist and a good understanding of the procedure to be performed and the surgeon’s requirements. Intravenous sedation should be used with great caution during lacrimal drainage surgery, because the airway may not be adequately protected from the effects of bleeding or the use of irrigation fluid.
1.6.4 Regional Anesthesia
Regional nerve blocks are useful to supplement the effects of subcutaneous injections for a limited number of surgical procedures under local anesthesia. An infratrochlear block can be combined with local tissue infiltration and intranasal cocaine for an external DCR. A peribulbar injection of 0.5% bupivacaine with 1:200,000 units of adrenaline mixed with hyaluronidase is ideal for an enucleation or evisceration procedure. Regional nerve blocks targeting the supraorbital, supratrochlear, infratrochlear, infraorbital, zygomaticofacial, zygomaticotemporal, and lacrimal nerves in addition to such a peribulbar injection, in combination with safe intravenous sedation, can permit an orbital exenteration to be performed on a conscious patient who is unfit for general anesthesia.
1.6.5 General Anesthesia
General anesthesia is required for children and uncooperative patients and is indicated for longer and more extensive surgical procedures, such as a lateral orbitotomy. It is also required to protect the airway of patients undergoing procedures that are likely to result in bleeding from the nose or mouth. The patient’s general health will determine the suitability of the patient for general anesthesia. A patient with a history of general medical disorders who is to undergo elective surgery should be identified to the anesthetist at the preassessment clinic.
Bupivacaine injections containing adrenaline (1:200,000 units) are used in combination with general anesthesia to assist hemostasis and to provide immediate postoperative pain relief. The use of such injections in combination with hyaluronidase before enucleation or evisceration surgery can be very effective in blocking the effects of the oculocardiac reflex. The anesthetist should be made aware of the potential for such a reflex, which can cause severe bradycardia and, rarely, asystole.
1.7 Surgical Instrumentation
The variety of delicate surgical instruments used in ophthalmic plastic surgery attests to the special demands of surgery in this region.
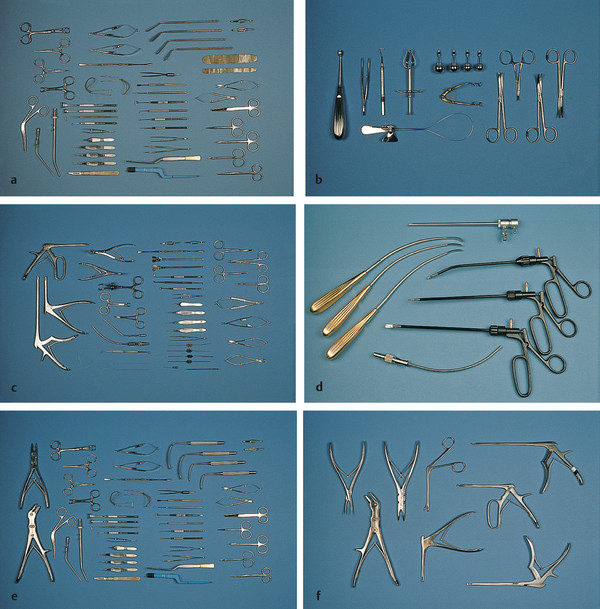
A basic ophthalmic plastic surgery instrument set should be available for oculoplastic cases (Fig. 1‑1a). Separate instrument sets should be available for enucleation and evisceration (Fig. 1‑1b), external DCR (Fig. 1‑1c), endoscopic DCR and endoscopic browlift surgery (Fig. 1‑1d), and orbital surgery (Fig. 1‑1e). A variety of accessory instruments should be readily available (Fig. 1‑1f). These instruments must be kept in good repair and should be respected and used appropriately. Alternatively, consideration can be given to the use of disposable instruments that are now of very good quality. Inappropriate use of instruments can result in damage to delicate instruments and damage to tissues. The nurse assistant should ensure that dried blood, tissue, and char are carefully removed from the instruments as they are handed back during the course of surgery. The surgeon should ensure that the instruments are carefully handed to the nurse assistant to prevent injury from sharp blades and needles.
Key Point
The surgeon should ensure that instruments are never passed across the patient’s face.
A number of basic principles apply to the use of ophthalmic instruments. Toothed forceps or skin hooks should be used to avoid crushing and damaging tissue. A variety of forceps of varying size are available and should be selected according to the type of tissue to be handled. The most commonly used toothed forceps to assist with dissection of the eyelids are Paufique forceps. The 0.12 Castroviejo forceps are ideal for the handling of delicate eyelid skin when suturing. Skin hooks must be handled with great care to prevent inadvertent injury to the globe. The eyelid skin is very delicate, and it is preferable to hold and lift the underlying orbicularis muscle, and not the skin, to dissect underlying tissue planes. Adson forceps are more robust and are used for handling the cheek, lower face, and scalp tissues.
A variety of scissors may be used during surgery. These may be curved, straight, sharp, or blunt-tipped. Curved, blunt-tipped Westcott scissors are used for the dissection of tissue planes in eyelid surgery and conjunctival surgery. They should not be used to blunt-dissect tissue planes. Stevens tenotomy scissors are more appropriate for this purpose and for the dissection of thicker tissue, such as a glabellar flap. Straight iris scissors are used for eyelid wedge resections. Straight Stallard scissors should be used for the removal of skin in a lower lid blepharoplasty.
Gross separation of tissue planes should be accomplished with blunt-tipped Stevens tenotomy scissors, which minimize the risk of bleeding; for example, they are used to blunt dissect Tenon’s fascia from the globe in an enucleation and the orbicularis muscle in an external DCR. Sharp-tipped iris scissors are used for performing eyelid wedge resections. Small suture scissors should be used for cutting sutures.
A Colorado or short Megadyne needle is an efficient instrument for the precise, delicate, and bloodless dissection of tissue planes in the eyelids. An earthing plate must first be attached to the patient, and care must be taken to ensure that the patient has removed all metallic objects from their clothing. The needle has both cutting and monopolar coagulation modes. It is used in conjunction with a Valleylab diathermy machine (Fig. 1‑2). I use this instrument ubiquitously in my practice for making skin crease incisions, subciliary incisions, and transconjunctival incisions in addition to general eyelid dissections (e.g., to perform blepharoplasties or to expose the levator aponeurosis and the inferior orbital margin). Alternatively, it can be used for soft tissue dissection in the eyelids after making the initial skin incision with a No. 15 Bard Parker blade. Its use requires a dry surgical field. The tissues to be dissected should be held under some tension. The tip of the needle should be moved constantly across the tissue to be dissected when the instrument is activated to avoid burning the tissues and should be used with a delicate stroking motion without applying pressure to the tissues.

Artery clips are used routinely to fix traction sutures and Jaffe retractor bands to the surgical drapes. Curved clips that lie flat against the surface of the drapes are preferable to straight clips. To fix the suture or bands, one limb of the clips should lie beneath a fold of the drapes before the clips are closed.
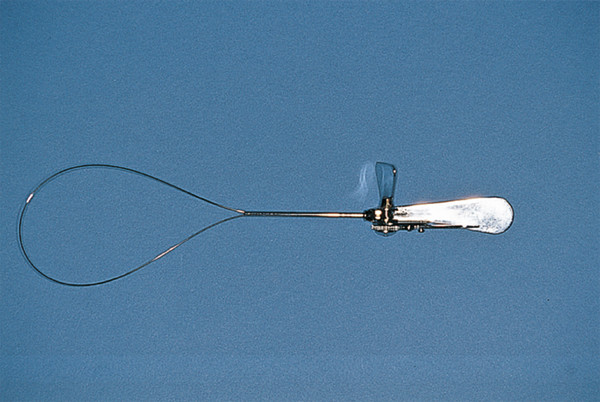
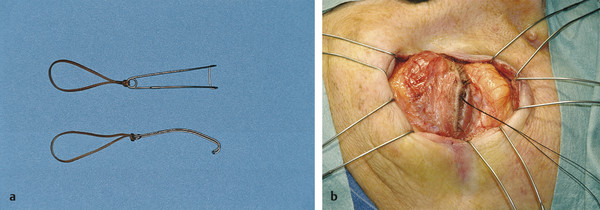
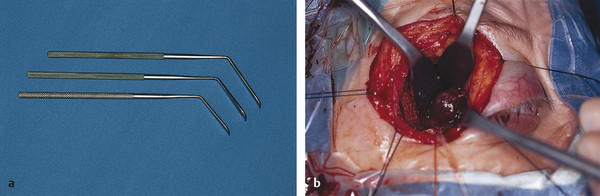
Enucleation scissors in a variety of curvatures and sizes should be available and used whenever the use of a snare is inappropriate, such as where a long piece of optic nerve is required, in the presence of a soft globe, a previous corneal section, or a penetrating keratoplasty. A snare may transect the posterior aspect of a soft globe and can cause a globe weakened by previous surgery to rupture, causing intraocular fluid to spray out under pressure. A snare is otherwise very useful for enucleation surgery, and its use is associated with minimal bleeding (Fig. 1‑3).
Spring-handle needle holders are available in a variety of sizes and may be curved or straight. These are excellent for use in oculoplastic surgery. These are selected according to the size of needle to be used. Needle holders designed to hold small needles, such as a 7–0 Vicryl suture needle, will be damaged if used inappropriately to hold larger needles. The Castroviejo needle holders are preferred, because they have a simple locking mechanism that permits the needle to be loaded securely and held between suture passes. Ring-handle needle holders (e.g., the Webster needle holder) are used to hold suture needles larger than 4–0.
A variety of bone punches are available for bone removal, such as for an external DCR (Fig. 1‑1f). It is important that these are used appropriately. The delicate bone of the lacrimal fossa floor can be removed using a fine punch, such as a Hardy sella punch. This should then be replaced by progressively larger Kerrison rongeurs for the removal of the anterior lacrimal crest and nasal bone. The continued use of the delicate Hardy sella punch for the thicker bone will result in damage to this instrument.
1.8 Correct Surgical Site Marking and Allergy Check
It is the responsibility of the surgeon to ensure that he or she has seen the patient before surgery and has clearly marked the correct surgical site after carefully checking the patient’s consent form and the patient’s identification bracelet. As mentioned previously, when the patient arrives in the anesthetic room, the surgeon should pause. This pause before anesthesia and surgery, or time out, forces everyone to slow down for a few moments and double check what they are about to do.
The surgeon should follow the hospital’s agreed protocol to ensure that the correct patient has arrived; that every member of the surgical team agrees that the correct operation is to be performed on the correct side; that the appropriate scans are available; and that all required surgical equipment, implants, and disposables are available. In addition, where appropriate, the availability of cross-matched blood should be checked and the availability of a pathologist confirmed whenever a frozen section is required. A checklist should be completed and signed.
The surgeon should check the patient’s allergy history before giving any injections and before prepping the patient. The surgeon should also inform the anesthetist before the administration of any injections. The surgeon should always prep and drape the patient himself or herself and should not allow himself or herself to be distracted during this very important process.
The surgeon should also ensure that all members of the surgical team are wearing eye protection prior to the commencement of surgery and that suction is available for the evacuation of surgical smoke.
Key Point
The surgeon should ensure that “time out” is called before the commencement of anesthesia and surgery.
1.9 Preparation and Draping of the Patient
If local anesthesia with or without sedation is used, the whole of the patient’s face should be cleaned with povidone-iodine solution diluted 50:50 with sterile water or saline, starting with the eyelids and moving outward. If the patient is allergic to povidone or iodine, aqueous chlorhexidine can be used instead. The face should then be dried. If general anesthesia is used, the area to be operated on should be cleaned, but both eyes should be left exposed if there is a need to check the symmetry of the globe positions. Additional areas may need to be cleaned, such as the postauricular area or the upper inner arm if a skin graft is required. The eyes should be instilled with a preservative-free lubricant ointment. The drapes should be applied by the surgeon in a manner that ensures no restriction on the movement of a local tissue flap or pressure on the eyebrow when undertaking a ptosis procedure.
1.10 Surgical Incision and Exposure
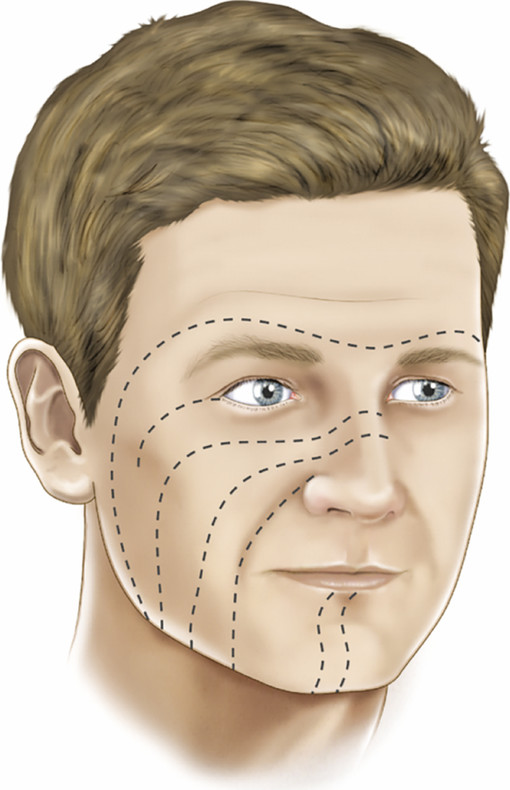
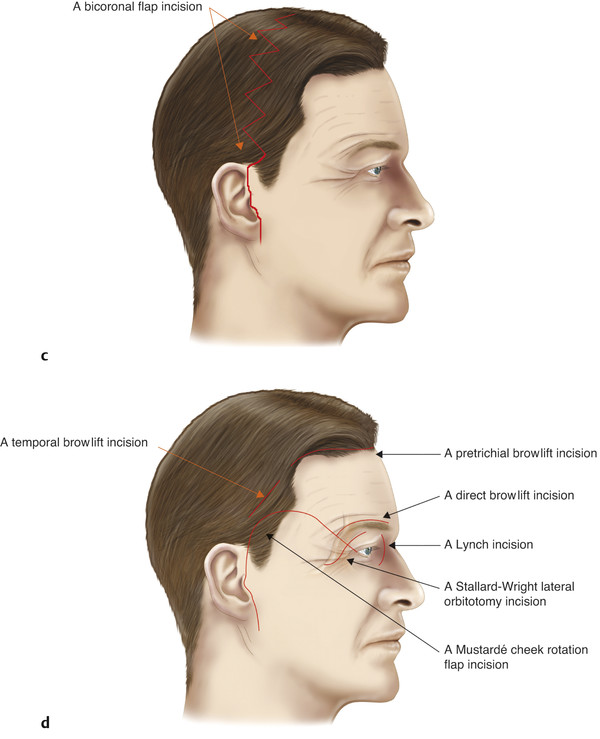
Incisions should be planned preoperatively to provide adequate surgical access and yet result in a minimally conspicuous scar. Wherever possible, skin incisions should be planned to follow the relaxed skin tension lines (RSTL). These lines lie within normal skin creases or folds, enabling incisions to be hidden or disguised (Fig. 1‑4). The lines correspond to the directional pull existing in relaxed skin; this is determined by the underlying structures and the depth of subcutaneous tissue and fat. Incisions that run parallel to the RSTL tend to remain narrow after wound closure, unlike those running perpendicular to them, which are more likely to gape.
Incisions that interrupt lymphatic drainage (e.g., incisions directly over the infraorbital margin) should be avoided, because they can lead to persistent postoperative lymphedema.
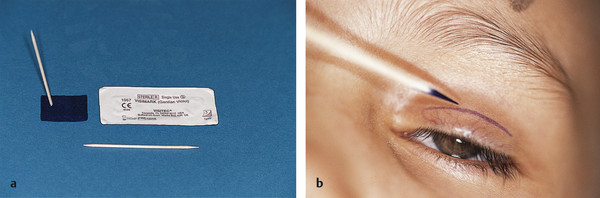
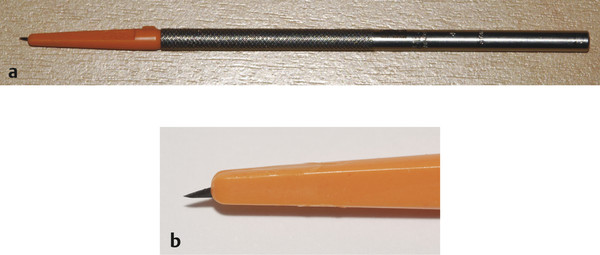
Skin incisions should be marked before the injection of the local anesthetic agent, which may obscure anatomical landmarks such as the upper eyelid skin crease. Marking is best achieved with a cocktail stick inserted into a gentian violet marker block (Fig. 1‑5a). This results in a fine line (Fig. 1‑5b). Grease on the skin surface should first be removed with a small alcohol wipe so that the marks are not inadvertently lost when the face is prepped with povidone-iodine solution.
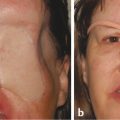
For very young patients or patients who are prone to hypertrophic or keloid scar formation (Fig. 1‑6), skin incisions may be avoided for certain procedures. For example, a DCR may be performed endoscopically and an orbital floor blowout fracture may be approached via a conjunctival incision.

Skin incisions which are commonly used in ophthalmic plastic surgery are shown in Fig. 1‑7. The Stallard Wright lateral orbitotomy incision is used for older patients, but for younger patients an upper lid skin crease incision is used instead, and the incision carried into a “laughter” line at the lateral canthus.

Skin incisions should be made perpendicular to the skin surface, except in the eyebrow region or scalp, where the incision should be beveled. For eyelid skin incisions, the Colorado needle is a very effective alternative to the use of a No. 15 Bard Parker blade. It results in less bleeding and permits a layer-by-layer dissection of the tissues, allowing identification of blood vessels that can be cauterized before they are cut.
When making a skin incision with either a blade or the Colorado needle, the incision should be made with a continuous motion to avoid jagged wound edges. The skin should be held taut. Skin incisions in the eyelids are aided by the use of 4–0 silk traction sutures placed through the gray line. A 4–0 black silk suture on a reverse-cutting needle is passed into the gray line of the eyelid and the curvature of the needle followed until the needle emerges from the gray line again. The delicate eyelid skin should be held with fine-toothed forceps, such as Bishop Harmon forceps. Skin hooks should be used with great care in the periocular region because of the risk of inadvertent injury to the globe.
Incisions along the gray line of the eyelids, such as a gray line split into the upper eyelid as part of an upper eyelid entropion procedure, or in both eyelids as part of a tarsorrhaphy procedure, should be made with a Beaver microsharp blade (7530) on a Beaver blade handle (Fig. 1‑8).
Surgical exposure is aided by the use of a variety of retractors or by the use of traction sutures. In upper eyelid levator surgery or an orbital floor fracture repair, self-retaining Jaffe retractors enable the surgeon to operate without needing a surgical assistant, unlike with Desmarres retractors (Fig. 1‑9). Desmarres retractors are very useful and are available in different sizes. They are also used to evert the upper and lower eyelids in conjunction with a gray line traction suture for posterior-approach surgery, such as a posterior approach Müller’s muscle resection. It is important to use the appropriate size of Desmarres retractor to evert the eyelid and avoid undue pressure being applied to the supraorbital margin by the retractor when everting the upper eyelid.
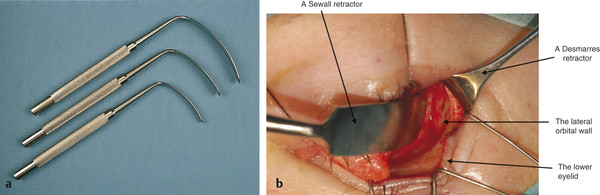
Sewall retractors (Fig. 1‑10) are used to retract the orbital contents during an orbital fracture repair, an orbital decompression, or an orbital exenteration. The blades are available in different sizes and should be selected appropriately. They can be used in conjunction with a piece of Supramid to improve the retraction of orbital fat during these procedures. Typically, these retractors are placed into the subperiosteal space. Great care, however, must be taken by the assistant when using these retractors, because extreme force can be applied to the globe. In addition, it is easy to “toe-in” the tip of the retractor and tear the periorbita. This can also lead to direct trauma to the optic nerve.
Wright retractors (Fig. 1‑11) are more delicate retractors that are used to retract tissues in the orbit during the course of the exploration of an orbital mass or during the course of an optic nerve sheath fenestration. Malleable retractors are mainly used to protect the orbital contents from the use of drills and saws. The use of retractors in orbital surgery is discussed in more detail in Chapters 19 to 20.
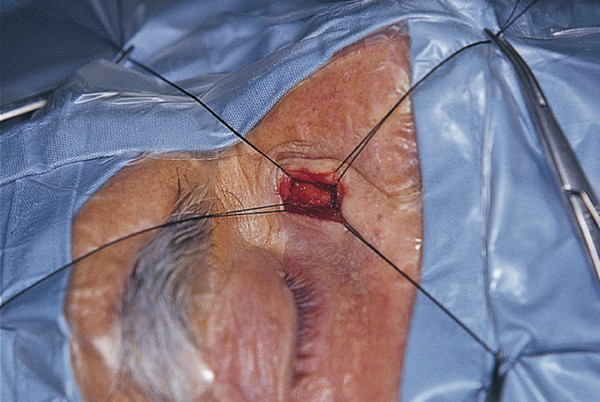
Traction sutures not only improve surgical exposure but also assist in hemostasis, such as in an external DCR (Fig. 1‑12).
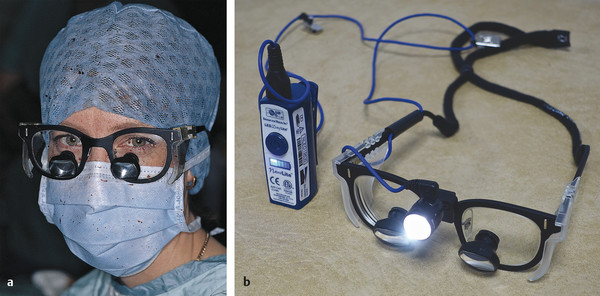
Safe surgical dissection is greatly facilitated by adequate magnification and illumination of the surgical field. The surgeon should wear surgical loupes, which do not unduly restrict the visual field. The loupes should be comfortable and should not require adjustment; typically, they provide 2.5 to 3.5 times magnification; they should be fitted with protective side shields (Fig. 1‑13a).
The use of a headlight offers a number of advantages over an overhead operating lamp. The light is always focused on the surgical field, which is not placed in shadow by the surgeon or assistant’s hands. The use of a headlight is essential in surgery within cavities, such as an external DCR or an orbital decompression. Modern lights can be fitted to the surgical loupes and turned on and off by the surgeon by a switch that is operated by the inside of the elbow and worn beneath the surgical gown (Fig. 1‑13b).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


