1 Fundamentals of Oncoplastic Breast Surgery
One of the main measures of successful breast cancer surgery is local control. It has been demonstrated that undertreatment followed by local failure is deleterious in some subgroups of patients. This knowledge has led to a shift in the treatment strategy for patients with breast cancer. Rather than rely on systemic interventions in response to inadequate surgical approaches, surgeons now place greater emphasis on meticulous planning and skilled execution combined with radiotherapy to minimize local relapse while maintaining cosmesis. 1 Oncoplastic surgery effectively accomplishes this goal by incorporating partial resection with immediate reconstruction. Today oncoplastic surgery is primarily performed to cope with unfavorable anatomy, relative tumor size and location, to challenge complex local treatments and postradiation breast surgery, and to remove the cancer without mutilation and with the tumor not touching ink for invasive disease and with at least 10 mm in ductal intraepithelial neoplasia (DIN). Oncoplastic surgery was not invented to extend unnecessary margins but to reduce reexcisions, recalls for distortion after prior breast-conserving surgery (BCS), and to lower the rate of mastectomies thus saving social and medical resources. 2
Origin of Oncoplastic Surgery
The term oncoplastic surgery was introduced in 1993 3 and published a year later. 4 It encompasses unique approaches suggested by different surgeons and focuses on tumor resection and breast aesthetics through partial breast reconstruction techniques that minimize potential breast deformities.
The initial focus of oncoplastic surgery was on breast deformities after quadrantectomy, 5 , 6 and it became another alternative to consider during the initial surgical planning and decision-making process.
The oncoplastic surgical approach allowed surgeons to tailor techniques to prevent deformities, minimize margins, and reduce potential for local recurrence.
Terms such as cosmetic quadrantectomy, 7 aesthetic diagnostic round-block technique, 8 low pole tumor reduction mammaplasty, 9 and central tumor reduction 10 define the basic principles that formed the roots of oncoplastic surgery. These techniques bridge the gap between resection and immediate reconstruction to save form and function, which are integral parts of the body image. Independent from its linguistic roots, the term oncoplastic is a distinctive label for tumor-specific immediate reconstruction. The term tumor-specific immediate reconstruction (TSIR) was introduced by John Bostwick III in 1996. 11 This concept covers the complete spectrum of available techniques, from partial to total immediate breast reconstruction (IBR).
TSIR represented a decisive stage in the evolution of oncoplastic breast cancer surgery; it includes delayed procedures, total reconstruction, and salvage procedures. The oncoplastic concept implies not only the reconstruction of partial defects, but also the planning of resection in cosmetic units, if possible, to provide the most natural-appearing, aesthetic breast. These two terms, TSIR and oncoplastic, are similar in meaning; however, the oncoplastic approach also includes delayed and salvage procedures. Regardless of the terminology used, partial breast reconstruction has been a valuable addition to the management of women and men with breast cancer. Initially, the benefits were evident in Europe, where the techniques were used to treat quadrantectomy-type defects. More recently, the techniques have become common in the United States for lumpectomy defects.
Today, on a worldwide basis, oncoplastic surgery does not interfere with treatment protocols and is oncologically based on the Milan I trial. In addition, it has enabled breast cancer patients to have fewer fears about disfigurement. 12
Anatomic Classification
The anatomic classification for the oncoplastic approach to partial mastectomy defects should include planning for a potential completion mastectomy.
The wider the excision, depending on the type of tumor, 13 the lower the risk of local failures potentially contributing to compromised cosmesis. To this end, two options have emerged: (1) partial reconstruction and (2) skin-sparing mastectomy (SSM) with reconstruction. 14
The main factors that influence the approach to treating the deformity are:
The location of the tumor (such as in the cleavage)
The tumor/breast ratio
The surgical resection (which may lead to nipple-areola distortion, retraction, and volume/size asymmetry)
Radiotherapy (which may lead to skin effects, color differences, shrinkage, and fat necrosis)
A smaller tumor/breast ratio should yield better cosmetic results; however, similar ratios might yield different results, depending on the tumor location.
Any anatomic classification of breast tumors for an oncoplastic approach to partial mastectomy defects should include the location, size, shape, symmetry, tumor/breast ratio, and NAC.
Box 1-1 Anatomic Classification of Breast Tumors Sites of Tumors and What They Affect
Upper outer quadrant—affects the lateral flow
Lower outer quadrant—affects the lateral flow
Central or borderline—retracts the nipple-areola complex
Upper inner quadrant—affects the cleavage
Lower inner quadrant—affects the crease
Superior pole—distorts upper pole fullness
Tumor/Breast Ratio
Lower is favorable
Higher is unfavorable
Nipple-Areola Complex
Central/subareolar, raising nipple-areola loss or retraction.
Noncentral/borderline of the breast quadrants, raising deep margin problems; these relate to the difficulties of deep clear margin resection, because the thin breast layer in the borderline of the breast makes achieving sufficient clearance in the third dimension, close to the muscle, difficult.
Avoiding Asymmetry
The most favorable anatomic situation for a partial mastectomy is asymmetry, especially when the affected breast is larger. The aim of avoiding asymmetry as a result of quadrantectomy was expressed in Veronesi’s definition referring to quadrantectomy as a “bilateral approach,” such as the “mirror” technique that was performed in the 1970s and 1980s as a way of balancing the volume of resection and the NAC position. 15 The latter technique contributed to recentralization techniques, introduced by Petit and Rietjens. 16 Oncoplastic planning often includes similar resections on the opposite side, such as a mirror biopsy, to improve symmetry. One approach is to perform the contralateral procedure after radiotherapy to allow edema and any breast fibrosis time to resolve.
Training Oncoplastic Surgeons
Specialized training is an often-debated issue. The concept of a specialized breast surgeon on a European, American, or worldwide level is important, because breast cancer is a silent epidemic. It is estimated that 1.152 million women will be diagnosed with breast cancer in the coming year. Of these, 411,000 will die of tumor-specific causes. It is also estimated that 20.6 million survivors have been treated for breast cancer. 17 Breast centers and specialized breast surgeons are required to have proper accreditation. This ensures that patients are offered the best treatments possible, but it also offers trainees a solid aim for their fellowship, which includes curriculum as well as accreditation. The leading surgeons in this field are the individuals driving this specialty forward—they have established guidelines for training breast cancer specialists, including breast surgeons, 18 and have created and published a good practice guide 19 ; these resources exemplify the current level of quality of the curriculum in our daily practice. In Europe, the entry requirement of candidates for training and accreditation in breast surgery is to be currently licensed to practice as a general surgeon, plastic surgeon, or gynecologist. The training facility is based at a certified breast center consisting of integrated departments of senology (surgical breast oncology) and plastic surgery, including microsurgery.
The training facility should provide training options for physicians to acquire sufficient skills and practice to establish breast centers of excellence. Training options should include oncologic surgery, plastic and aesthetic surgery, principles of oncoplastic surgery, radiology, nuclear medicine, pathology, systemic therapy, radiotherapy, and others. Training options in the United States and other countries may vary; however, the ultimate goals are the same. These are detailed more extensively in Chapter 2.
Technical Insights
The following section highlights some of the oncoplastic techniques that are thoroughly detailed in other chapters. Terms that are common to oncoplastic breast surgery are also introduced. In short, this section demonstrates the depth, complexity, and constant evolution of the oncoplastic approach.
Cosmetic Quadrantectomy
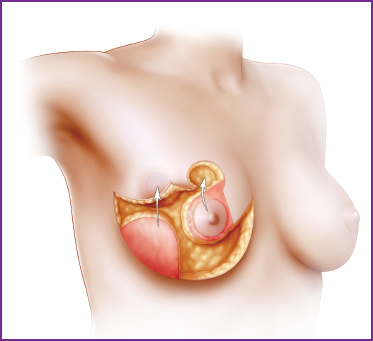
Cosmetic quadrantectomy is one form of resection in which the aesthetic subunits of the breast are carefully considered. The goal is to perform the resection in a way that preserves a natural shape, depending on the patient’s body image. The skin “pouch” technique (A), with its resultant shrinking of the skin (B), is one way to accomplish this.
Surgical Sequence
Needle framing (to localize the extent or center of the tumor by ultrasound-guided needle localization in a 90-degree angle)
Composite resection/ductectomy/quadrantectomy
Margin and papilla biopsy
Full-thickness defect closure with nipple-areola recentralization
Patient Examples
Local Flap Reconstruction (Matrix Rotation)
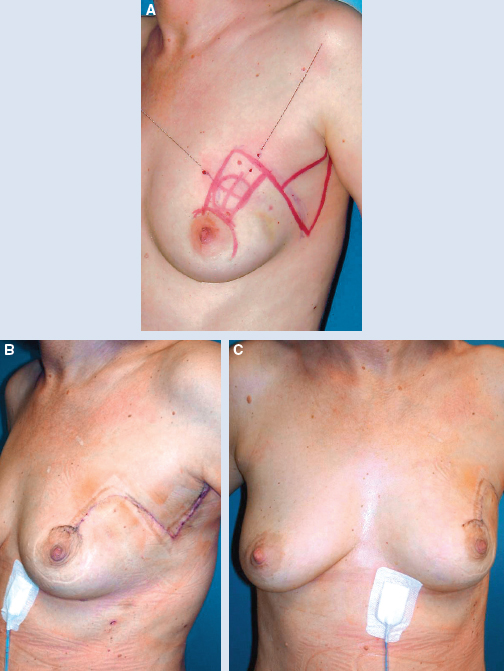
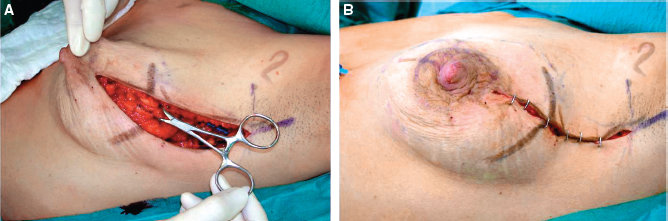
This patient had BCT with matrix rotation of the outer quadrant. She is shown both preoperatively (A) and 2 days postoperatively (B and C).
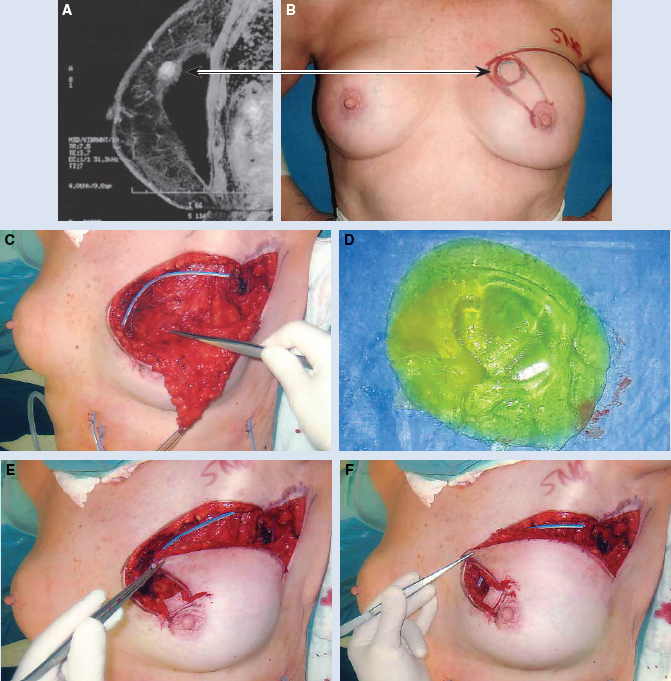
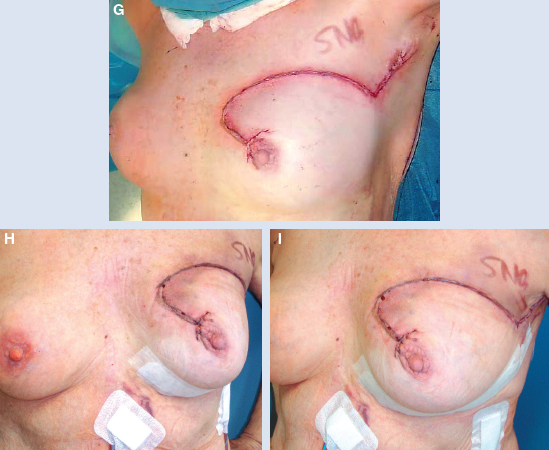
This MRI shows a submuscular implant (A), and the clinical view of the prepectoral cancer in the upper inner quadrant on the left side (B). The sector resection included the muscle stripe and the removed implant (C and D). The new implant had complete muscle coverage. The lateral breast matrix and skin were rotated into the defect (E and F).
The patient had safe coverage, with immediate partial reconstruction (G through I). This example demonstrates the advantage of oncoplastic surgery with an implant.
Local flaps are a useful option for reconstructing defects in the upper inner quadrant, which is often called no-man’s land. 10 Breast tissue and skin are rotated to fill in the defect.
Surgical Sequence
Needle framing
Axilla triangle
Parallel sector resection
Margin and papilla biopsy
Nipple-areola complex shifting
Matrix rotation
Related posts:
 2 Current Approach to Oncoplastic Breast Surgery
3 How to Incorporate Oncoplastic Surgery Into Your Practice
14 Psychosocial Aspects of Oncoplastic Breast Conservation
2 Current Approach to Oncoplastic Breast Surgery
3 How to Incorporate Oncoplastic Surgery Into Your Practice
14 Psychosocial Aspects of Oncoplastic Breast Conservation
 17 Central Defect Reconstruction
17 Central Defect Reconstruction
 26 Correction of the Breast-Conserving Therapy Deformity Using Local Flaps
26 Correction of the Breast-Conserving Therapy Deformity Using Local Flaps
 34 Outcomes and Tumor Recurrence After Oncoplastic Surgery of the Breast: Eighteen-Year Follow-up
34 Outcomes and Tumor Recurrence After Oncoplastic Surgery of the Breast: Eighteen-Year Follow-up
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


