1 Extensor Tendon Repair (Zone 1, 3, 5)
Abstract
Extensor tendon injuries are more common than flexor tendon injuries and require similar precision in diagnosis and treatment. Closed injuries without an open injury can be treated with splints or casts, whereas those resulting from an open injury (e.g., laceration) should be treated with an open repair. In addition, chronic injuries, or those involving significant bony avulsions, often require surgical intervention. Soft tissue mallet injuries may have similar outcomes following splinting in either acute or chronic phase. Central slip injuries must be monitored closely to prevent development of a Boutonnière deformity. For zone 5 “fight bite” injuries, tendon repair should be delayed until any infection is cleared. Postoperative therapy for zones 1 and 3 injuries should focus on immobilization. However, isolated zone 5 injuries may benefit from early gliding with relative motion splinting.
1.1 Key Principles
Extensor tendons are thinner and flatter than flexor tendons, and are therefore less likely to hold core sutures. Repair methods should focus on maximizing strength while minimizing shortening. As such, mattress or figure-of-eight-type sutures may be better suited for repair. Given the frequency of contamination, absorbable suture material with a prolonged degradation time such as polydioxanone (up to 6 weeks) should be considered in lieu of permanent sutures that may harbor prolonged bacterial colonization or represent a nidus for breakdown or pain in the thin dorsal skin envelope.
The extensor mechanism is largely extrasynovial and any instrumentation can cause potential scarring to skin and bone. In the setting of an associated fracture, periosteal stripping can cause dense adherence of the extensor tendon to the underlying cortical bone. This should be considered when choosing techniques of osteosynthesis to allow for early mobilization and gliding of the tendon.
Extensor tendon injuries are often associated with damage to neighboring structures, such as metacarpophalangeal (MCP) joint penetration in the setting of “fight bite” injuries in zone 5, or germinal matrix and physeal injuries in zone 1.
1.2 Anatomy
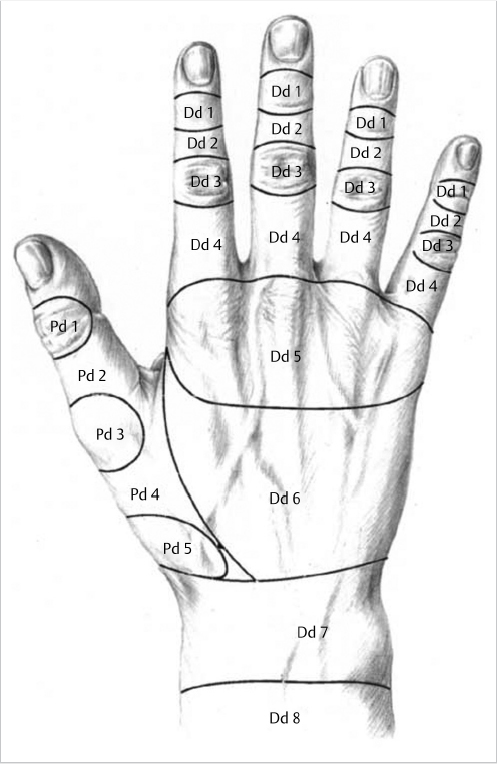
Extensor tendon injuries are classified by zones, with “odd” number designations occurring over joints (► Fig. 1.1). So, zone 1 injuries are over the distal interphalangeal (DIP) joint and represent disruption of the terminal extensor, zone 3 are at the level of the proximal interphalangeal (PIP) joint with an injury to the central slip, and zone 5 designate injuries at the MCP joint. It should be noted that zone 5 injuries, in addition to disruption of the joint or metacarpal head, may include sagittal hood and sagittal band injuries, resulting in subluxation of the extensor tendon into the intermetacarpal recess.
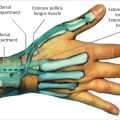
The extensor mechanism of the digits is governed by two separate and neurologically independent systems. The radial nerves innervate the extrinsic extensors (extensor digitorum communis [EDC], extensor indicis proprius [EIP], and extensor digiti minimi [EDM]) and the ulnar and median nerves innervate the intrinsic extensors (lumbricals, interossei). The extrinsic extensors originate in the proximal forearm and are responsible for MCP joint extension.
Within the intrinsic system, the lumbricals originate on the flexor digitorum profundus (FDP) tendon, though the third and fourth lumbricals may have an accessory head on the ulnar side of the neighboring flexor tendon. The interossei originate on the metacarpal and attach to the extensor mechanism at the level of the proximal phalanx. Given the volar position of the intrinsic extensor, relative to the axis of rotation of the MCP joint, they are responsible for MCP joint flexion and IP joint extension.
1.3 Repair Indications and Contraindications
Generally, the indications of closed or open treatment of extensor tendon injuries in the fingers depend on whether the disruption is due to a closed or open (wound) injury. Closed injuries without an open injury can be treated with splints or casts, whereas those resulting from an open injury (e.g., laceration) should be treated with an open repair. In addition, chronic injuries, even when closed, often require surgical intervention. Open injuries, chronic extensor deficiencies, or complex traumas typically warrant operative intervention.
Active infection, loss of dorsal soft tissue coverage, or chronic injuries with joint stiffness or ankylosis may represent relative contraindications to operative repair.
1.4 Anesthesia
Extensor injuries in zones 1 and 3 can be repaired under digital block, while a wrist block may be needed for zone 5. However, general anesthesia may be required in some patients, especially pediatrics, to allow appropriate exploration and irrigation of the wound. Wide awake local anesthesia using a local anesthetic with epinephrine obviates the need for a tourniquet and is an increasingly popular and effective method for acute repairs.
1.5 Caveats, Pearls, and Lessons Learned (Extensor Zone 1, 3, 5)
1.5.1 Zone 1: Terminal Tendon Injuries (Mallet Finger)
Anatomy
The lateral bands are formed from contributions of the intrinsic muscles (lumbricals, interossei) and the EDC tendon. The two lateral bands come together just proximal to the DIP joint to form the terminal tendon that attaches onto the dorsal aspect of the distal phalanx. The action of the terminal tendon is to effect extension at the DIP joint, and a disruption of the tendonbone juncture leads to loss of active extension of the DIP joint. The finger then assumes a flexion position at the joint due to the unopposed pull of the flexor tendons.
Treatment
Most closed zone 1 tendon avulsions (i.e., soft tissue mallet) can be treated with extension splinting of the DIP joint. We recommend uninterrupted splinting for 6 weeks followed by gradual weaning of 2 additional weeks of nighttime splinting. It is important to avoid hyperextension of the DIP joint in the splint to prevent skin necrosis. For patients that present in a delayed fashion, it is still reasonable to offer splinting, with reports of chronic injuries up to 3 months demonstrating satisfactory outcomes.
Tendon avulsions with a fracture fragment (i.e., bony mallet) are also correctable with a splint. Joint subluxation may be present in injuries involving 50% or more of the joint surface, and in order to establish a congruent joint, surgical repair may be needed. In cases where a large articular fragment is involved but the joint is stable through range of motion, operative indications may be based upon function as opposed to the absolute presence of a fracture.
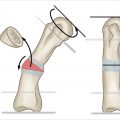
Closed reduction and percutaneous pining can be performed for delayed or open injuries. Mild hypertension of the DIP joint improves clinical joint reduction, which is visualized under fluoroscopy. A slight bend of the k-wire may help prevent migration or extrusion during the treatment period (► Fig. 1.2). Regardless of the repair technique, the patient should be counseled that a slight extension lag, swan neck deformity, or joint stiffness may persist.
Soft Tissue Mallet Repair
A soft tissue mallet may require operative treatment if open from a laceration or a crush injury, or for those that have failed conservative treatment with splinting. A recent systematic review demonstrated similar outcomes in either splinting or operative repair. Therefore, operative repair may be best suited for failed splinting or a secondary rupture. Several repair techniques have been reported, but we prefer the use of a small anchor placed at the dorsal ridge of the distal phalanx to avoid injury to the joint or germinal matrix. If desired, the repair can be augmented through dermatotenodesis, where the skin closure sutures include the underlying extensor tendon to encourage scarring of the two tissue planes. Following repair, a retrograde k-wire should be placed across the joint for 4 to 6 weeks to maximize tendon adherence.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


