1 Anatomy of the Breast
Structure of the Female Breast
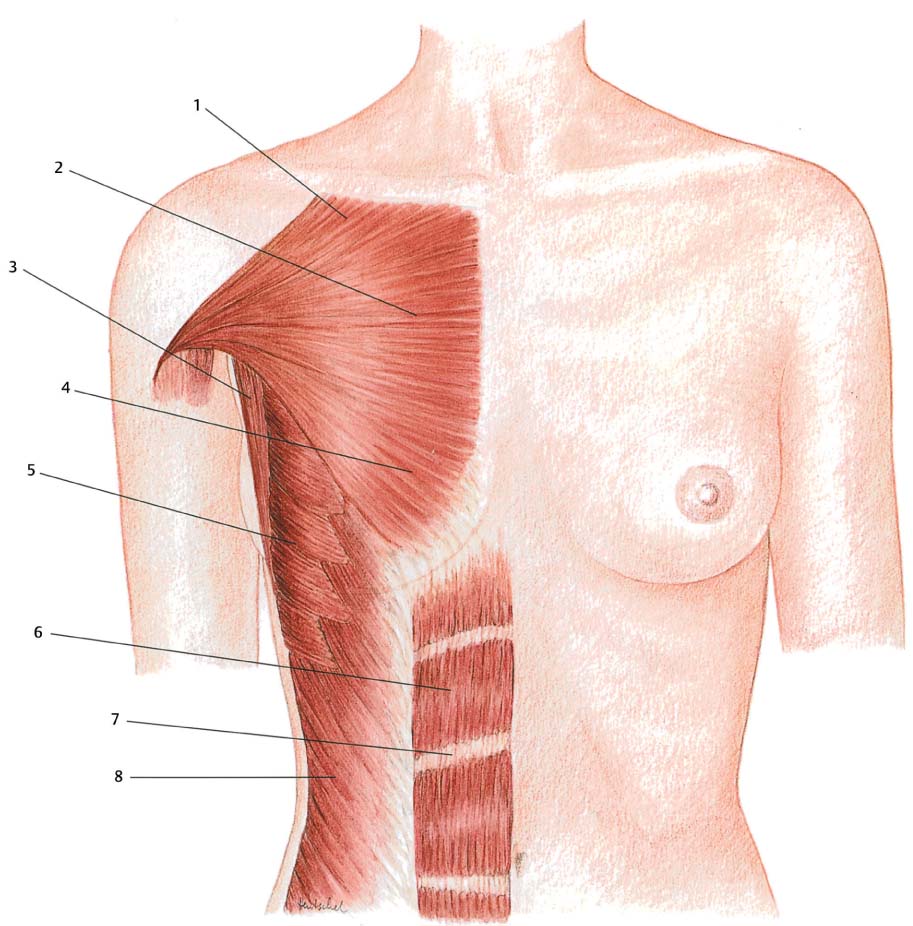
The female breast is roughly circular except at the upper outer quadrant, where the axillary tail of Spence extends to the axilla ( Fig.1.3 ). The functional portion of the breast is a modified cutaneous gland, an appendage of the skin. It is enclosed between the superficial and deep layers of the superficial fascia and extends from the sternocostal junction to the midaxillary line laterally, and to the third to the sixth ribs in the midclavicular line. In the elderly or in large breasts, the submammary fold may slide to the seventh rib. The upper two-thirds of the breast lie on the pectoralis major fascia and extend laterally to the serratus anterior muscle. The lower third lies on the external oblique muscle of the abdomen and the rectus abdominis muscle.
The lobule is the basic unit of the breast ( Fig.1.2 ). Each lobule contains 10–100 elongated terminal ducts called alveoli or acini. Ducts draining 20–40 lobules coalesce to form larger ducts and, ultimately, an excretory duct. A total of 15–20 lactiferous ducts drain the entire breast and dilate into the milk sinus beneath the areola.
The surrounding stroma consists of connective tissue, nerves, blood vessels, and lymphatic channels. Portions of the fibrous tissue of the breast parenchyma extend from the surface of the glandular breast anteriorly to the superficial layer of the superficial fascia (Cooper ligaments). Posterior ligaments suspend the breast to the deep layer and the pectoral fascia. Although the Cooper ligaments subdivide the parenchyma, there is no true surgical segmental breast architecture.
Because the Cooper ligaments are anchored in the skin, tethering of these ligaments by a small scirrhous carcinoma commonly produces a dimple or subtle deformity in the otherwise smooth surface of the breast.
With pregnancy, there is hyperplasia of the lobular units and diminution of the fibrous stroma. The normal size may be increased as much as two or three times. The nipple and areola become more prominent and more deeply pigmented. When lactation stops, the extralobular tissue involutes and the breast gradually returns to resting state. It does not return to the nulliparous form, however, and instead retains the mature shape.
Blood Supply
Three major arteries supply the breast with blood: the perforating branches of the internal thoracic artery, and the lateral thoracic and pectoral arteries ( Fig.1.2 ). The lateral perforating branches of the intercostal arteries and branches of the subscapular artery also contribute minor amounts to the blood supply.
The arterial supply to the medial and central breast stems from the perforating branches of the internal thoracic artery. These pass through the first through the fourth intercostal space just lateral to the sternum, penetrate the origin of the pectoralis muscle, and enter the medial edge of the breast, supplying more than 50 % of the blood to the organ.
The lateral thoracic artery, the second largest source of blood to the breast, arises from the axillary artery and courses down along the lateral border of the pectoralis minor muscle to reach the serratus anterior muscle. Its external mammary branches and the lateral perforating branches of the intercostal arteries supply the lateral breast.
The pectoral artery originates at the thoracoacromial artery, coursing down between the pectoralis major and minor. It supplies the posterior surface of the breast.
The perfusion of the nipple–areola complex is particularly important during surgery for aesthetic purposes. The blood supply to this complex arises medially and cranially from the internal thoracic and intercostal arteries.
The breast skin is mainly nourished by a subdermal plexus formed by perforators from the glandular tissue. The perfusion of skin flaps depends on the conservation of the subdermal plexus, the quality of the microcirculation, and the preservation of the major arterial supply at the base of the breast. The same is true for the central breast area with the nipple–areola complex.
The breast has a rich anastomosing network of superficial subcutaneous veins that mainly drain into the internal mammary vein. The drainage of the deep veins corresponds to the arterial blood supply.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


