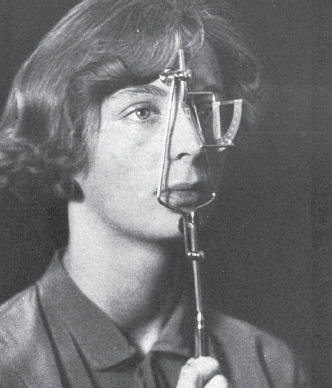
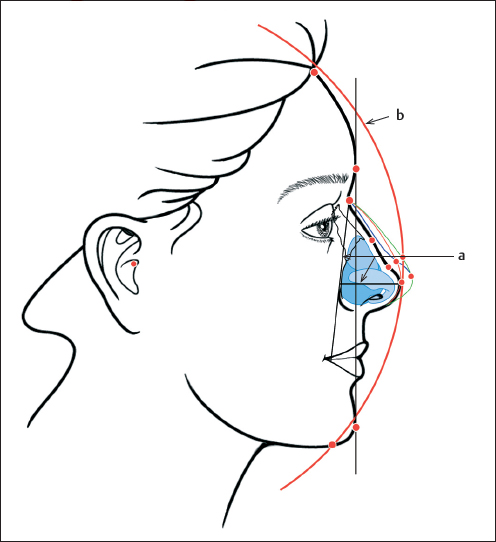
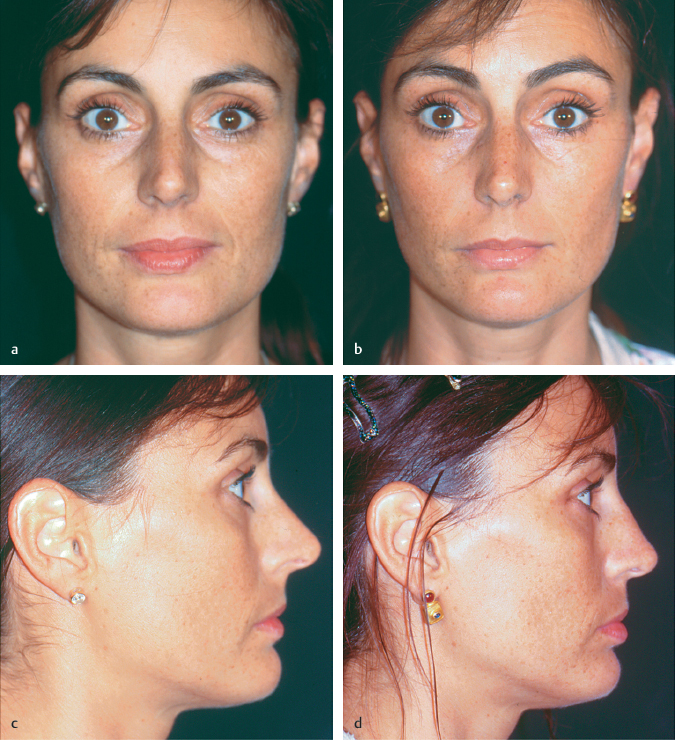
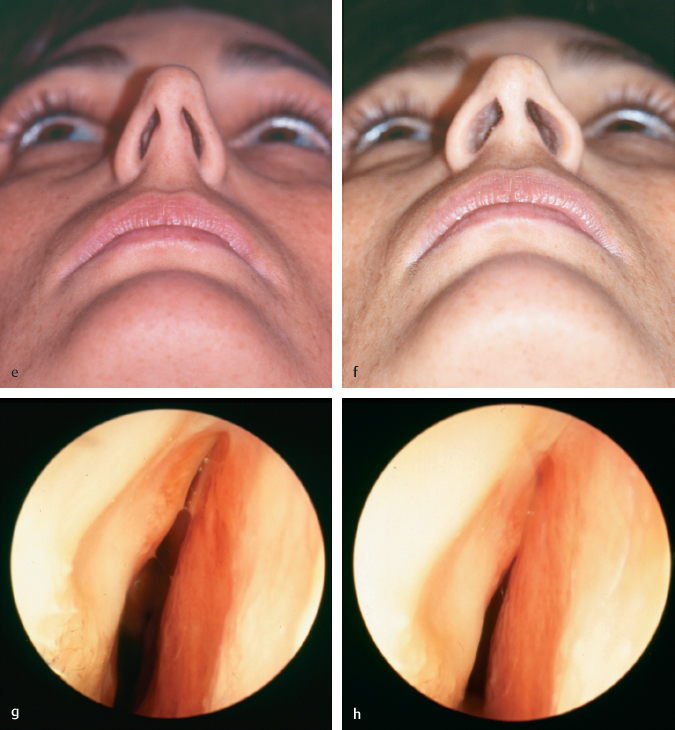
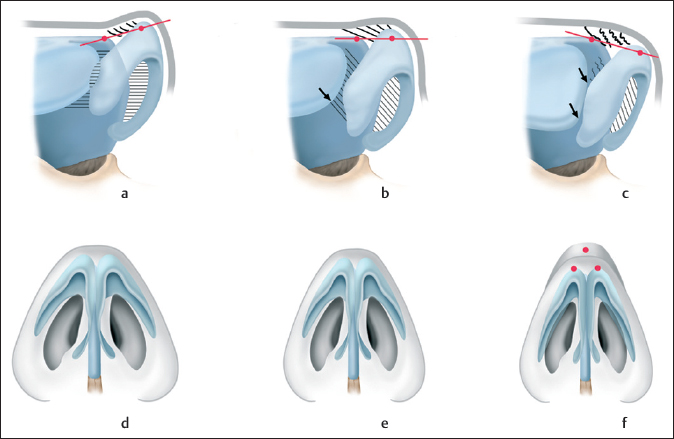
Chapter 11 The functional tension nose is characterized by an excess of anatomical components in the cartilaginous nose. The basic problem is excessive length of the septal cartilage in the basodorsal direction combined with hyperplasia of the upper lateral cartilages. Both septal and lateral cartilages develop embryologically from a common rudiment.1 It is common, therefore, to find combined hyperplasia that frequently affects the alar cartilages as well. This overgrowth leads to a general elevation of the nasal dorsum. The nasal pyramid is narrow and resembles a high, narrow, pointed gothic arch. Due to the firm attachments between the septum and upper lateral cartilages and the membranous attachment of the alar cartilages, the changes in the nasal dorsum are always accompanied by typical deformities of the nasal tip. This marks the difference between the functional tension nose and the humped nose, in which the dorsal hump is bony or cartilaginous in varying proportions. The shape of the nasal tip is usually unchanged. The hump in itself does not cause nasal airway problems, unless it is posttraumatic and associated with septal deviation. A pseudohump exists when the distance from the nasal tip to the facial plane is too small, causing the dorsum to move above the level of the nasal tip. The term tension nose always refers to a combined morphological and functional problem. Due to the excess cartilage, the functional tension nose is often disharmonious in relation to the face. It is too large and too high, i.e., overprojected. The nasal tip alone may be overprojected, independently of the overall size of the nose (Figs. 11.1a, b and 11.2a–d). Building on the tripod model of Anderson and its modification by McCollough and Mangat, Parell and Becker identified four key factors in the pathogenesis of the functional tension nose: excessive height of the septum, anteroinferior rotation of the tip, narrowing of the tip, and excessive length of the lateral crura of the alar cartilages.2–4 The functional tension nose also tethers the upper lip, causing abnormal exposure of the maxillary gingiva.5 Various surgical techniques have been described for relieving tension on the alar cartilages. These techniques focused mainly on the resection of the dome area,6 portions of the lateral crura,7 or the upper and lower alar cartilages.4 Bull stressed the importance of a hyperplastic anterior nasal spine in the overprojected nasal tip and recommended resecting the spine to retroposition the tip.8 Joseph used the profile angle as a measure of nasal projection. He defined it as the angle formed by the intersection of two straight lines: one line tangent to the glabella and chin, and a second line tangent to the nasal dorsum. He stated a normal range of 23 to 37 degrees. By measuring the angles in portraits painted by various famous artists (e.g., Holbein, da Vinci, Reynolds, Gainsborough), Joseph determined an average profile angle of 30 degrees9 (Fig. 11.3). Goode recommended the ratio of nasal length, measured as the distance between the nasion and pronasale, and projection measured between the alar groove and the pronasale for evaluating underprojection or overprojection of the nose and nasal tip. He defined the normal range as a ratio of 0.55 to 0.60.10 Baud described a method of profile analysis in which he drew a circle around the face with a radius from the external auditory canal to the pronasale (tip-defining point). He then checked the relationship between three key profile points (the pronasale, pogonium, and frontal hairline). Ideally, the three key points are located on the path of the circle (see Chapter 5). He used three sectors and sector angles to analyze the profile.11 Our own modification of this method is described in Chapter 5. In our experience, the facial circle should be centered on the lateral roof of the external auditory canal (the porion). We have had good experiences with a simplified and modified form of this method in routine situations, as it permits a rapid assessment of nasal projection in relation to the chin and forehead. The following questions can be answered: Fig. 11.1 Dorsal hump. (a) Before and (b) 3 years after septorhinoplasty. Fig. 11.3 Joseph developed a “profilometer” for directly measuring the profile angle, without the need for a lateral photograph. Digital image processing can be used, for example, to predict whether reducing the tip projection, causing a relative anterior displacement of the pogonion toward the circle, will provide sufficient improvement to the profile, or whether chin augmentation should be recommended12,13 (Fig. 11.4). The surgical treatment of the overprojected nose or functional tension nose has both functional and aesthetic indications. Both indications are based on the same morphological causes, and they are separated here purely for didactic reasons. The nares display typical changes: they are narrow, have a slit-like rather than oval shape, and terminate in a high “gothic” vestibule. The alar lateral crura and upper lateral cartilages are medialized, causing stenosis of the nasal valve. The nasal valve is formed by the junction of the free caudal margin of the upper lateral cartilage with the septal cartilage. The normal nasal valve opens at an angle of approximately 15 degrees. This angle is decreased in the functional tension nose, which in itself leads to obstructed nasal breathing. Forced inspiration causes the nasal valve to narrow and collapse, causing further airway obstruction (Fig. 11.5). Even a mild degree of high septal deviation in this situation will produce marked aerodynamic effects and exacerbate the nasal obstruction. Today, the term nasal valve (see Chapter 5) is distinguished from nasal valve area, which includes the membranous attachment to the free cranial margin of the alar cartilage and the functionally important head of the inferior turbinate. The functional tension nose is characterized by hyperplasia of the septal cartilage. Typically, the septal cartilage is too long in its dorsobasal dimension, elevating the upper lateral cartilages and cartilaginous nasal dorsum. The cartilaginous dorsum is typically convex or may form a hump, which blends proximally with a bony hump at the rhinion. The nasofrontal angle is reduced, depending on the size of the hump. Not infrequently, hyperplasia of the individual cartilages is also combined with increased longitudinal growth, creating the impression of a long nose. Functional tension nose is associated with typical changes in the supratip area, depending on the anatomical situation. The supratip point moves to the level of the tip-defining points, and tip definition is lost. Elastic fibers in the nasal tip area pass from the corium layer of the skin to the corium of the nasal vestibule.14 The skin in this area is relatively immobile. If the hyperplasia of the caudal septum can no longer be compensated by the elastic and collagen fibers of the skin over the nasal tip and the connective tissue fibers between the septum, alar cartilages, lateral cartilages, and membranous septum, then the tip-defining points will drop below the level of the supratip point (at the level of the anterior septal angle). This drooping of the tip is called ptosis. If we draw a straight line from the tip-defining point to the supratip point, we find that the angles of the nasal tip tangents are reversed when compared with the “ideal” nose. Although this discrepancy in the levels of the tip and supratip areas may be no more than 1 to 2 mm, it has a significant impact on nasal tip aesthetics (Figs. 11.5a–h and 11.6a–f). Fig. 11.5 Woman with functional tension nose and nasal valve stenosis. (a,b) Frontal views before and after surgery. (c,d) Lateral views before and after surgery. (e) Preoperative basal view. (f) Postoperative basal view after widening of the vestibule and nasal valve. (g) Preoperative right nasal valve during quiet respiration. (h) Preoperative right nasal valve during forced inspiration (0-degree endoscope, Karl Storz, Tuttlingen). Fig. 11.6 Stages of tension nose. (a) Normal nose. (b) Compensated tension nose. (c) Decompensated tension nose with a ptotic tip. (d) Normal position of the alar cartilages. (e) Tension nose with elongated nares and incipient obstruction of the nasal valve. (f) Severe obstruction of the nasal valve, with a tendency toward valve collapse and a ptotic tip. Contraindications for septorhinoplasty for a functional tension nose or an overprojected nose or tip are based on functional and aesthetic considerations. Other contraindications may be due to underlying conditions (e.g., coagulation disorders, hypertension) or systemic diseases (diabetes mellitus). The patient’s skin and connective-tissue type may prohibit the use of certain operative techniques. For example, very thin skin through which the contours of the alar cartilages can be seen preoperatively would contraindicate grafting procedures on the tip. An overprojected nose with a convex dorsum may be an ethnic feature. It may be very desirable to preserve this convexity at operation. We have also seen cases in which the patient desired straightening of the nasal dorsum but her family did not. The operation should not be scheduled until an agreement has been reached. As with every nose, facial proportions should be considered in the assessment of the functional tension nose, especially the position of the chin, forehead, maxilla, and mandible in the three standard views: frontal, lateral, and basal. When the tension nose is viewed from the front, the bony and cartilaginous framework appears thin and the nasal base is narrow. The skin of the supratip and tip area is tight, pale (hypoemic), and relatively immobile. The nasal dorsum and tip are usually narrow. The infratip triangle is usually too long. In the basal view, the nares appear narrow and slit-like rather than elliptical, and they terminate in a high “gothic” vestibule. The alar lateral crura and upper lateral cartilages are medialized (see Fig. 11.6). Typical associated profile changes are described in the section on Aesthetic Indications earlier in this chapter.15 Especially in patients with a functional tension nose, palpation of the external and internal nose yields information that is important for surgical planning. It is easier to palpate tension than to see it. Active anterior rhinomanometry should be performed to objectify the subjective sensation of obstructed nasal breathing. This study is based on the synchronous recording of the narinochoanal pressure difference ΔP (in Pa) and of the nasal airflow V (in cm3/s).12,16 If there are signs of nasal valve stenosis, Bachmann recommends the dilatation test. Spreading open the upper part of the valve with a small cotton ball can demonstrate the pathological significance of the morphological or functional valve stenosis. The dilatation curve in this case is better than the resting curve.17 The preoperative consultation with the patient is held at least 24 hours before the operation and is preferably conducted by the surgeon or a physician representing him or her, following the recommendations given in Chapter 5. The doctor and patient review the agreed surgical goals, preferably aided by clinical photographs or drawings, and the patient is informed about all possible complications. The points that have been reviewed are documented. The patient signs a consent form stating that all necessary information has been presented (verbally and in writing), that the patient understands all of this information, and that he or she consents to the operation. Patients with an overprojected nose or nasal tip often want to have the desired surgical result simulated preoperatively on a computer screen so that they can see their “new” nose and appreciate the overall effect of the operation on the face. This wish is justified, given the radical effect that this type of surgery can have on the patient’s appearance. Opinions differ as to the value of graphics programs in preoperative planning. We offer our patients this option and have had positive experience with it. One advantage is that the doctor and patient have 20 to 30 minutes in which they can thoroughly discuss and review the surgical goals. During this time, the doctor can learn a great deal about the patient’s wishes. Only those changes that can actually be effected in the nose should be simulated on the computer. The simulated image is not the blueprint for judging the success of the operation, but only a tool for comprehension and planning. Consequently, we do not save the simulated image but document the desired result in a diagram.18 Modern septorhinoplasty is a well-planned and atraumatic procedure with less bleeding. If there are signs of bleeding, the routine workup includes a simple blood count (Hb, platelets, leukocytes). Coagulation parameters (quick prothrombin time [PT], partial thromboplastin time [PTT], and thrombin time) are also determined. Patients are asked about the use of cardiovascular medications or “blood thinners.” If patients report the use of nonsteroidal anti-inflammatory agents (e.g., aspirin, acetylsalicylic acid), a platelet function test is indicated. If this test is delayed, the operation should be postponed. The workup should include an allergy test if there is evidence of perennial or seasonal allergy. At least a plain radiograph of the paranasal sinuses should be obtained prior to any septorhinoplasty. If sinus disease is present, the sinuses should be evaluated by coronal computed tomography or digital volume tomography (DVT). Function studies consist of active anterior computerized rhinometry with a decongestion test and olfactometry with a threshold and identification test by Sniffin’ Sticks. Patients with middle ear ventilation problems or otitis media should be assessed with tonal audiometry and tympanometry. Silicone foils or Doyle splints are used to stabilize the nasal septum. They are removed on the third to fifth postoperative day. Merocel packs can be left in the ethmoid for 2 to 3 days, but intranasal packs should be dispensed with whenever possible. Steri-Strips are affixed to the external nose, placing light traction or pressure on the nasal tip according to requirements. The internal nose is treated with nasal oil (e.g., GeloSitin, Coldastop) and an isotonic saline spray (e.g., Emser Sole Spray, Rhinomer). Intranasal crusts are removed under endoscopic control. Further details on postoperative care are presented in Chapter 15. Although the nose consists of only a few structural elements, the variations in their size, arrangement, and interrelationships lead to countless shapes and nuances. Ultimately, no two noses are alike. The preoperative morphological analysis of an overprojected nose or a functional tension nose is essential for a successful operation. Through inspection and palpation, the surgeon can determine which structural elements are the major causes of the overprojection or tension deformity of the nasal inlet. Hyperplasia is rarely confined to a single structure, but often only a few features are chiefly responsible for the overprojection. Although the operation focuses on the main anatomical problem based on this morphological analysis, the surgical correction of an overprojected nose always requires more or less extensive changes in multiple structural components of the nose in order to achieve the most natural and harmonious result. Because an overprojected nose is always a result of hyperplasia, surgical treatment consists mainly of a series of resections. 1. Reduction or resection of hyperplastic structural elements. 2. Selective weakening of tip support mechanisms as described by Tardy19 (Figs. 11.7 and 11.8a–f).
The Functional Tension Nose, the Overprojected Nose
11 The Functional Tension Nose, the Overprojected Nose
11.1 Introduction
11.1.1 Definition of Terms
11.1.2 Measurement of Overprojection
 Is the nose or tip overprojected?
Is the nose or tip overprojected?
 Does the patient have maxillary or mandibular prognathism?
Does the patient have maxillary or mandibular prognathism?
 How does the forehead affect the profile (high or sloping forehead)?
How does the forehead affect the profile (high or sloping forehead)?

11.2 Indications
11.2.1 Functional Indications
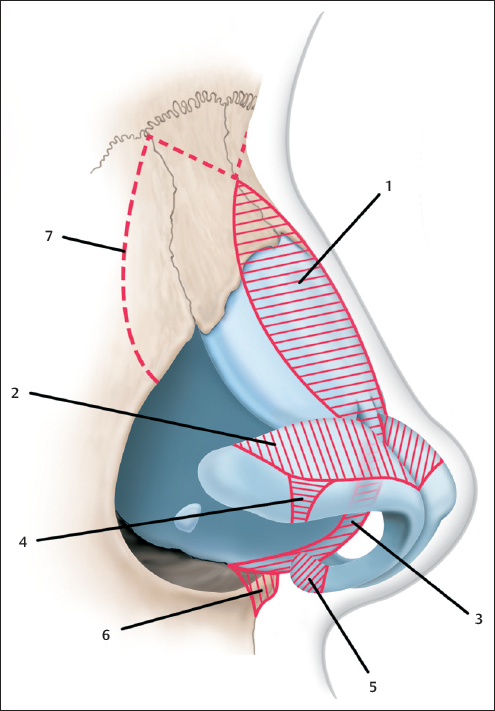
 Black: normal nose.
Black: normal nose.
 Red: functional tension nose without overprojection.
Red: functional tension nose without overprojection.
 Blue: overprojection tip.
Blue: overprojection tip.
 Green: overprojected functional tension nose.
Green: overprojected functional tension nose.
11.2.2 Aesthetic Indications
11.3 Contraindications
11.3.1 Functional Contraindications
 Good nasal breathing in computer rhinomanometry.
Good nasal breathing in computer rhinomanometry.
 No stenosis or collapse of the nasal valve, no inspiratory alar collapse.
No stenosis or collapse of the nasal valve, no inspiratory alar collapse.
 Function should not be sacrificed for morphological change. If significant reduction of the dorsum is needed, the surgeon should use spreader grafts, for example, or alternative techniques to establish a functioning nasal airway.
Function should not be sacrificed for morphological change. If significant reduction of the dorsum is needed, the surgeon should use spreader grafts, for example, or alternative techniques to establish a functioning nasal airway.
11.3.2 Aesthetic Contraindications
 Adverse effects on the overall profile. For example, a high nasal dorsum “lightens” a heavy, massive chin, even in prognathism. Lowering the dorsum in this case would further accentuate the lower half of the face.
Adverse effects on the overall profile. For example, a high nasal dorsum “lightens” a heavy, massive chin, even in prognathism. Lowering the dorsum in this case would further accentuate the lower half of the face.
 The correction of an overprojected nose, possibly combined with a mentoplasty, can radically alter the facial appearance. If the patient does not want this, the surgery may be contraindicated.
The correction of an overprojected nose, possibly combined with a mentoplasty, can radically alter the facial appearance. If the patient does not want this, the surgery may be contraindicated.
11.4 Preoperative Preparations and Prerequisites
11.4.1 Inspection
11.4.2 Palpation
 External nose: size, shape, and resilience of the alar cartilages; palpation of the anterior septal angle; tip recoil and tip support.
External nose: size, shape, and resilience of the alar cartilages; palpation of the anterior septal angle; tip recoil and tip support.
 Internal nose: anterior septum, anterior nasal spine, membranous septum, medial crura, and footplates.
Internal nose: anterior septum, anterior nasal spine, membranous septum, medial crura, and footplates.
11.4.3 Function Studies
11.4.4 Informed Consent
11.4.5 Photographic Documentation and Computer Simulation
11.4.6 Laboratory Tests
11.4.7 Postoperative Measures
11.5 Preoperative Analysis
11.5.1 Principles of Surgery for the Overprojected Nose and Tension Nose
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine