This procedure has supplanted Muller’s muscle conjunctival resection (MMCR) and levator aponeurotic advancement in my practice, which is a mixed cosmetic and functional blepharoplasty practice. It is more reliable and stable over time than aponeurotic surgery and does not require the second internal incision as with MMCR with its attendant concerns regarding direct contact with the ocular surface. It is a valuable adjunct to the cosmetic blepharoplasty surgeon’s armamentarium with a low complication rate and a high rate of patient and surgeon satisfaction.
Key points
- •
Involutional ptosis is rather common in patients requesting cosmetic blepharoplasty and contributes to the appearance of fatigue.
- •
Ptosis repair is sometimes unpredictable and can be challenging to the casual ptosis surgeon.
- •
Whitnall’s ligament suspension allows maximal reliable levator aponerurotic repair of involutional ptosis with minimal complications.
Ptosis often must be addressed in order to maximize the aesthetic result of upper blepharoplasty. Ptosis repair is one of the most common procedures performed in an oculofacial surgeon’s practice.
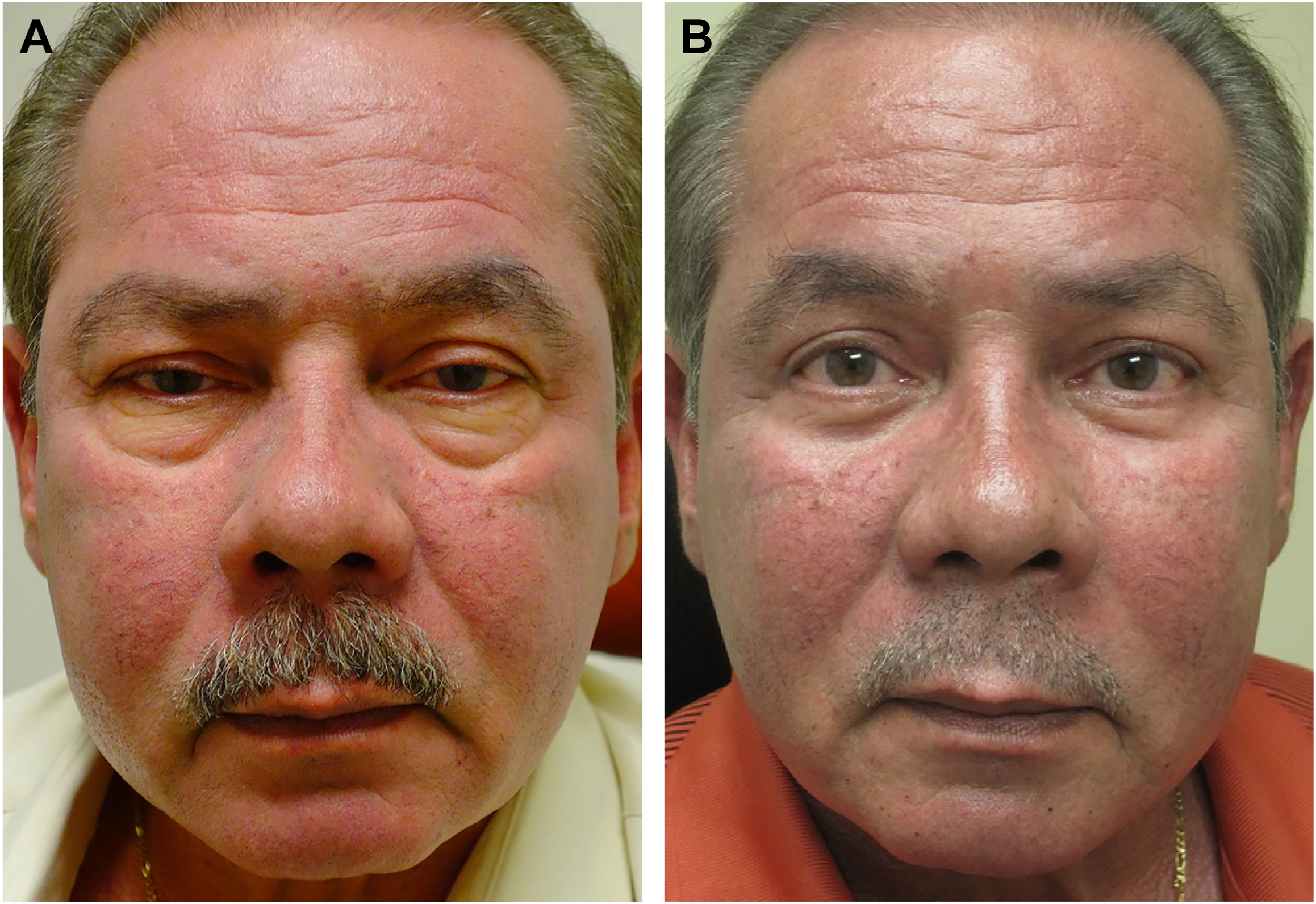
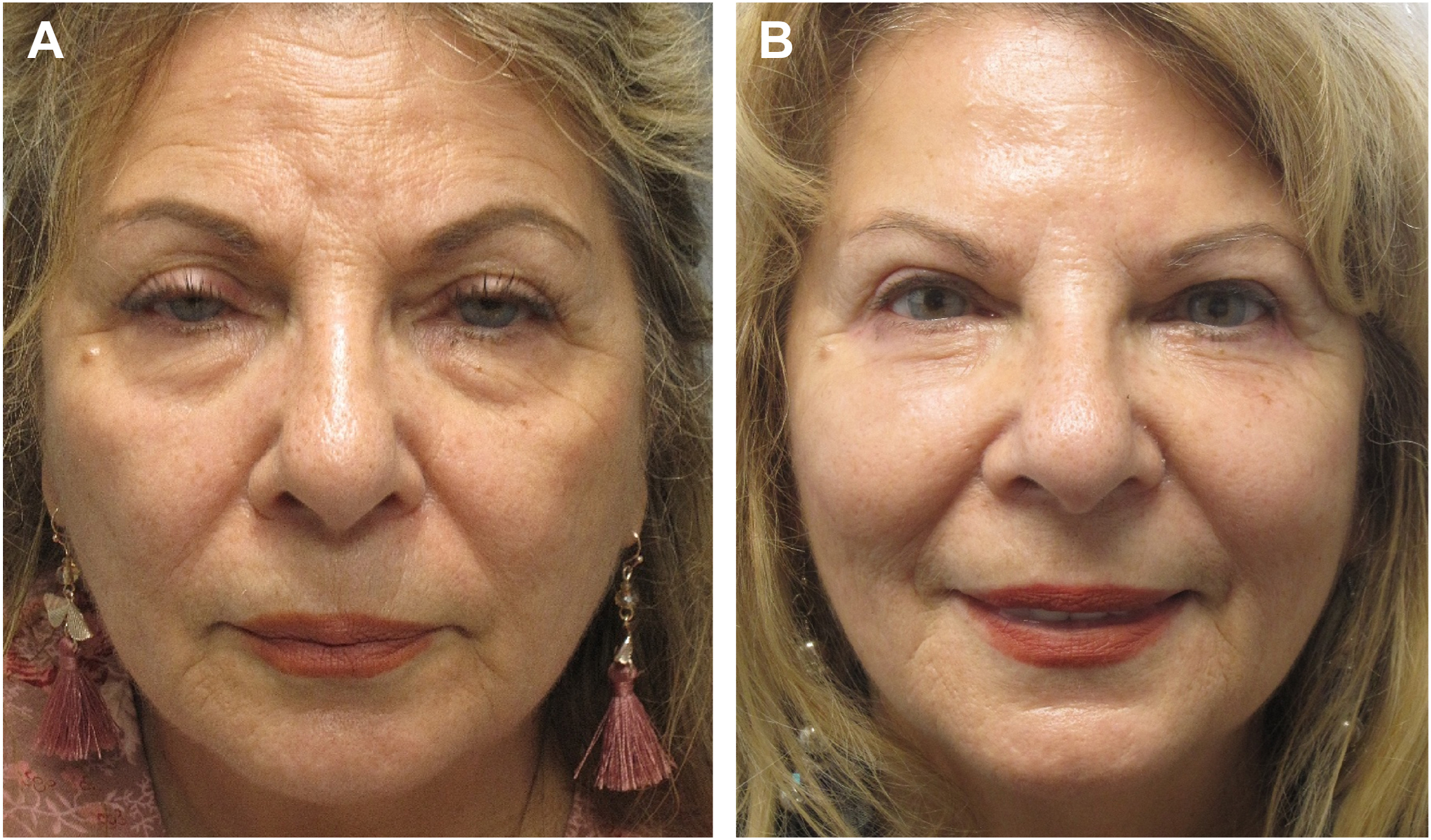
Older patients frequently present with ptosis severe enough to interfere with activities of daily life, manifesting margin-to-reflex distance of 2 mm or less. Aesthetically, ptosis creates a tired, inattentive appearance, especially when combined with orbitomalar sulcus deflation and midface descent, and/or frank steatoblepharon. Patients are thought to be sleepy, under the influence of alcohol or drugs, or unintelligent, based on the appearance of upper eyelid drooping [ ] Correction of ptosis when combined with upper and/or lower cosmetic blepharoplasty results in a refreshed younger more alert appearance and hence a more comprehensive facial rejuvenation than would be accomplished without ptosis repair. A series from the Mayo Clinic reported that “up to 21% of patients undergoing upper blepharoplasty required ptosis correction in addition to upper blepharoplasty” [ ] ( Fig. 1 A, B , Fig. 2 A, B ).
Ptosis repair can be challenging to occasional and even frequent blepharoplasty surgeons. Approaches that are simple and reliable and that do not require secondary surgeries are highly desirable. One of these techniques is the Muller’s muscle conjunctival resection (MMCR), which may be useful in patients with ptosis responsive to Neosynephrine. One disadvantage of the technique is that it requires an internal incision in addition to an external upper blepharoplasty incision (if needed if involutional aesthetic issues are to be addressed) which can result in increased swelling, and discomfort related to corneal irritation and chemosis.
For the past 8 years, I have been utilizing a technique of plication of the levator aponeurosis to Whitnall’s ligament, which fulfills the above criteria with great success and a minimal reoperation rate. It is a valuable addition to the cosmetic surgeon’s armamentarium. Herein, I will describe the anatomy necessary to an understanding of the procedure, the technique itself, and show some typical results.
Causes of involutional ptosis
Multiple causes of ptosis are well-described and include congenital ptosis, mechanical ptosis, myogenic ptosis, neurogenic ptosis, and neuromuscular junction-related. Involutional ptosis is the most common cause of aesthetic ptosis. Levator function is normal, and the upper lid crease is usually elevated with hollowing of the upper sulcus.
Changes in the aponeurosis or its relationships to adjacent eyelid tissues are generally thought to be the root cause of ptosis, with combinations of dehiscence, attenuation, or elongation described. A decline in levator palpebrae superioris function with age has also been recognized, and the severity of involutional ptosis has been shown to be associated with diminished levator function in many cases [ ]. The variety of procedures espoused to correct involutional ptosis may, in part, be related to the variety of underlying pathoanatomic elements.
Anatomy of Whitnall’s ligament
Whitnall’s ligament was first described in 1910 by Dr Samuel Ernest Whitnall as a superior transverse ligament at the junction of the levator muscle and its aponeurosis [ ]. Anderson and Dixon’s seminal article in 1979 further elaborated the anatomy and function [ ]. Further investigation was done by by Codère and colleagues [ ]. The ligament originates medially at the superior border of the trochlea and the adjacent orbital bone and traverses horizontally to the lateral orbital wall between the palpebral and orbital lobes of the lacrimal gland, merging with the anterior fascia of the levator muscle. The ligament has variably been referred to as the anterior transverse ligament or check ligament [ ]. It is composed of collagen and a variable amount of elastin. There is a less robust inferior transverse component beneath the levator muscle and aponeurosis, which also spans the orbit and is described as forming a sleeve around the levator muscle. This structure has been called the intermuscular transverse ligament [ ], and it is said to contribute to the suspensory ligament of the superior fornix together with the superior transverse ligament or Whitnall’s.
The anatomy of Whitnall’s varies widely in thickness, continuity, and branching as illustrated in Anderson and Dixon’s original article in 1979 [ ], which included photographs of a “poorly developed” and a “hypertrophic” Whitnall’s ligament (their Figs. 5 and 6 ).
There has been some dispute regarding Anderson’s suggestion that Whitnall’s ligament provides a fulcrum directing the pull of the levator not only posteriorly but also superiorly. Goldberg and colleagues [ ] presented MR images of the levator muscle action and Whitnall’s motion during opening and closing of the upper eyelid. They concluded, “Whitnall’s ligament …travels anteriorly and posteriorly with the excursion of the levator muscle.” The elastic nature and vector of Whitnall’s motion can easily be observed intraoperatively when the patient is asked to open the eyes, and the ligament follows the levator into and out of the orbit. One may observe a mild pulley action redirecting the vector, but primarily the ligament directly follows the levator muscle’s movement.
In Anderson’s article, his anatomic dissections demonstrate the inferior movement of Whitnall’s with closure of the eye, which may allow closure even when it is sutured to the tarsus, and hence the absence of lagophthalmos noted after their “Whitnall’s sling” procedure (Anderson and Dixon [ ]; see Figs. 1 A, B and 2 A, B).
My experience performing this procedure has shown me that Whitnall’s ligament is quite variable in structure and robustness, from dense to fibrillar and branching, and rarely can barely be discerned, and it occurs only very rarely as low as the superior margin of the aponeurosis.
Whitnall’s Ligament and Ptosis Repair
The technique of Whitnall’s suspension to correct ptosis has been described in the literature almost exclusively for the treatment of congenital ptosis with poor levator function. Its use has been advocated by Anderson as a “Whitnall’s sling” [ ] and others as a substitute for levator resection in severe congenital ptosis. Daoudi and colleagues [ ] evaluated Whitnall’s suspension alone in severe congenital ptosis with good results.
A 2020 report by Pfeiffer and colleagues [ ] from Europe compared involutional ptosis repair by “simple reinsertion” of dehisced aponeurosis to tarsus, compared to “double reinsertion” suturing aponeurosis to tarsus and also suturing Whitnall’s to tarsus. Anatomically, they describe an upper transitional zone (UTZ) of 1 to 5 mm or more between the upper edge of the aponeurosis and Whitnall’s ligament in 70.5% of cases, which is consistent with my observations. They noted improved correction of ptosis using the Whitnall’s suspension particularly in cases of a larger gap (UTZ) between the superior border of the aponeurosis and Whitnall’s, supporting the Whitnall’s technique in a majority of cases.
Techniques for correction of involutional ptosis
Two procedures are commonly used to correct involutional or aponeurotic ptosis. MMCR described by Alan Putterman [ ] has the advantage of avoiding a skin incision and may be considered “minimally invasive.” Several protocols have been advocated for determining the degree of resection to be performed, but none are definitive [ , ]. Multiple reports have compared levator aponeurotic advancement technique with MMCR, but the results appear similar [ ].
It is reported that the incidence of reoperation is lower with MMCR. BenSimon and colleagues [ ] compared MMCR to levator advancement and reported a slightly higher reoperation rate following aponeurotic advancement, but insofar as MMCR is often performed on patients with less severe ptosis, it is unclear whether the variable results are due to patient selection or the technique used. Chang and colleagues [ ] concluded in a review that there is no level 1 evidence to compare the techniques.
Levator aponeurotic repair or advancement (LAA) is usually performed under local anesthesia with mild intravenous sedation to allow patient cooperation opening and closing the eyes intraoperatively. In the case of frank dehiscence, the aponeurosis may be reapproximated to the tarsus. A common variation in technique is dissection posterior to the levator aponeurosis to allow full thickness advancement of the aponeurosis as a free flap. The commonest maximal use of the LAA involves plication from the tarsus to the superior margin of the aponeurosis. More lift can be achieved with partial tarsal resection.
One to three plicating sutures have been described. The patient is awakened and asked to open their eyes. The lids are then adjusted with attention to height, contour, and symmetry. The lid margin is placed 1 to 2 mm above the desired height to compensate for the loss of tone of the orbicularis due to local anesthesic infiltration. The elevation is limited to the superior edge of the aponeurosis as the sutures are generally not placed into the levator muscle itself in this procedure.
In my fellowship training with Stephen Bosniak and Serge Morax, a simplified approach to levator advancement was used, plicating the anterior surface of the aponeurosis to the anterior surface of the tarsus with no posterior dissection or resection.
For the past 8 years, I have been performing levator advancement plicating the anterior surface of the tarsus to Whitnall’s ligament with one horizontal mattress suture of 6-0 silk in most cases of involutional ptosis with margin-reflex distance (MRD) of 2 mm or less and levator excursions of 8 mm or more with excellent results in several hundred cases. Because Whitnall’s moves in concert with the levator muscle, I have had one case of mild lagophthalmos. If there is undercorrection, I can be certain that the maximal correction has been achieved without a more complex procedure such as levator resection, or aponeurotic advancement combined with tarsal and/or Muller’s resection. If more lift is required, sometimes, revision by MMCR is helpful. The Whitnall’s procedure is my default procedure for involutional ptosis repair.
Surgical technique
I have used CO 2 laser as a cutting tool since the early 1990s for almost all eyelid procedures. The laser causes less burning and charring than monopolar cautery, with the Bovie cautery operating at 1204 degrees C and the CO2 laser at 100 degree C (James Zins MD, 2019, personal communication), and hence I believe less stimulation of scarring and cicatricial issues of induration and contraction. The 0.2 mm laser spot is used in continuous mode at 5 to 6 W using stainless steel corneal protectors.
The upper eyelid creases are marked in the desired location, usually asking the patient to open and close and verifying symmetry with calipers centrally, medially, and laterally. If skin or skin and muscle resection is elected to correct excess skin weighing down the eyelids or to improve cosmesis, a pinch technique is used. With the eyes open, the apex of the eyelid contour is marked to locate the center of the plicating suture.
The skin and orbicularis are incised in a single layer and the skin muscle flaps excised exposing the orbital septum. The septum is tented and the preaponeurotic fat is exposed. The fat is peeled off the aponeurosis from inferior to superior with light passes of the laser dividing the fine attachments until Whitnall’s ligament is exposed. The anterior surface of the tarsus is exposed. There is generally minimal to no bleeding with the use of the CO 2 laser.
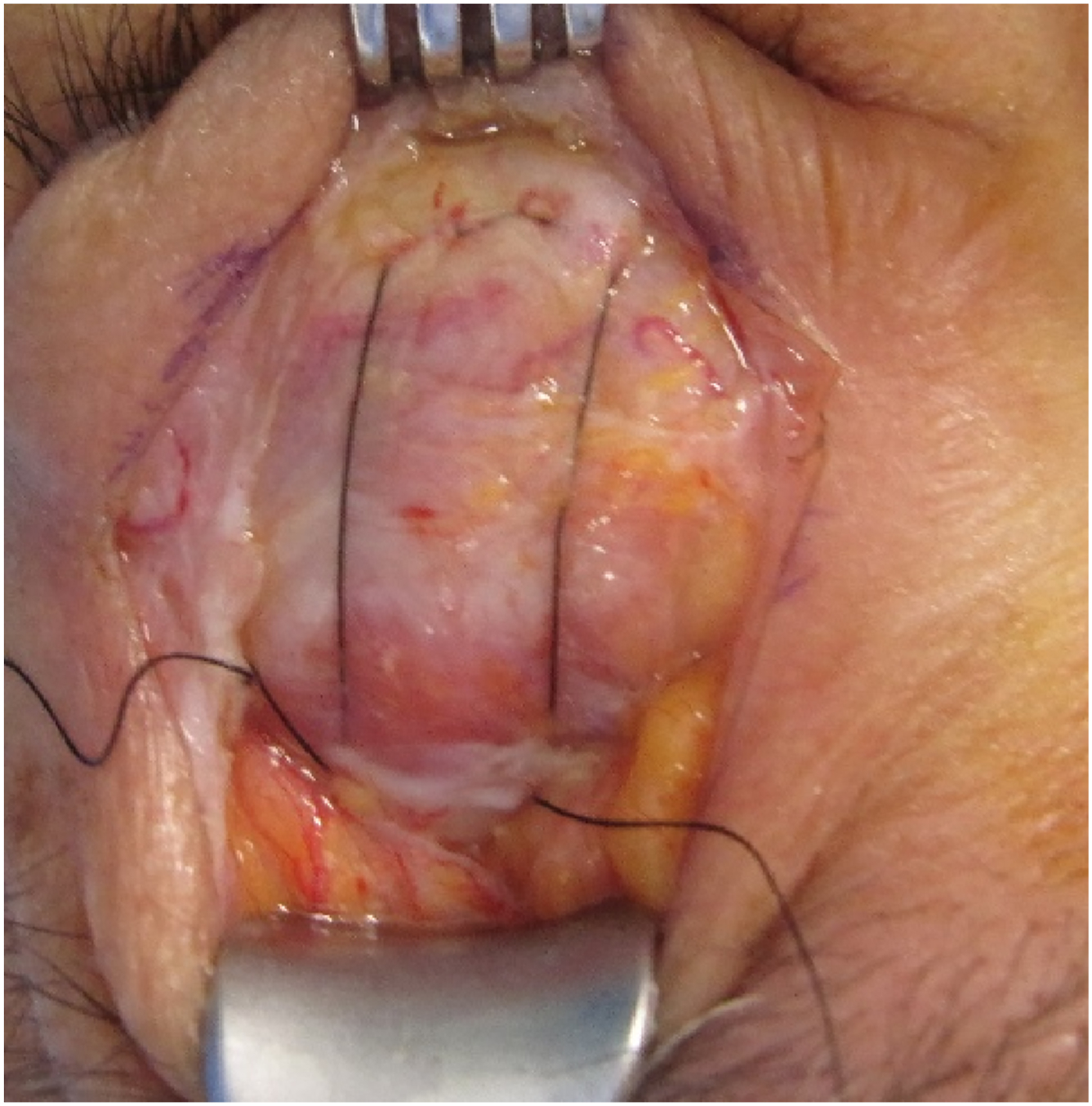
A double-armed 6-0 silk suture with a small spatula needle (Ethicon 769 – Rariton, NJ) is passed horizontally with three or four. half-depth bites of the tarsus centered on the apex of the contour 2 mm inferior to the superior border, taking care to avoid Mullers muscle. The small spatula needle facilitates the half -depth bite of the tarsus. The eyelid is everted to verify that the suture bites are not full thickness. The suture is then passed through Whitnall’s ligament in a horizontal mattress manner as wide as the lateral and medial points of entry into and out of the tarsus and tied temporarily with a slip knot. Whitnall’s has significant variation from very robust and thick to fibrillar and attenuated, occasionally with a diagonal orientation ( Figs. 3 and 4 ). The patient is awakened and the corneal shields are removed and the lights moved off the field, and the patient is asked to open their eyes. The height, contour, and symmetry are observed ( Figs. 5–13 ). Often the heights and contours are perfectly symmetric. This is one of the surprising advantages of this technique. Occasionally, there is some mild overcorrection or asymmetry, which a small hang-back can correct. The three or four bite tarsal stitch technique affords excellent contours in the vast majority of cases. The target height is between 1 mm below and 1 mm above the superior limbus with a higher level favored in patients with preoperative lesser levator excursions.
Related posts:
 Update on Anesthesia and Pain Management Strategies in Cosmetic Surgery
Update on Anesthesia and Pain Management Strategies in Cosmetic Surgery
 Body Contouring After Massive Weight Loss
Body Contouring After Massive Weight Loss
 Endpoints in Laser & Light-Based Devices
Endpoints in Laser & Light-Based Devices
 Adjustments to the Maxillofacial Skeleton to Improve Facial Harmony
Adjustments to the Maxillofacial Skeleton to Improve Facial Harmony
 Advances, Techniques, and Complications Associated with Adjacent Fat Transfer in Lower Blepharoplasty
Advances, Techniques, and Complications Associated with Adjacent Fat Transfer in Lower Blepharoplasty
 Filler Rhinoplasty
Filler Rhinoplasty
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


