 FIG. 10-1. Periungual warts. |
Seborrheic keratoses
Acrochordons (skin tags)
Clavus (corn) or callus
Molluscum contagiosum (MC)
Squamous cell carcinoma
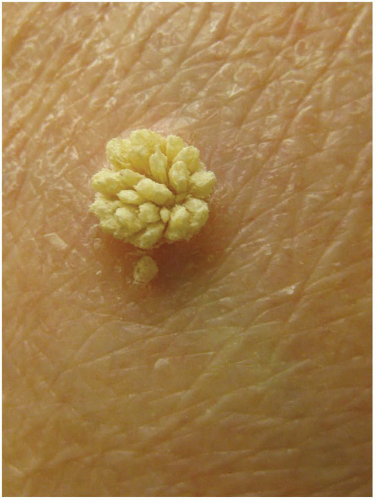 FIG. 10-2. Filiform wart. |
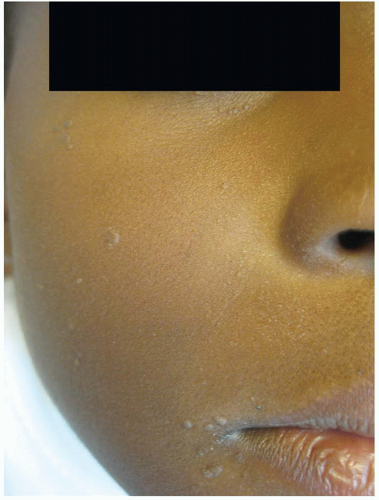 FIG. 10-3. Flat warts. |
thickened surface) on close examination can help to differentiate them from warts. Seborrheic keratoses are also often pigmented. Skin tags are soft, fleshy, pedunculated skin-colored papules that can have a clinical appearance similar to filiform wart, but will lack the characteristic finger-like projections on close examination.
 FIG. 10-4. Interrupted dermatoglyphics of warts. |
 FIG. 10-5. Thrombosed capillaries after paring wart. This sign is pathognomonic. |
TABLE 10-1 First- and Second-line Treatment Options for Warts | ||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||
dermatitis, a common phenomenon, is characterized by the development of eczematous patches or plaques surrounding the lesions. The dermatitis has been attributed to the localized reaction to the virus.
 FIG. 10-6. Classic molluscum lesion. |
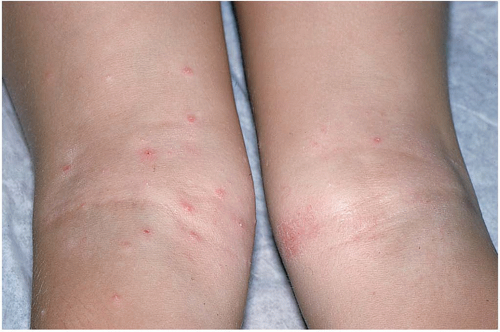 FIG. 10-7. Molluscum in atopic dermatitis. |
Genital warts
Folliculitis
Keratosis pilaris
Basal cell carcinoma
Infectious processes such as cryptococcosis or histoplasmosis
The central umbilication may not always be visible on clinical examination. Lightly spraying or touching the surface of the lesion with liquid nitrogen will often reveal this distinctive finding.
The umbilication will appear against the frozen white background and is a helpful diagnostic sign (Figure 10-9).
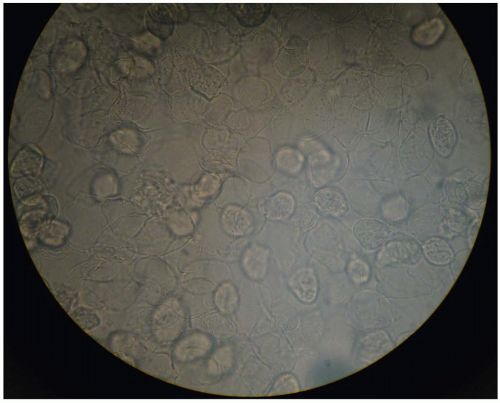 FIG. 10-8. Molluscum bodies on KOH prep. |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


