Raegan D. Hunt, Sheila Fallon Friedlander Viral infections can induce a remarkable variety of cutaneous manifestations in the neonate and toddler. The clinical manifestations of any viral infection are influenced by the virulence, tissue tropism, and age at which the infection is acquired. Infections may occur in utero, perinatally (acquired between the onset of labor and the delivery), or postnatally. Skin findings may be a result of local invasion and infection, or an indirect result of viral infection of other tissues. Diagnosis of infection is based on the morphology and distribution of the skin lesions, as well as the overall clinical presentation, supported by specific laboratory studies when possible. Rapid diagnosis and appropriate antiviral therapy maximize the possibility of a positive outcome for the infant. Herpes simplex virus (HSV) types 1 and 2 are pathogens for the fetus, newborn, infant and toddler, which induce a spectrum of clinical disease. Specific manifestations depend on the time and route of exposure as well as maternal immune status (primary vs recurrent maternal infection). HSV is a large, double-stranded DNA virus that can produce an acute primary infection in the susceptible host. In addition, HSV-1 and -2, like other herpes viruses, have the ability to integrate into host DNA and establish latency. Poorly understood host and environmental factors can cause reactivation of virus within latently infected sensory ganglia, leading to recurrent, active infections. Neonatal infection occurs most often as a direct result of active maternal infection, usually from primary infection acquired during pregnancy. The rate of neonatal disease has been shown to parallel the rate of genital herpes in a community.1 Neonatal infection is estimated to occur at a rate of 1 in 3000 to 1 in 20 000 live births. Infection of the fetus or newborn may occur during gestation (in utero), at the time of labor and delivery (perinatally), or following the delivery (postnatally). Although the majority of neonatal infections (80–90%) are considered to be acquired perinatally, both in utero infections (4%) and postnatal infections (10%) have been well documented.2 Most affected neonates acquire infection through contact with infectious genital secretions or herpetic lesions at the time of vaginal delivery. Although primary infection in the pregnant woman usually leads to symptomatic illness, a significant proportion of women with primary infection do not have recognizable systemic or local disease.3 Primary maternal infection is usually associated with prolonged shedding (2–3 weeks) of high titers of virus from lesions, while the maternal immune response develops, in contrast to the more limited viral shedding and much shorter duration of lesions (2–5 days) with recurrent disease in women with specific humoral and cellular immunity. Neonatal infection occurs in up to 50% of infants born to mothers during primary infection, compared with an estimated 2% or less of infants born to mothers suffering from recurrent infection; pre-existing protective maternal antibodies likely explain this difference in clinical outcome. Active maternal infection at the time of delivery, based on viral culture, is thought to occur in approximately 1–7 per 1000 births.4 However, data based on polymerase chain reaction (PCR) techniques from genital specimens at delivery suggest that active maternal infection may occur up to eight times more frequently than previously appreciated.5 Prospective studies have documented that the majority of women with active infection at the time of delivery are asymptomatic, suggesting that improved rapid laboratory diagnosis and careful examination are needed to identify the at-risk mother and infant. The optimal strategy for preventing neonatal HSV infection is controversial. Discordant HSV status of sexual partners is a risk factor if the female is susceptible, and queries regarding partner status and advice regarding abstinence near term for susceptible women with infected partners are appropriate. Routine HSV screening in pregnant women and antepartum HSV cultures in asymptomatic women with history of recurrent disease are not recommended. Based on evaluation of available limited or inconsistent scientific evidence (Level B), the American College of Obstetrics and Gynecology recommends that women with active recurrent genital herpes should be offered suppressive viral therapy at or beyond 36 weeks’ gestation and that cesarean delivery is indicated in women with active genital lesions or prodromal symptoms (e.g., vulvar pain or burning) at the time of delivery.6 Cesarean delivery is not recommended for women with a history of HSV who do not have active disease or have only non-genital disease at the time of delivery. Importantly, neonatal herpes infection has been described in infants born to mothers taking antiviral suppressive therapy and such cases may present with an atypical clinical picture and/or viral resistance patterns.2,7 Postnatal infections may be transmitted from both maternal, non-genital sites (including breast lesions) and non-maternal sources, such as other family members or nosocomial transmission from healthcare workers. In the absence of an HSV lesion on the breast, breast-feeding is not contraindicated. Active handwashing and awareness of transmission risk should be employed by all individuals with a history of or active HSV who are in contact with an infant. Congenital (intrauterine) infection was described in 1966 by Sieber and colleagues, in an infant with culture-positive lesions, seizures, and evidence of immunity at the time of a normal delivery in which the amniotic membranes were ruptured at birth.8 In 1969, South described an infant with microcephaly, microphthalmia, seizures, and vesicular lesions on the fingers and toes following a maternal primary HSV-2 genital infection during the first month of pregnancy.9 Subsequent studies of congenital infection have documented the presence of specific cell-mediated immunity to HSV in the newborn at birth, whereas infants infected during labor and delivery do not usually develop cellular immunity until the second week of the infection.10 Infection in utero may occur either as a result of ascending infection through apparently intact membranes, or as a result of viremia occurring with a primary maternal infection. Fetal infection often leads to fetal death; however, if the fetus survives, delivery may occur at term with late sequelae in both skin and central nervous system (CNS). Skin manifestations at delivery are the result of residua from primary fetal infection in addition to latent virus reactivation at previous cutaneous sites of fetal infection. Skin lesions are common in the neonatal period (Fig. 13.1). In one study, 70% of infected infants had vesicular lesions, and 30% also had evidence of scar formation on the face, trunk, or extremities.11 In addition, aplasia cutis congenita-like skin findings and lesions characteristic of epidermolysis bullosa have been described.12 Atrophic limbs, previously reported with congenital varicella virus infection, have also been documented with congenital HSV infection.13 HSV infections acquired in utero in which the infant completes a normal gestation are almost invariably associated with CNS damage, which is easily detected by computed tomography (CT). CNS changes indicate longstanding destruction of neuronal tissue without acute inflammation. Microcephaly is present in over 50%, and chorioretinitis is present in 60% of infants with congenital HSV infection. Although skin and CNS abnormalities are present at birth, infected infants often do not show the signs of systemic toxicity and overwhelming sepsis that may occur with primary perinatal or postnatal infection. Neonatal disease occurs in three clinically recognized syndromes, all acquired in the perinatal period: infection localized to the skin, eyes, or mouth (SEM disease); disseminated infection; and CNS infection. Exposure to maternal primary infection at the time of delivery may lead to overwhelming infection in the neonate, with a high mortality rate, or a more slowly progressive, insidious disease in which the infant has only mucocutaneous manifestations or develops slowly progressive neurologic symptoms. The incubation period varies substantially, from clinical symptoms at delivery due to presumed ascending infection through non-intact membranes, to infection presenting as late as 6 weeks of age. Infants with disseminated and SEM disease have an earlier onset, typically presenting between the first and second weeks of life. The variability of the incubation period is dependent on the integrity of the amniotic membranes, the inoculum of virus, the tissue inoculated (e.g., skin, mucous membrane), and the presence or absence of transplacental specific antibody. Cutaneous or mucosal lesions (mouth, nose, eye) can occur with or without signs of sepsis or encephalitis. Infants with skin, eye, or mouth disease account for 40% of all neonatal cases of HSV infection. The skin lesions appear as small, 2–4 mm vesicles, with surrounding erythema, often in herpetiform (zosteriform) clusters (Fig. 13.2). They usually occur on the part of the body which was in prolonged contact with the cervix. Often, lesions will occur at sites where the skin integrity has been breached. One of the most common sites of cutaneous infection is on the scalp vertex at the site of placement of fetal scalp monitor electrodes (Fig. 13.3). Vesicular lesions usually develop within the first 1–2 weeks of life following inoculation at this site. Lesions may progress locally, or disseminate (Fig. 13.4). In areas of mucosal involvement, a shallow ulceration with moderate inflammation is most often seen. The ulceration may be focal, with the lesion size closely resembling that of a cutaneous vesicle, or ulcerations may spread irregularly, coalescing over a much larger area. Lesions tend to follow the clinical stages of vesicle resolution seen in the older child, with pustulation 24–72 h after the appearance of the vesicle, followed by eschar formation. Skin lesions are present in most neonates with disseminated disease (77%), and in 60% of infants who present with CNS disease. In any newborn with skin or mucosal lesions of HSV, even without a history of symptomatic illness, an investigation must be undertaken to rule out disseminated or CNS disease. HSV dissemination is the most devastating manifestation, presenting in the more premature infant (average gestational age at birth of 36.5 weeks) at an average chronologic age of 11 days. Multisystem involvement is analogous to overwhelming bacterial sepsis. Shock, disseminated intravascular coagulation, and multiple organ system failure are characteristic. Involvement of the lung, liver, and brain is common. The mortality rate is high. Without antiviral therapy, approximately 75% of infants will die, and even with specific antiviral therapy, mortality is still significant. Neurologic sequelae in survivors are also common, occurring in approximately 40%. Statistically, these infants have the lowest average circulating concentration of antibody to HSV. In as many as 40% of infants ultimately diagnosed with disseminated or CNS infection, clinical disease begins with skin lesions only. Clinical and laboratory evidence of dissemination or CNS involvement not obvious at the time of presentation may develop during the first days of treatment, despite antiviral therapy. Infants with HSV encephalitis present at a slightly older age (mean 17 days) and tend to be full term, in contrast with newborns with other clinical presentations. Antibody titers are higher in this group, leading to speculation that antibody may modify the progression of disease, with virus inoculated at delivery producing a clinically undetectable initial infection which spreads from mucosal sites to the CNS. Subtle neurologic symptoms are often present for days before the parent recognizes that the infant requires medical attention. As the child becomes more irritable and seizures become more pronounced, infants are hospitalized and evaluated. Skin lesions are only present in 60% of infants with HSV encephalitis, making the diagnosis difficult in many. The diagnosis of a herpes virus infection can be made in several ways (Table 13.1). HSV grows rapidly and easily in cell culture, and evidence of infection may be evident within the first few days after inoculation. Culture remains the most accurate means of diagnosis, but adjunctive tests may provide more rapid results. All suspected cases should have the following samples collected: (1) swab specimens from mouth, nasopharynx, conjunctiva and anus for HSV culture (the same swab can be used to test all sites, ending with the anus); (2) skin vesicle and CSF for PCR and culture analysis; (3) whole blood sample for PCR; and (4) blood sample for ALT testing. The most rapid results can be obtained from scraping of a vesicle sent for histopathologic Tzanck smear analysis, but this test is probably the most unreliable due to interpreter variability and sampling error. Direct fluorescent antibody testing (DFA) is rapid and specific, but not as sensitive as culture. CNS evaluation is necessary to rule out encephalitis. This includes traditional CSF analysis, as well as PCR. CT of the brain may be helpful in the diagnosis of encephalitis but is not considered sensitive until after 5 days of CNS symptoms. Magnetic resonance imaging (MRI) is more sensitive for CNS inflammation of the temporal lobes – the preferred sites of viral replication – and may be diagnostic within 3 days of onset of symptoms. EEG can also be helpful in CNS infections localized to the temporal lobe and may be positive earlier than any imaging study. TABLE 13.1 Diagnosis of infection a Viral PCR panels are available in some centers and PCR diagnostic technology is rapidly evolving. Disseminated infection with HSV produces a clinical picture similar to that of early-onset neonatal sepsis caused by group B Streptococcus, enteric Gram-negative bacilli, and Listeria. Empiric therapy with antibiotics (standard management for the hospitalized ill neonate) will have no effect on the progression of HSV disease. For infants with progressive clinical symptoms of sepsis and sterile bacterial cultures of blood, urine, and CSF, HSV should be considered as a potential pathogen. Other viral infections in the newborn period may also be confused with HSV. Enteroviral infection can cause a wide spectrum of clinical signs in the neonate, from fever and irritability to overwhelming sepsis with multiple organ system failure, to aseptic meningoencephalitis with minimal symptoms of systemic toxicity. Enteroviral infections may be associated with cutaneous vesiculopustular lesions. Neonatal seizures caused by enteroviral infections are the result of diffuse CNS irritation, in contrast to the focal temporal lesions of early HSV disease. Destructive changes of HSV that are appreciated on serial imaging studies of the CNS (by either CT or MRI) are not generally seen with enteroviral disease. Perinatal varicella may produce overwhelming sepsis in the newborn. The density of cutaneous lesions in neonatal varicella usually far exceeds that seen with HSV infections, which characteristically produce a focal cluster of lesions at the site of inoculation with minimal cutaneous dissemination. However, both demonstrate the identical findings of multinucleate giant cells on Tzanck preparations. Only virus-specific staining techniques, PCR, or culture will be able to differentiate between these viruses. Other viral pathogens occasionally cause severe acute disease in the newborn, including influenza A and B, parainfluenza 1, 2, and 3, and adenovirus. In general, the seasonal context of the infection, exposure history, and a predominance of respiratory tract symptoms help differentiate these infections. Viral cultures of the respiratory tract will assist in the identification of these pathogens. Incontinentia pigmenti may present with localized vesicles, which may be mistaken for herpes simplex infections. These infants often have peripheral eosinophilia. Biopsy will reveal increased numbers of eosinophils, and cultures will be negative for HSV. Vesicular lesions that appear herpetic can also occur in Langerhans’ cell histiocytosis. Tzanck preparation will reveal histiocytes, and biopsy will show large numbers of histiocytes and an absence of multinucleate giant cells. Additionally, epidermolytic hyperkeratosis (EHK), epidermolysis bullosa (EB), congenital erosive and vesicular dermatosis, and ankyloblepharon-ectodermal dysplasia clefting syndrome can present with denuded eroded skin and bullae which may be confused with HSV. The treatment of choice in neonatal herpes infections is acyclovir administered intravenously, regardless of the clinical presentation (Table 13.2). Acyclovir 60 mg/kg per day in three divided doses should be given for 14 days for SEM, and for a minimum of 21 days in those with disseminated or CNS disease.14 In infants with renal failure, the doses should be reduced accordingly. The mortality rate for disseminated disease is about 29%, even with therapy. Approximately 50% of infants will experience cutaneous recurrences. Daily suppressive doses of oral acyclovir have been recommended to prevent skin recurrences and, in infants with CNS disease surviving neonatal HSV, treatment with suppressive doses of oral acyclovir for 6 months after the initial 14–21 day parenteral acyclovir regimen led to improved neurodevelopmental outcomes at 1 year of age.15 Valacyclovir is also efficacious in the treatment of HSV, but no oral liquid formulation currently exists. Pharmacokinetic studies have shown inter-infant drug clearance variability in those less than 3 months of age, and some experts therefore do not recommend use in very young infants.16 TABLE 13.2 Herpes virus infections in neonates and infants a Adapted from Red Book: 2012 Report of the Committee on Infectious Disease, American Academy of Pediatrics, 2012. At least 25% of US children have serologic evidence of HSV-1 by age 7 years. HSV infections in young children may present with clusters of erosions and vesicles (Fig. 13.5). However, most primary, non-neonatal HSV infections are asymptomatic. Gingivostomatitis secondary to HSV-1 is the most common presentation in childhood, generally occurring from 1 to 5 years of age. Children may be quite ill, with fever, drooling, submandibular adenopathy, and diffuse edema and erythema of the gingiva and oral mucous membranes. Extension of lesions to the lips, chin and cheeks often occurs. Ulcers, erosions, and oral symptoms can be so severe that hospitalization may be required for intravenous hydration support. The differential diagnosis includes coxsackie virus infection, Stevens–Johnson disease, and aphthous ulcers. Isolated HSV labialis may also occur, but less frequently. HSV infection of the pulp of the distal phalanx of a digit, termed herpetic whitlow can occur in children as an isolated finding. Such lesions are slate-gray, vesicular, and painful (Fig. 13.6 This form of severe HSV cutaneous infection develops in individuals who suffer from a chronic skin condition. Though most commonly seen in association with atopic dermatitis, it can be associated with disorders such as Darier disease or pemphigus vulgaris. Patients develop vesiculations and erosions predominantly in affected dermatitis sites where the skin barrier is presumably impaired and more vulnerable to viral invasion. The lesions often have a ‘punched-out’ monomorphous appearance, and vesicles may not be evident (Fig. 13.7). These children may have high fevers and appear ill. Secondary bacterial infection of the skin and keratoconjunctivitis may also develop. The differential diagnosis includes varicella infections, including zoster, and secondary bacterial infection of primary skin conditions. Families should be counseled regarding the risk of recurrence, and the need to protect their child from direct exposure to active herpes lesions in others. Therapy of HSV infections in children depends on the severity of involvement and underlying immune considerations. Immunocompromised children and those with eczema herpeticum will often benefit from intravenous therapy. Bland emollients are also often utilized; in children with eczema herpeticum, topical corticosteroids are then added once the infection appears to be responding to antiviral therapy. Most other conditions can be treated with oral therapy if treatment it desired. Varicella (chickenpox) is usually a benign, self-limited disease when it occurs in immunocompetent individuals during childhood. The developing fetus and neonate, however, are at higher risk for an adverse outcome following infection. Fortunately, more than 90% of women are estimated to have varicella zoster virus (VZV) IgG seropositive status, thereby conferring immunity to the fetus. In addition, women planning conception are encouraged to seek VZV vaccination if they do not have evidence of prior immunity, substantially decreasing the risk of fetal infection. The widespread use of the varicella live attenuated (Oka/Merck) vaccine has led to a lower incidence of VZV disease in the general population, thereby decreasing the exposure risk to expectant mothers and infants. However, the vaccine is not 100% effective, and healthcare practitioners must be aware of the possible manifestations of varicella infection in neonates, as well as appropriate therapy. The exact incidence of varicella during pregnancy is unknown, but is estimated to be between three and 10 cases per 10 000 pregnancies. Fetal or early neonatal exposure may result in a variety of manifestations, ranging from minimal cutaneous lesions to significant morbidity and death. Three distinct disorders may occur following intrauterine or neonatal exposure to VZV: fetal varicella syndrome, neonatal varicella, and infantile herpes zoster. Congenital defects predominantly involving the skin, nervous system, and musculoskeletal system can occur following fetal exposure to varicella virus. Other terms for the fetal varicella syndrome include varicella embryopathy and congenital varicella syndrome. Specific anomalies include cicatricial skin lesions that correspond to a dermatomal distribution, often with hypoplasia of underlying tissues. These lesions may initially appear as denuded areas and subsequently develop stellate or angular scars (Fig. 13.8). Low birthweight is a common finding in affected infants. The varied extracutaneous manifestations of this syndrome can be grouped as neurologic, musculoskeletal, ophthalmologic, gastrointestinal, and genitourinary. Limb paresis and hypoplasia of the extremities are common findings, as is chorioretinitis. Less common findings include microphthalmia, cataracts, nystagmus, hydrocephalus, and mental retardation (Table 13.3). Varicella zoster virus (VZV) is a herpes virus consisting of double-stranded DNA. The incubation period is usually 14 days, but ranges from 10 to 21 days after exposure. Most fetuses exposed to VZV during gestation will have no discernible sequelae. The greatest risk for fetal varicella syndrome occurs in the first 20 weeks’ gestation, with the highest risk (2%) between 13 and 20 weeks;17 a lower rate before 13 weeks (0.4%) may reflect underreporting or a higher rate of spontaneous abortion. Rare cases in the second half of pregnancy have been reported.18,19 A prospective study carried out in Germany and the UK between 1980 and 1993 identified 1373 women who had varicella and 366 who had zoster during the first 36 weeks’ gestation. Nine cases of congenital varicella syndrome were reported overall, and all occurred after maternal varicella infection in the first 20 weeks of pregnancy. The highest risk occurred between 13 and 20 weeks’ gestation, with seven cases noted in this subset. No cases of congenital varicella were noted following maternal herpes zoster during pregnancy. Herpes zoster in infancy was identified in 10 children whose mothers had varicella during pregnancy. Although 97 women who received varicella zoster immunoglobulin (VZIG) developed varicella, no cases of congenital varicella occurred in this group.17 Some believe that the failure to identify congenital varicella in late pregnancy reflects the limited statistical power of epidemiologic efforts, but nonetheless, late pregnancy is clearly a time of lower risk for the development of the classic stigmata of congenital disease.20 It has been postulated that the severe segmental anomalies that can be seen in fetal varicella syndrome are the result of reactivation of primary varicella in the developing fetus at a time when the immune system is not sufficiently developed to modify the severity of infection. Maternal herpes zoster does not appear to pose a significant risk to the fetus. No cases of congenital varicella occurred in a prospective study of 366 women who had zoster during pregnancy, and no serological evidence of transplacental transmission was noted.17 Approximately 18 cases of congenital anomalies occurring in association with maternal herpes zoster infection have been reported; however, it is not clear that these anomalies were a result of maternal zoster infection.21 A case of cutaneous lesions and limb hypoplasia in a fetus whose mother developed disseminated herpes zoster at 12 weeks’ gestation did appear consistent with fetal varicella syndrome, but localized maternal zoster has not been clearly implicated as a cause of fetal disease.22 The denuded or scarred areas seen with fetal varicella syndrome may be mistaken for aplasia cutis congenita or Bart syndrome. Other congenital viral infections should be considered in any infant presenting with microcephaly, ophthalmologic, or neurologic abnormalities. Prenatal diagnosis of fetal varicella syndrome using viral or immunologic methods is unreliable.23 IgM may be undetectable, even in infants with classic clinical findings. Infection before 18 weeks’ gestation may lead to a suboptimal or altered immune response resulting from immaturity of the fetal immune system. Prenatal diagnosis of intrauterine exposure to varicella may be accomplished by means of cordocentesis, amniocentesis, and chorionic villus sampling.23 IgM may be detected in cord blood as early as 19–22 weeks’ gestation. Virus can be grown from amniotic fluid and fetal blood samples, and DNA probes can be utilized to evaluate placental tissue.24,25 However, transplacental transfer of virus can occur without any significant sequelae to the fetus, and the degree of fetal involvement cannot be determined by immunologic or viral evaluation. Thus, although the above-mentioned evaluations may be useful in diagnosing fetal varicella syndrome, they are neither sensitive nor specific enough to accurately determine which fetuses will suffer untoward effects. High-quality ultrasound at 20–22 weeks’ gestation has been used as a means of surveying at-risk fetuses. Sonographic abnormalities include fetal hydrops, polyhydramnios, abnormal foci within the liver, microcephaly, and limb hypoplasia.26 Unfortunately, some findings may not be apparent until later in pregnancy. A report of a fatal case of varicella embryopathy that used ultrasonography and MRI at 26 and 32 weeks’ gestation found a high correlation between fetal imaging and subsequent pathologic findings, including limb involvement and even dermatologic features; however, MRI scanning was required to identify CNS abnormalities. The authors recommend combining prenatal ultrasonography with MRI in any woman noted to have varicella seroconversion during pregnancy.27 Varicella virus is not usually isolated from live-born infants with congenital infection, and other findings must be used to confirm the diagnosis. Criteria useful in confirming the diagnosis include clinical, virologic, or serologic evidence of maternal varicella infection during pregnancy; erosions or scars in a dermatomal distribution; and immunologic evidence of varicella infection in the infant, including IgM antibody or persistence of IgG antibody beyond 1 year of life in the absence of clinical varicella infection. The development of herpes zoster in the first year of life without a prior history of varicella infection is also good evidence that the infant was exposed to varicella zoster during gestation. In rare instances, varicella virus particles have been detected by means of electron microscopy in skin samples obtained at or near birth.24 Prevention by eliminating natural infection during pregnancy is the best approach to this disease, and should be facilitated by the increasing use of the varicella vaccine in childhood. Ideally, pre-conception evaluation should identify at-risk women, who should then receive the varicella vaccine before conceiving. No fetal anomalies have been reported in infants born to pregnant women who have received the vaccine inadvertently. Nonetheless, the vaccine, which is a live attenuated virus, is contraindicated in pregnancy. Therapeutic abortion is not automatically recommended to at-risk mothers as the risk of a fetal anomaly following exposure is so small.28 At-risk mothers known to have recent exposure to varicella during the first 20 weeks of pregnancy should have varicella serologic evaluation. Latex agglutination (LA), immunofluorescent assays (IFA), fluorescent antibody-to-membrane antigen assays (FAMA), and enzyme-linked immunosorbent assays (ELISA) are sensitive and specific.23 The LA test is also rapid and simple, making it quite useful in evaluating at-risk pregnant women. Varicella zoster immunoglobulin post-exposure prophylaxis may be offered to varicella-susceptible pregnant women. It may be administered within 96 h of exposure, but is most efficacious within the first 48 h. It does not reliably prevent maternal illness, but does modify the severity of infection. It is unclear whether VZIG prevents fetal varicella syndrome or neonatal infection, but there were no cases of fetal infection in 97 pregnancies complicated by maternal exposure and treated with post-exposure VZIG prophylaxis.17,29 Because fetal varicella syndrome is so rare, larger studies would be required to confirm protection. Exposed pregnant women who are seropositive for VZV do not require VZIG. Treatment with acyclovir should be considered in any pregnant women with varicella, particularly those in the third trimester, because of the risk of severe maternal disease, and to minimize the risk of neonatal disease in case delivery occurs during or soon after acute infection. The drug is usually well tolerated with little toxicity to the mother, but the risks and benefits to the mother and fetus have not yet been clearly delineated. The International Registry of Acyclovir Use During Pregnancy has followed at least 1246 fetal exposures to the drug, and no increased incidence of fetal abnormalities in exposed infants has been noted.30 It has not been determined whether such treatment will eliminate the risk of varicella embryopathy or infantile zoster in exposed fetuses. Ophthalmologic and neurologic evaluation of the infant born to a mother with varicella during pregnancy is indicated, as is careful examination of the musculoskeletal, genitourinary, and gastrointestinal systems for underlying anomalies. Neonatal varicella may result if a mother develops chickenpox before or immediately after delivery. If maternal varicella occurs from 5 days before to 2 days after delivery, the in utero-inoculated fetus is at high risk for severe disseminated disease. The clinical course of neonatal varicella can be quite variable. Those who are more likely to develop severe illness generally develop skin lesions within 5–10 days after delivery. Some children will develop a few cutaneous lesions, but otherwise remain well. Lesions often appear initially as small pink to red macules that relatively rapidly become papular and subsequently develop a teardrop-shaped vesicle. Other patients initially develop crops of cutaneous lesions that may evolve into hemorrhagic and/or necrotic vesicles (Fig. 13.9). Disseminated infection with widespread cutaneous and visceral involvement may develop and lead to severe morbidity. The mortality rate for neonatal varicella before the use of acyclovir has been estimated at 10–30%.28,29 Death from severe pneumonitis and respiratory distress often occurs 4–6 days after onset of lesions. Hepatitis and encephalitis may also develop. A study from Thailand in 1999, evaluating 26 children with neonatal varicella, reported no mortality. Of the 26 children, 12 received intravenous acyclovir.31 Infants may develop lesions from 1 to 16 days after birth if the mother experiences active disease near the time of birth. The usual onset of rash is 9–15 days after onset of maternal rash. Administration of VZIG may prolong the incubation period to 28 days.14 In aggregate data from two studies, 23–62% of infants whose mothers developed varicella in the last 3 weeks of pregnancy developed neonatal varicella.17 The risk of severe neonatal varicella is related to the timing of maternal infection, presumably because of a critical period when transmission of virus to the infant occurs prior to the development and transplacental transfer of maternal antibodies, which modify expression of the infection in the neonate. Smears of vesicles using a Tzanck preparation will demonstrate multinucleate giant cells and margination of chromatin. VZV PCR evaluation is also helpful and is more specific for VZV; vesicular swabs, scrapings, biopsy tissue and CSF can be evaluated by PCR analysis. Direct fluorescent antibody (DFA) tests are less sensitive than PCR and occasionally false-positive in disorders such as incontinentia pigmenti and Langerhans’ cell histiocytosis; therefore positive viral culture or PCR remain the best, most reliable means of diagnosis.32 A history of maternal varicella infection during pregnancy is also helpful but not necessary to confirm the diagnosis because infants may also contract the disease from siblings, care givers, and other close contacts. The differential diagnosis of vesiculopustular lesions is discussed in Chapter 10. Prevention is the best intervention. Delaying delivery until sufficient time has elapsed for transplacental transfer of maternal antibody is one approach; this generally occurs 5–7 days after the onset of maternal illness. Neonates born to mothers who have developed varicella from 5 days before to 2 days after delivery should receive VZIG intramuscularly as soon as possible after delivery.14 Direct contact between the infant and maternal skin lesions should be avoided, but breastfeeding is not prohibited if such contact can be avoided. Neonates who develop lesions or signs of infection should be treated with intravenous acyclovir, 20 mg/kg every 8 h for a minimum of 10 days. More prolonged therapy of 14–21 days may be necessary for disseminated or CNS infection.14 Aggressive supportive therapy is sometimes also required. The use of prophylactic acyclovir in high-risk infants has also been suggested by some authors. It should be borne in mind that any infant born to a woman who has had varicella within 3 weeks of delivery may be infectious at birth or shortly thereafter. If onset of maternal infection is within 1–2 weeks of delivery, many experts recommend that the child be isolated (from at-risk hospital personnel and other babies) from birth. If onset of disease occurs in the mother within 1 week of delivery, or following the birth of the infant, the infant should be isolated 7 days after the onset of maternal disease.14 If a mother develops a varicella rash 3 or more days after delivery, the infant may contract varicella but this will more likely be via the respiratory route, which theoretically leads to a smaller systemic inoculum and less severe disease. However, serious illness has been reported in the first 4 weeks of life when infants contract disease from their mother or siblings during this period. Severe infantile disease may occasionally occur even in infants born to immune mothers.33 If the mother is seronegative and the infant is exposed to an infectious sibling, many experts would recommend VZIG post-exposure prophylaxis for the infant. Post-exposure prophylaxis with acyclovir may be effective in older infants, but no data exist for its efficacy or safety in neonates. Although the mortality rate following noncongenital infantile varicella (0.008%) is higher than that in older children, it is still lower than the rate in immunocompromised individuals (7%) or following intrauterine exposure (10–30%).26 Recommendations regarding prophylaxis after VZV exposure vary. The UK Advisory Group on Chickenpox recommends routine administration of VZIG to all neonates following exposure. If sensitive and rapid testing is available, exposed infants may be tested and the use of VZIG avoided for those with passive antibody to VZV. Others recommend concentrating prophylactic measures on those infants less than 30 weeks old and weighing less than 1 kg. The Report of the Committee on Infectious Diseases of the American Academy of Pediatrics recommends VZIG for all exposed, hospitalized premature infants who are less than 28 weeks’ gestation, or who weigh 1 kg or less at birth. In addition, those exposed, hospitalized premature infants of 28 weeks or more gestation, born to mothers who are seronegative or lack a history of varicella infection, should also be given VZIG.14 Following primary infection, the varicella zoster virus persists in the sensory dorsal root ganglia and is kept in check by cell-mediated host immune mechanisms. Reactivation of the virus can occur and generally leads to localized involvement of skin and nerves in a dermatomal pattern corresponding to the ganglion in which reactivation took place. This disease, termed herpes zoster, has been recognized since antiquity. The term ‘zoster’ (girdle
Viral Infections
Introduction
Herpes simplex virus
Epidemiology
Intrauterine HSV infection
Cutaneous findings
Extracutaneous findings
Neonatal (perinatal) herpes simplex infection
Cutaneous findings

Extracutaneous findings
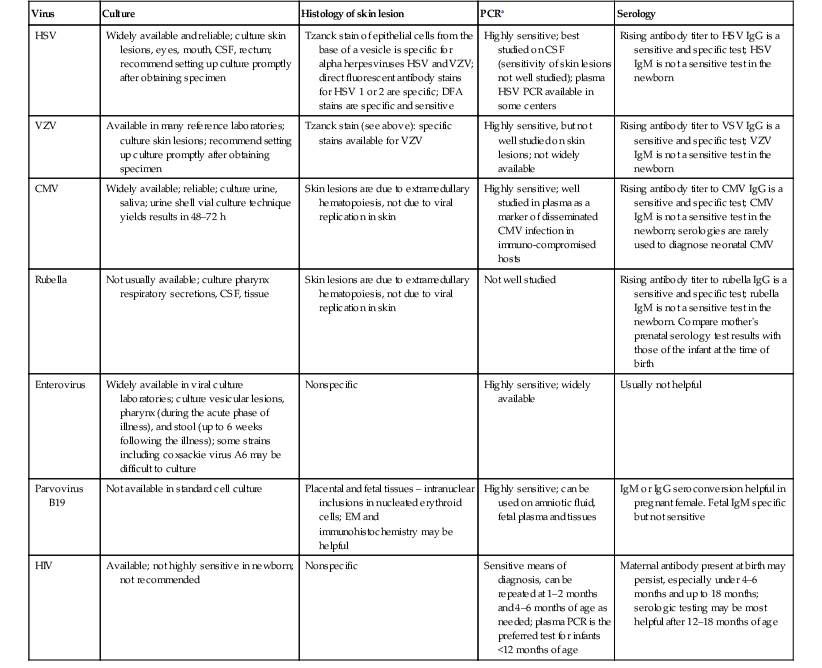
Diagnosis
Virus
Culture
Histology of skin lesion
PCRa
Serology
HSV
Widely available and reliable; culture skin lesions, eyes, mouth, CSF, rectum; recommend setting up culture promptly after obtaining specimen
Tzanck stain of epithelial cells from the base of a vesicle is specific for alpha herpesviruses HSV and VZV; direct fluorescent antibody stains for HSV 1 or 2 are specific; DFA stains are specific and sensitive
Highly sensitive; best studied on CSF (sensitivity of skin lesions not well studied); plasma HSV PCR available in some centers
Rising antibody titer to HSV IgG is a sensitive and specific test; HSV IgM is not a sensitive test in the newborn
VZV
Available in many reference laboratories; culture skin lesions; recommend setting up culture promptly after obtaining specimen
Tzanck stain (see above): specific stains available for VZV
Highly sensitive, but not well studied on skin lesions; not widely available
Rising antibody titer to VSV IgG is a sensitive and specific test; VZV IgM is not a sensitive test in the newborn
CMV
Widely available; reliable; culture urine, saliva; urine shell vial culture technique yields results in 48–72 h
Skin lesions are due to extramedullary hematopoiesis, not due to viral replication in skin
Highly sensitive; well studied in plasma as a marker of disseminated CMV infection in immuno-compromised hosts
Rising antibody titer to CMV IgG is a sensitive and specific test; CMV IgM is not a sensitive test in the newborn; serologies are rarely used to diagnose neonatal CMV
Rubella
Not usually available; culture pharynx respiratory secretions, CSF, tissue
Skin lesions are due to extramedullary hematopoiesis, not due to viral replication in skin
Not well studied
Rising antibody titer to rubella IgG is a sensitive and specific test; rubella IgM is not a sensitive test in the newborn. Compare mother’s prenatal serology test results with those of the infant at the time of birth
Enterovirus
Widely available in viral culture laboratories; culture vesicular lesions, pharynx (during the acute phase of illness), and stool (up to 6 weeks following the illness); some strains including coxsackie virus A6 may be difficult to culture
Nonspecific
Highly sensitive; widely available
Usually not helpful
Parvovirus B19
Not available in standard cell culture
Placental and fetal tissues – intranuclear inclusions in nucleated erythroid cells; EM and immunohistochemistry may be helpful
Highly sensitive; can be used on amniotic fluid, fetal plasma and tissues
IgM or IgG seroconversion helpful in pregnant female. Fetal IgM specific but not sensitive
HIV
Available; not highly sensitive in newborn; not recommended
Nonspecific
Sensitive means of diagnosis, can be repeated at 1–2 months and 4–6 months of age as needed; plasma PCR is the preferred test for infants <12 months of age
Maternal antibody present at birth may persist, especially under 4–6 months and up to 18 months; serologic testing may be most helpful after 12–18 months of age
Differential diagnosis
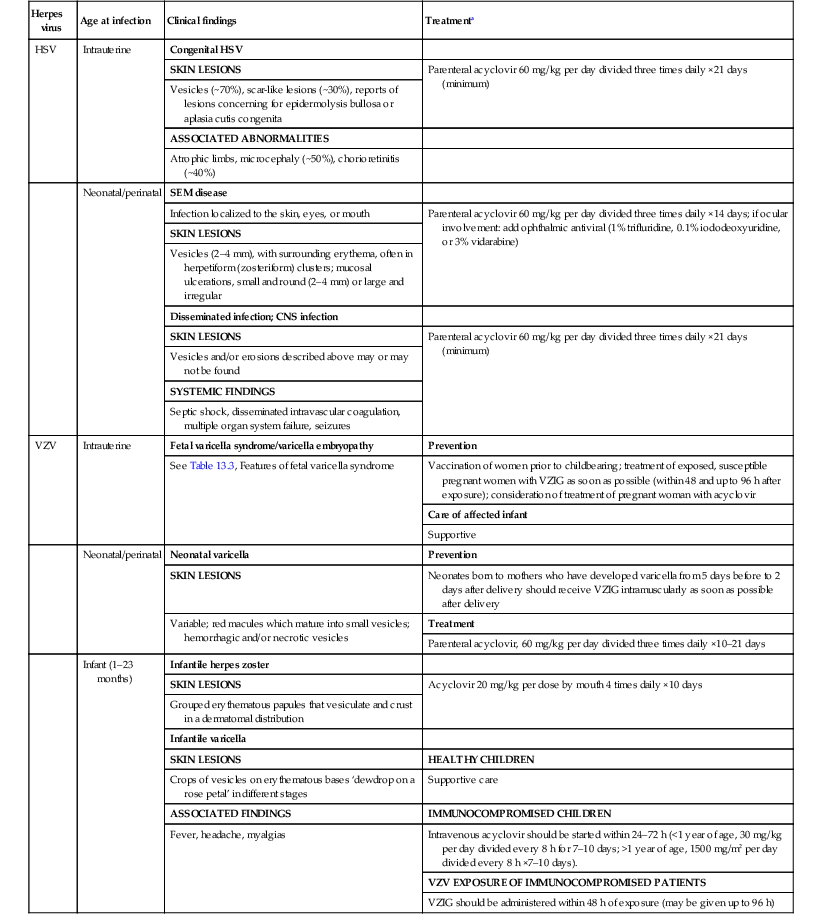
Management and prognosis
Herpes virus
Age at infection
Clinical findings
Treatmenta
HSV
Intrauterine
Congenital HSV
SKIN LESIONS
Parenteral acyclovir 60 mg/kg per day divided three times daily ×21 days (minimum)
Vesicles (~70%), scar-like lesions (~30%), reports of lesions concerning for epidermolysis bullosa or aplasia cutis congenita
ASSOCIATED ABNORMALITIES
Atrophic limbs, microcephaly (~50%), chorioretinitis (~40%)
Neonatal/perinatal
SEM disease
Infection localized to the skin, eyes, or mouth
Parenteral acyclovir 60 mg/kg per day divided three times daily ×14 days; if ocular involvement: add ophthalmic antiviral (1% trifluridine, 0.1% iododeoxyuridine, or 3% vidarabine)
SKIN LESIONS
Vesicles (2–4 mm), with surrounding erythema, often in herpetiform (zosteriform) clusters; mucosal ulcerations, small and round (2–4 mm) or large and irregular
Disseminated infection; CNS infection
SKIN LESIONS
Parenteral acyclovir 60 mg/kg per day divided three times daily ×21 days (minimum)
Vesicles and/or erosions described above may or may not be found
SYSTEMIC FINDINGS
Septic shock, disseminated intravascular coagulation, multiple organ system failure, seizures
VZV
Intrauterine
Fetal varicella syndrome/varicella embryopathy
Prevention
See Table 13.3, Features of fetal varicella syndrome
Vaccination of women prior to childbearing; treatment of exposed, susceptible pregnant women with VZIG as soon as possible (within 48 and up to 96 h after exposure); consideration of treatment of pregnant woman with acyclovir
Care of affected infant
Supportive
Neonatal/perinatal
Neonatal varicella
Prevention
SKIN LESIONS
Neonates born to mothers who have developed varicella from 5 days before to 2 days after delivery should receive VZIG intramuscularly as soon as possible after delivery
Variable; red macules which mature into small vesicles; hemorrhagic and/or necrotic vesicles
Treatment
Parenteral acyclovir, 60 mg/kg per day divided three times daily ×10–21 days
Infant (1–23 months)
Infantile herpes zoster
SKIN LESIONS
Acyclovir 20 mg/kg per dose by mouth 4 times daily ×10 days
Grouped erythematous papules that vesiculate and crust in a dermatomal distribution
Infantile varicella
SKIN LESIONS
HEALTHY CHILDREN
Crops of vesicles on erythematous bases ‘dewdrop on a rose petal’ in different stages
Supportive care
ASSOCIATED FINDINGS
IMMUNOCOMPROMISED CHILDREN
Fever, headache, myalgias
Intravenous acyclovir should be started within 24–72 h (<1 year of age, 30 mg/kg per day divided every 8 h for 7–10 days; >1 year of age, 1500 mg/m2 per day divided every 8 h ×7–10 days).
VZV EXPOSURE OF IMMUNOCOMPROMISED PATIENTS
VZIG should be administered within 48 h of exposure (may be given up to 96 h)
HSV in children beyond the neonatal period

 ). They may result from autoinoculation or inoculation from another infected individual. Genital lesions can also occur in young children with vesicular and eroded lesions, but should always raise concern for sexual abuse.
). They may result from autoinoculation or inoculation from another infected individual. Genital lesions can also occur in young children with vesicular and eroded lesions, but should always raise concern for sexual abuse.
Eczema herpeticum
Varicella
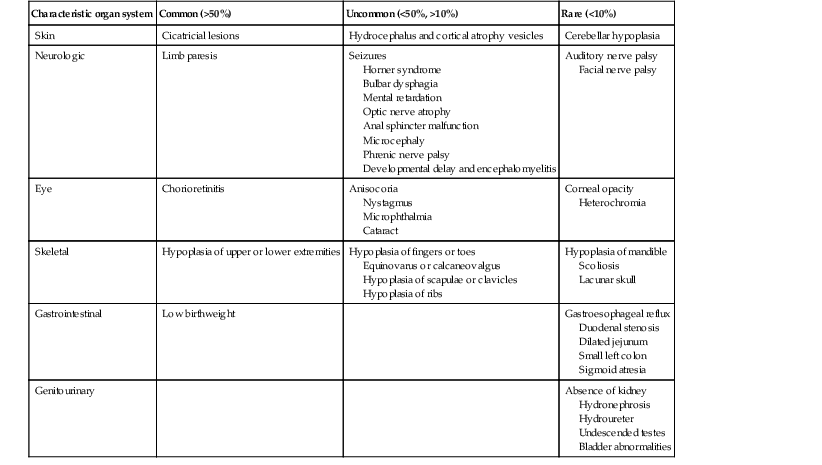
Fetal varicella syndrome
Cutaneous findings
Extracutaneous findings
Etiology and pathogenesis
Diagnosis
Treatment
Neonatal varicella
Cutaneous findings
Extracutaneous findings
Etiology and pathogenesis
Diagnosis
Treatment
Special concerns for the neonatal nursery and intensive care unit
Varicella exposure in the neonatal intensive care unit.
Infantile herpes zoster
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Viral Infections
13