Vertical Rectus Abdominis Flap for Perineal Reconstruction
Dhivya R. Srinivasa
Jeffrey H. Kozlow
DEFINITION
Perineal reconstruction is often required after oncologic resections for anorectal, gynecologic, and/or genitourinary tumors. Other etiologies including inflammatory bowel disease (IBD), trauma, and necrotizing infections can also be treated in a similar fashion after control of the destructive process.
The defect can be defined in two components: the internal pelvic outlet defect and the external skin/soft tissue defect.
Because radiation therapy is an integral component of locoregional tumor management, the surgeon must consider the implications of radiation.
Although multiple options are available to the reconstructive surgeon, a pedicled vertical rectus abdominis myocutaneous (VRAM) flap is one of the workhorse flaps for reconstruction of the perineum. The VRAM flap allows for harvest of varying combinations of the muscle, fascia, subcutaneous fat, and skin with tailoring of components to the acquired defect. The soft tissues of the VRAM are robust and reliable in anatomy, making this an attractive option for many reconstructive surgeons.
ANATOMY
The surgeon must be well learned in pelvic and perineal anatomy including the following components:
Genitourinary: Bladder, seminal vesicles, and prostate
Gynecologic: Ovaries, uterus, cervix, and vagina
Colorectal: Rectum, levator muscles, and anus
FIG 1 depicts a sagittal schematic of the male and female pelvis.
In colorectal and perianal resections, the presence or absence of the levator musculature following extirpation can determine the need for pelvic outlet volume to fill the defect and close the pelvic floor. Removal of all the soft tissue in the pelvic outlet will result in a defect that will not collapse down due to the surrounding bony architecture, resulting in postresection “dead space.”
The abdomen is a readily available donor site for perineal reconstruction. It is remote from the zone of radiation, has a pedicle that originates close to the pelvis, and commonly has lax soft tissue.
In most cases of perineal reconstruction, the donor site can be closed primarily. Component separation is a useful adjunct if needed to facilitate tension-free primary fascial closure.1
The VRAM flap derives blood supply from the deep inferior epigastric artery (DIEA), a branch of the external iliac arterial system as depicted in FIG 2. Dissection of the flap pedicle into the pelvis provides maximal arc of rotation. The DIEA and venae comitantes are predictably located on the underside of the rectus muscle, exiting into the pelvis along the lateral aspect of the muscle.
PATHOGENESIS
Resection of anorectal and urogenital tumors is most often the impetus for perineal reconstruction. Although staging and management can be complex, a significant portion of these tumors undergo surgical therapy along with radiation for curative intent.
The use of neoadjuvant radiation portends approximately a 60% risk of complications including abscess, wound dehiscence, and enterocutaneous fistula. The introduction of vascularized, nonradiated tissue to the surgical site can significantly decrease the risk of major complications.2
Subsequent systematic reviews and meta-analyses have confirmed the benefits of local tissue transfer for perineal reconstruction.3
In female patients, rectal tumors can also invade the posterior vagina requiring an even more complex reconstruction following extirpation. An example of this type of defect is pictured in FIG 3.
Anal tumors are treated primarily with the Nigro protocol, of which radiation is a key component. However, salvage of recurrent disease requires abdominoperineal resection with a wide skin margin resulting in a more significant external defect. Primarily closing the perineal defect is often wrought with complications due to tension, pressure, and radiation injury. Thus, soft tissue reconstruction with regional flaps can improve wound healing and decrease complications.4
Primary vulvar and vaginal tumors present similar challenges as do anorectal tumors but also require consideration of a functional reconstruction. Vulvar and vaginal tumors can be resected sans radiation, but locally advanced tumors, high-risk tumors, and positive margins can be treated with external beam radiation. Specifically for vulvovaginal reconstruction, restoration of appearance and function has quality of life benefits in addition to decreased wound healing complications.5,6
IBD, namely Crohn disease, can present with fistulas and recurrent abscesses.
Recalcitrant disease that fails medical management is often treated surgically, and abdominoperineal resection is reserved for a severe disease affecting quality of life.
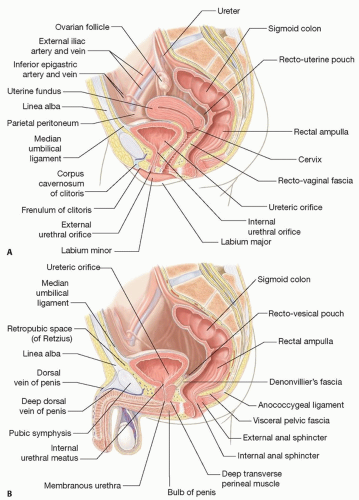
FIG 1 • A. Sagittal view of female anatomy. B. Sagittal view of male anatomy.
Inherently, these patients are high risk for wound complications. Most have been on chronic immunosuppressive therapy with corticosteroids and other immune modulators. Further, the tissue has been inflamed for years, with notable friability.
The introduction of healthy vascular tissue improves wound healing and decreased incidence of major complications.7
Other etiologies for perineal defects include trauma and necrotizing infections, which require full debridement of nonviable tissue prior to reconstruction.
PATIENT HISTORY AND PHYSICAL FINDINGS
Perineal reconstruction can be performed for a multitude of indications, and a thorough history should include pertinent information to each of these conditions.
Prior to deciding on a reconstructive plan, the following information should be obtained.
Extent of planned defect focusing critically on:
Amount of external skin resection
Maintenance or resection of the levator complex
Vaginal involvement in anorectal tumors
Presence of fistulas, which may require extended resection margins
History of radiation or planned adjuvant radiation therapyRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree