19
Vasculitis
• Cutaneous vasculitides are classified based on the size of the vessels affected, which determines the morphology of the skin lesions (Table 19.1).
Table 19.1
Classification of cutaneous vasculitis.
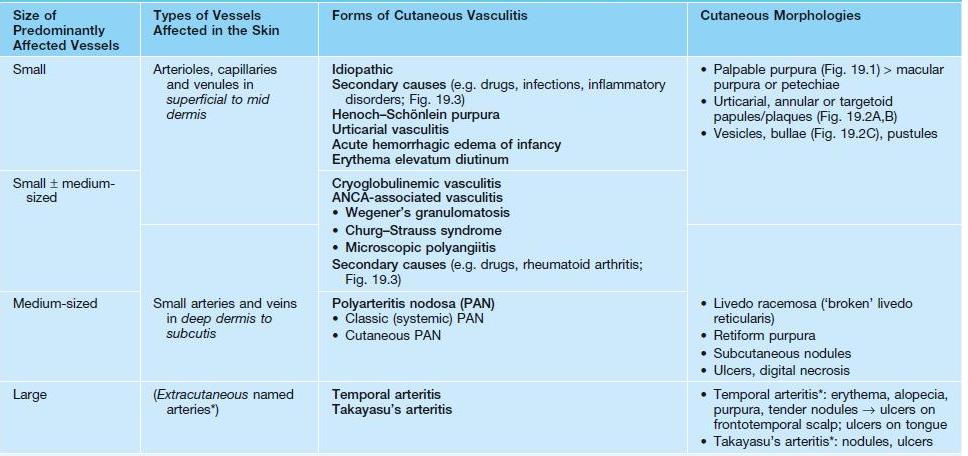
* Cutaneous involvement is uncommon.
ANCA, antineutrophil cytoplasmic antibodies.
• Favors adults but can occur at any age; HSP accounts for the majority of cases in children.
Cutaneous Small Vessel Vasculitis (CSVV)
• The clinical hallmark of CSVV is palpable purpura – nonblanching red-purple papules that favor dependent sites and areas of trauma (Koebner phenomenon) or pressure (e.g. from tight clothing); however, lesions often begin as partially blanching urticarial papules or purpuric macules, and occasionally other morphologies may be observed (e.g. vesicles or pustules; see Table 19.1, Figs. 19.1 and 19.2); frequently asymptomatic but can have associated pruritus, burning, or pain.



Fig. 19.1 Cutaneous small vessel vasculitis. A Classic presentation of purpuric papules on the distal lower extremities; a few lesions have become vesicular. B Early lesions may be pink papules. C Central necrosis with formation of hemorrhagic crusts. A, Courtesy, Kalman Watsky, MD; C, Courtesy, Frank Samarin, MD.



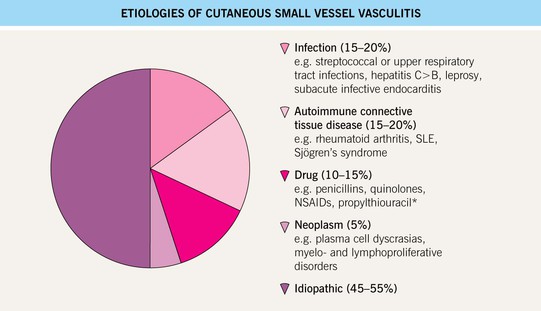
• Possible underlying conditions are presented in Figs. 19.3 and 19.4.


• Characterized by the histologic finding of leukocytoclastic vasculitis (LCV) – transmural infiltration of postcapillary venules by neutrophils that undergo fragmentation (leukocytoclasia), leading to fibrinoid necrosis of the vessel walls (see Fig. 1.11).
• DDx: specific CSVV subtypes or systemic vasculitides (see Table 19.1 and below), morbilliform drug eruptions or arthropod bites (with hemorrhage in dependent sites), petechial viral exanthems (see Fig. 68.1), pigmented purpura, erythema multiforme, pityriasis lichenoides, septic emboli.
• Rx: eliminate possible triggers, evaluate for systemic involvement (see Fig. 19.14), and provide supportive care (e.g. leg elevation, NSAIDs); for more severe or persistent (e.g. >4 weeks) skin disease, oral dapsone ± colchicine; if rapidly progressive or ulcerating, a 4- to 6-week course of prednisone may be considered.
Henoch–Schönlein Purpura (HSP)
• Form of CSVV characterized by prominent vascular IgA deposition, which is evident via DIF of a skin biopsy specimen (see Fig. 23.2); favors children <10 years of age, often presenting 1–2 weeks after an upper respiratory tract infection (URI).
• Urticarial papules evolve into palpable purpura, occasionally progressing to bullous or necrotic lesions (Fig. 19.5); typically involves the buttocks and lower extremities, but may be more widespread.


Fig. 19.5 Henoch–Schönlein purpura. A Multiple pink, partially blanching papules on the lower extremities. B More developed lesions with central necrosis.
•






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


