Chapter 18 Use of the Transtibial Technique to Avoid Posterior Cruciate Ligament and Roof Impingement of an Anterior Cruciate Ligament Graft
Definition, Complications, and Diagnosis of Posterior Cruciate Ligament Impingement
PCL impingement occurs when the ACL graft wraps around the PCL as the knee is flexed. Impingement of the ACL graft around the PCL causes a tension rise in flexion that either limits flexion or stretches the ACL graft, resulting in anterior instability. Not widening the notch and malplacement of the ACL graft in the coronal plane cause PCL impingement in the transtibial technique.1–3
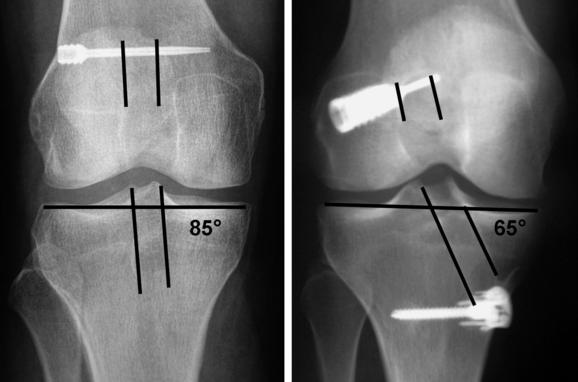
PCL impingement can be suspected if bone was not removed from the lateral femoral condyle (i.e., a wallplasty) until the space between the PCL and lateral femoral condyle exceeded the width of the ACL graft by 1 mm. An anteroposterior (AP) radiograph is diagnostic of PCL impingement when the tibial tunnel is at an angle greater than 70 degrees with respect to the medial joint line or when the lateral edge of the tibial tunnel is medial to the apex of the lateral tibial spine2 (Fig. 18-1). Magnetic resonance imaging (MRI) with three-dimensional (3D) reconstruction is diagnostic of PCL impingement when there is no space between the ACL graft and PCL or when the ACL graft does not run straight and is deformed by the PCL.1 Arthroscopy is diagnostic of PCL impingement when there is no space between the ACL graft and PCL at the apex of the notch and when the ACL graft is slack and bows laterally with the knee in 30 degrees of flexion.3 Surgeons who avoid PCL impingement will find that their patients have better knee flexion and better anterior and rotatory stability.1,2
Definition, Complications, and Diagnosis of Roof Impingement
Roof impingement occurs when the intercondylar roof contacts the ACL graft before the knee reaches full extension. Impingement of the ACL graft against the intercondylar roof causes either a loss of extension or a stretching out of the graft from abrasion, resulting in anterior instability. The cause of roof impingement is malplacement of the ACL graft in the sagittal plane. Placing the tibial tunnel anterior to the intercondylar roof with the knee in maximal extension causes roof impingement.4–7
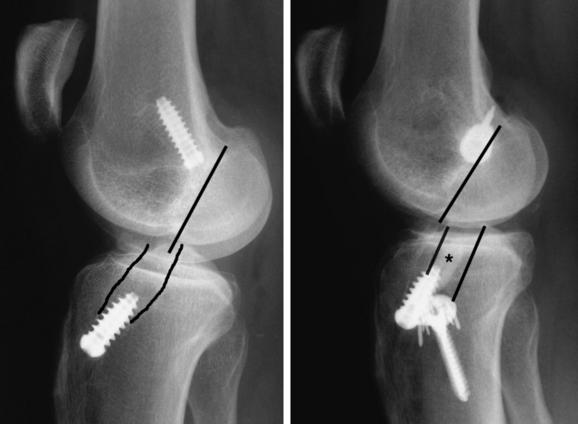
A lateral radiograph of the knee in maximal extension is diagnostic of roof impingement when the tibial tunnel is anterior to the intercondylar roof (Fig. 18-2). The lateral radiograph is less helpful in evaluating a bone–patellar tendon–bone graft than a soft tissue graft because the bone plug may obscure the wall and orientation of the tibial tunnel and because the tendon does not fill the bone tunnel.7 An MRI is diagnostic of roof impingement when the pathognomonic regionalized signal increase occurs in the graft, which is confined to the distal two-thirds of the ligament within the intercondylar notch. The portion of the ACL graft in the tibial and femoral tunnel and the portion of the graft that exits the femoral tunnel retain a low signal, which is identical to the PCL and patellar tendon.8–10 Arthroscopy is diagnostic of roof impingement when the ACL graft is frayed or a fibrous nodule is formed at the entrance of the tibial tunnel into the notch.11 Surgeons who avoid roof impingement will find that their patients have better knee extension and stability.7,12
The Tibial Tunnel: The Key Tunnel in the Transtibial Technique
The advantage of the transtibial technique is that when the notch is widened and the tibial tunnel is placed correctly in the coronal and sagittal plane, the correct placement of the femoral tunnel is automatic. The reason for this is that the position of the over-the-top femoral aimer and the position of the reamer are both controlled by the tibial tunnel.3 If the notch is not widened and the tibial tunnel is placed incorrectly in either the coronal or sagittal plane, then the femoral tunnel will be placed incorrectly and the patient will suffer from motion loss or instability.1,2,7
The feasibility of the transtibial technique to replicate the tension pattern of the intact ACL was determined by a cadaveric study that analyzed the effect of varying the angle of the tibial tunnel (and femoral tunnel) in the coronal plane on the tension pattern of the ACL graft (Fig. 18-3). Drilling the tibial tunnel at an angle of 60 degrees in the coronal plane placed the ACL graft far down the side wall of the notch away from the PCL, and the tension in the graft matched the intact ACL. Drilling the tibial tunnel at 70 and 80 degrees placed the ACL graft near the apex of the notch and the PCL, and the tension increase in the ACL graft with knee flexion was subsequently abolished by incremental excision of 2 to 6 mm of the lateral edge of the PCL. Therefore, the cause of the abnormal tension rise in flexion is the premature mechanical impingement of the ACL graft on the PCL during flexion and is avoided by placing the tibial tunnel at an angle less than 70 degrees.3
Related posts:
 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
 Proprioception and Anterior Cruciate Ligament Reconstruction
Proprioception and Anterior Cruciate Ligament Reconstruction
 Anterior Cruciate Ligament Reconstruction Utilizing the Rigidfix for Femoral-Sided Fixation
Anterior Cruciate Ligament Reconstruction Utilizing the Rigidfix for Femoral-Sided Fixation
 Revision Anterior Cruciate Ligament Reconstruction Using Autologous Hamstring Tendons
Revision Anterior Cruciate Ligament Reconstruction Using Autologous Hamstring Tendons
 High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
 Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


