Facial paralysis severely impacts a person’s ability to interact with the world. Advances in microsurgery, especially free neurotized muscle transfers, have greatly improved reanimation outcomes. The gracilis free muscle transfer, introduced in 1971, is the most widely used procedure for long-standing flaccid paralysis. This review covers recent innovations in gracilis reanimation, including vector design and neurotization options, and introduces the free strap muscle for dynamic facial reanimation.
Key points
- •
The gracilis free muscle transfer (GFMT) remains the most widely used technique for dynamic reanimation in long-standing facial paralysis with muscle atrophy.
- •
GFMT provides a consistent, safe, and reliable mean to restore oral commissure excursion with smiling, in the hands of an experienced surgeon.
- •
Cross-facial nerve grafts and masseteric nerve transfer are the most commonly utilized donor nerves, in isolation or together, for reinnervation of the free muscle transfer.
- •
Advances in vector design of free muscle transfers have improved the natural appearance of smiling in postsurgical patients.
Introduction
One of the most integral parts of human communication and facial expression is the smile. Facial paralysis can have devastating consequences on individuals’ ability to smile, produce articulate speech, oral competence, and has been shown to increase rates of depression, social anxiety, and reduce quality of life (QOL) measures. , Thus, surgical procedures for smile restoration have become an important topic of discussion. Static procedures to improve facial symmetry have been implemented for many years. However, the last decade has seen an increase in research on dynamic procedures aimed at improving facial movement. These include nerve reanastomosis, cable grafting, motor nerve transposition, or muscle transfers. Advances in microsurgical technology and technique over the last 50 years have further expanded surgeons’ abilities to restore facial movement, particularly in the subset of patients with long-standing paralysis and muscle atrophy. This study will focus on microvascular techniques used for dynamic facial reanimation.
The first description of free tissue transfer for facial reanimation was by Thompson in 1971 in which he used the palmaris longus and extensor digitorum brevis muscles as a free muscle graft without any nerve or blood supply in 8 patients. A small number of patients developed muscle contraction but the grafts were eventually found to atrophy and fibrose. Harii then performed the first microvascular transfer of the gracilis muscle in 1976 in a single-stage manner while using the superficial temporal vessels for blood supply and deep temporal nerve for reinnervation. Obrien and Manktelow then further expanded on this study in the early 1980s by performing a gracilis free tissue transfer in a 2 stage approach utilizing a cross-facial nerve graft (CFNG) for reinnervation. At the time, there were significant issues with muscle bulk. Manktelow described the fascicular territories of the gracilis in 1985 to allow for debulking. Debulking the muscle has now been truly refined over the last decade. A number of other donor muscles have been described in search for the most ideal and effective method for dynamic facial reanimation including extensor digitorum brevis in microvascular manner, pectoralis minor, latissimus dorsi, sternohyoid muscle alone, omohyoid muscle alone, serratus anterior, and most recently, a sterno-omohyoid composite muscle free flap. However, the gracilis muscle remains the most widely used donor option for free muscle transfer in facial reanimation primarily due to its reliability of the neurovascular pedicle, limited donor site morbidity, and strong contractile muscle force.
In this study, we will describe the advances in gracilis free muscle transfer (GFMT) for smile reanimation including innervation options, multivector design, and lower lip reanimation. Additionally, we will describe more recent publications in the use of strap muscles as free muscles for smile reanimation.
Discussion
Gracilis Free Muscle Transfer
The gracilis muscle is a long, thin, slow-twitch, muscle of the thigh that adducts and medially rotates the leg. It typically ranges between 4 and 6 cm in width, up to 25 cm in length, and the neurovascular pedicle consistently enters the muscle proximally approximately 8 to 10 cm caudal from the pubic tubercle. The average preharvest length is 14 cm while the average inset length is 10 to 11 cm. The gracilis tendon is not typically included in the harvest. There is a dominant musculocutaneous perforator at this location should skin be required. The gracilis has a type II vascular pattern according to the Mathes and Nahai classification system. The dominant pedicle is a terminal branch of the adductor artery, which arises from the profunda femoris, but it can also arise from the medial femoral circumflex artery. This runs between the adductor longus muscle anteriorly and the adductors brevis and magnus posteriorly. It typically enters the gracilis at the junction between the proximal one-third and distal two-thirds of the muscle. Perforators to the other adductor muscles must be ligated in order to obtain adequate length, which is typically 6 cm in length and 2 mm in arterial diameter. The major artery is accompanied by 2 vena comitantes that may or may not join into 1 vein and these drain into the profunda femoris vein. Their diameter can range from 1.5 to 2.5 mm. The vascular supply of the muscle itself is typically very reliable; however, the skin perforators can vary. It is important to always stay vigilant during pedicle dissection as anatomic variations may be encountered, such as multiple arteries supplying the muscle ( Fig. 1 ).
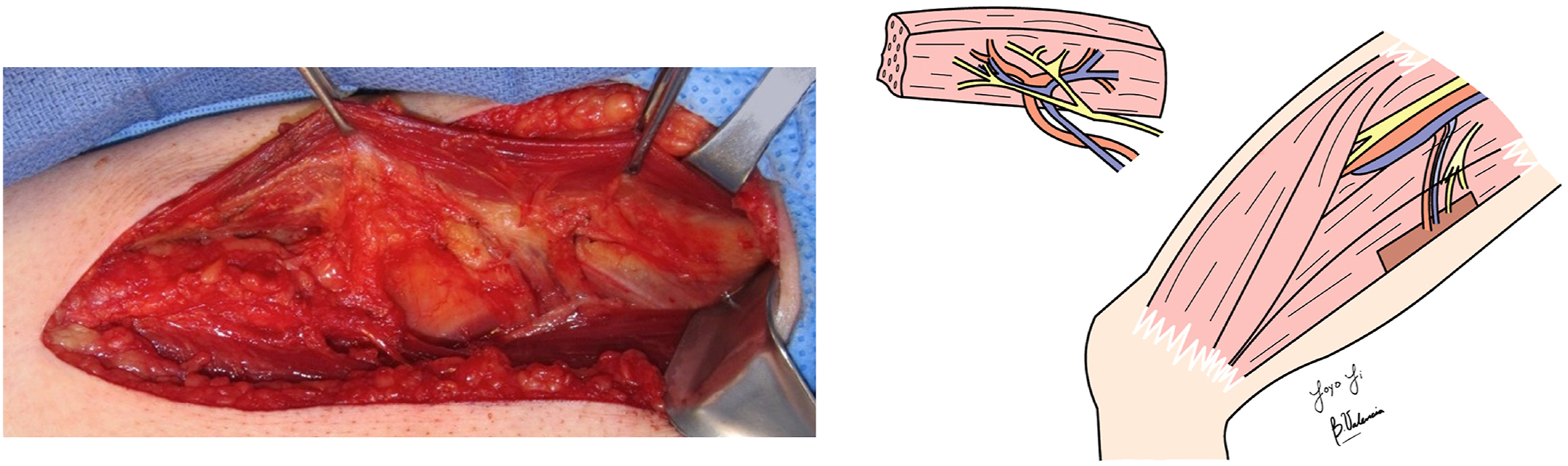
The motor input to the gracilis muscle is from the anterior branch of the obturator nerve, which runs in an oblique path to enter the muscle 2 to 3 cm cephalad from the vascular pedicle (see Fig. 1 ). This may be traced proximally between the adductor longus and brevis to achieve an increased length.
An important factor in muscle harvest is the transferred muscle weight, as this can be a surrogate for the motor units transferred in each segment. The transferred gracilis muscle typically weighs anywhere from 10 to 30 g, depending on the amount of muscle debulked. Recent studies have reported their average gracilis muscle weight to be around 30 g , ; however, weights at higher volume centers are generally closer to 15 g or less. It is important to note that while debulking may be more esthetically pleasing for facial contour, it can also decrease the number of motor units and compromise smile excursion. In contrast, the reinnervated muscle retains its bulk over time rather than atrophying like noninnervated muscle flaps. This retained bulk can be disconcerting to patients, especially those with thin faces.
Overall, the outcomes from GFMT have been shown to be reliable and consistent, making it the most commonly used donor muscle for free tissue transfer in facial reanimation. Two recent meta-analyses examining the efficacy of the GFMT have shown a resultant pooled mean oral commissure excursion of 7 to 7.5 mm, regardless of donor nerve used. , The studies also indicate a low flap failure rate, 2.9%, suggesting a significant improvement in smile with low rates of revision.
Innervation Options for Gracilis Free Muscle Transfer
A critical aspect of free muscle transfer for smile reanimation is the choice of donor motor nerve for innervation of the free flap ( Table 1 ). As previously mentioned, the original description of the GFMT in 1976 reported the use of the deep temporal nerve. While this choice has been largely abandoned, there is currently no universal consensus on the one donor nerve that supersedes all others. The most commonly described donor motor nerves are the cross-face nerve graft, masseteric nerve graft, and a combination of both. More rarely, either a hypoglossal nerve graft or spinal accessory nerve (SAN) graft may be used.
| Nerve | Donor Source | Advantages | Disadvantages | Notes |
|---|---|---|---|---|
| Most commonly used options | ||||
| Cross-facial (CFNG) | Contralateral midface branch of CNVII, with a long cable graft most commonly sural nerve, but can also be median antebrachial cutaneous nerve | Spontaneity | Lower reliability in oral commissure excursion, if used in isolation requires 2 stage procedures with 6 mo in between | 75% of GFMT patients innerved with a CFNG had spontaneous smiling compared with 20% of patients with solely masseteric nerve innervated GFMT. CFNG may also be sufficient for coaptation in children |
| Masseter | Ipsilateral branch of CNV | Strong, reliable oral commissure excursion, faster time to onset of GFMT movement, can be done as single stage | Lack of spontaneity, patient needs to activate by biting down | In 154 GFMT patients undergoing innervation by masseteric nerve alone, Bhama et al found a mean of 2.2 mm greater oral commissure excursion than those innervated by the contralateral facial nerve (8.7 mm vs 6.5 mm). Similarly, Bae et al found oral commissure excursion in masseteric nerve transfer was 14.2 mm compared to 7.9 mm for CFNG in a series of 166 children undergoing GFMT |
| Dual innervation with CFNG and ipsilateral nerve to masseter | Ipsilateral trigeminal branch of CNV and CFNG with cable graft coapted from contralateral midface branch of CNVII (most commonly sural nerve cable graft) | Combines spontaneity of the CFNG with reliable power of the masseteric nerve transfer | Typically performed in 2 satges, more recently being performed in a single stage | Retrospective case-control comparing single-stage innervation GFMT cases with either CFNG or the masseteric nerve alone vs 25 dually innervated (CFNG plus masseteric nerve) GFMT cases The study found that spontaneity in dually innervated patients (33%) was higher than in patients with the masseter alone (20%) but lower than in those with CFNG alone (75%) ( P > .05) |
| Cross-masseter with our without CFNG | Contralateral midface branch of CNVII and contralateral trigeminal branch of CNV both into a single cable graft | — | Must be a 2 stage procedures with 6 mo in between | A 2022 study of 8 patients found that when smiling and biting simultaneously the oral commissure excursion was greater than with the activation of each individual component. In spontaneous smile, the authors found commissure excursion to be higher than that provided by only the facial nerve (smile only) in most adult patients treated |
| Less commonly used options | ||||
| SAN | Ipsilateral CNXI | High axon count, single stage | Trapezius and shoulder weakness and pain | Reserved for settings where other nerve options are unavailable |
| Hypoglossal nerve | Ipsilateral CNXII | Single stage, high axon count | Possible hemilingual weakness and atrophy, short length can necessitate cable graft, which may reduce success | If utilized, a partial hypoglossal nerve donor will reduce morbidity |
Cross-facial nerve graft as innervation for free muscle transfer
The CFNG, which utilizes midfacial branches of the contralateral, unaffected, facial nerve, has the potential of creating a spontaneous and synchronous smile. However, it has lower reliability given its long course and less oral commissure excursion than other donor nerves. , ,
While the CFNG was originally described in 1971 as a single-stage procedure for facial reanimation, it was not popularized until 1976 when Harii and team utilized it in a 2 stage procedure to innervate a GFMT. The advantages conferred by the 2 stage procedure were secondary to increased axonal growth through the CFNG prior to coaptation with the GFMT. This allowed viable axons to be present in the distal end of the nerve graft prior to neurorrhaphy, thereby increasing effective innervation of the GFMT at the time of coaptation and decreasing the risk of denervation atrophy. Therefore, the CFNG procedure is commonly done in 2 stages. In the first stage, a donor graft is harvested, most commonly the sural nerve, and coapted to a donor facial nerve branch in the unaffected side of the face. Typically, a midfacial branch is chosen given the redundancy in innervation of the upper lip. It is imperative to choose a robust branch of the facial nerve to provide adequate donor axons to the CFNG. The polarity of the sural nerve was originally thought to make a difference in outcomes; however, it has been found that the donor sural nerve graft can be coapted from either end, paying attention to branching patterns. The chosen distal end of the CFNG is tunneled subcutaneously through the upper lip and out into the affected side of the face. Some surgeons choose to bury this end in the contralateral canine fossa to limit the length of the CFNG in an attempt to increase axonal growth in the distal end. Other surgeons choose to keep the donor graft long, depending on the intended future recipient target. The nerve is then allowed to grow through the cable graft. Timing for the second-stage procedure is typically 6 to 12 months after the initial stage in adults or 6 to 9 months in children. , A strong Tinel’s sign may indicate when the graft has sufficient axonal growth in the distal end. This is elicited by tapping the distal end of the CFNG resulting in an “electrical” or “pins and needles” sensation. In free muscle transfer (FMT), the second stage of the procedure, the distal end of the CFNG is freshened and coapted to the donor nerve from the free muscle graft.
Advantages of cross-facial nerve graft for innervation
An advantage of utilizing a CFNG for innervation of free muscle transfer is the ability to provide spontaneity of smile, coordinated with activation of the unaffected, contralateral, side of the face. , , It has been shown through videographic techniques that 75% of GFMT patients reinnervated with a CFNG had spontaneous smiling compared with 20% of patients with masseteric nerve innervated GFMT. Similarly, other studies directly comparing GFMT-innervated by CFNG to other innervation sources (hypoglossal, masseteric, and spinal accessory), found a significantly higher proportion of CFNG patients demonstrated spontaneous smile. ,
Disadvantages of cross-facial nerve graft for innervation
One drawback of using the CFNG as a donor nerve is its lower reliability when compared to other donor nerves. , , Bhama and colleagues looked at 127 cases of GFMT for smile reanimation in patients ranging from 6 to 80 years old. They observed that the CFNG innervation resulted in reduced oral commissure movement compared to the innervation by the masseteric nerve (6.5 ± 2.9 mm vs 8.7 ± 3.5 mm). It is important to note, children achieve better results with GFMT innervated by CFNG alone than adults. Another study by Hontanilla and Cabello examined 41 patients with an average age of 42 years who underwent GFMT with CFNG innervation. They found that these patients regained 5.1 mm of commissural elevation during a smile but noted that masseteric nerve-innervated GFMT yielded 40% more oral commissure movement compared to CFNG-innervated flaps. Ylä-Kotola and colleagues conducted a study involving 27 patients aged 7 to 65 years who underwent free tissue transfer innervated by only CFNG, with 11 of them undergoing GFMT. They discovered that 78% of the patients felt that their QOL had improved, while 22% believed that the reanimation had no noticeable effect and was correlated with decreased dynamic motion postoperatively.
Masseteric nerve as innervation for free muscle transfer
First described by Zuker and colleagues in 2000 for children undergoing smile reanimation for Moebius syndrome, the masseter nerve has been shown to provide consistent, strong, oral commissure excursion. Additionally, it has a relatively fast onset and only requires a single-stage surgery, making it a work-horse donor nerve.
The masseteric nerve arises from the anterior division of the mandibular branch of the trigeminal nerve, providing motor supply to the masseter muscle. Surgically, the nerve has been described in the subzygomatic triangle. This triangle is bounded by the ramus of the mandible posteriorly and the zygomatic arch superiorly. The nerve exits the foramen rotundum and courses in a diagonal to the masseter muscle, bisecting this triangle. The nerve can usually be found within the masseter muscle about 1 cm inferior to the arch and 3 cm anterior to the tragus. It typically courses obliquely with respect to the muscle, or parallel to the zygomatic arch, and can be located in the middle of the muscle belly about 10 to 15 mm deep to the parotidomasseteric fascia.
Advantages of masseteric nerve innervation
The primary advantage of innervation with the masseteric nerve lies in its ability to give strong, reliable, oral commissure excursion in smile, especially when compared to CFNG alone. , , In 154 GFMT patients undergoing innervation by masseteric nerve alone, Bae and colleagues found a mean of 2.2 mm greater oral commissure excursion than those innervated by the contralateral facial nerve (8.7 vs 6.5 mm). Similarly, Bae and colleagues found oral commissure excursion in masseteric nerve transfer was 14.2 mm compared to 7.9 mm for CFNG in a series of 166 children undergoing GFMT.
The masseteric nerve also has a faster onset of movement than other donor nerves. The CFNG have been reported to take up to 2 years to show full effect, while masseteric nerves have been shown to function as early as 3 to 6 months postoperatively. , Additionally, GFMT with masseteric nerve innervation can be done as a single-stage procedure, which is more ideal for patients with significant medical comorbidities, higher operative risk, or who desire results in a shorter time frame.
Disadvantages of masseteric nerve innervation
The primary disadvantage in using the masseteric nerve to drive a GFMT-powered smile is the lack of consistent spontaneity of movement. Smiling activated by the masseteric nerve primarily requires a voluntary biting or clenching action. Therefore, when an emotive smile is involuntarily elicited on the unaffected side, a natural-appearing smile on the GFMT side to match synchronously can be challenging and requires training and effort. While several studies have explored spontaneity with extensive facial physical therapy and motor training, the majority of patients has reported spontaneity only a small percentage of the time. ,
Dual innervation
Dual innervation of free muscle transfer for smile reanimation utilizes the strengths of various donor nerve sources while compensating for their respective limitations. The most prevalent dual innervation is the coupling of the masseteric nerve with the CFNG. This pairing offers the prospect of enhanced oral commissure excursion through the masseteric nerve and increased spontaneity via the CFNG. The challenge of understanding dual innervation outcomes is how to separate the contribution of each nerve and the need for large case series with rigorous postoperative assessment.
Dual Innervation with Cross-facial Nerve Graft and Masseteric Nerve
The first published data from dual innervation were for latissimus dorsi muscle transfer, using both the masseteric nerve and a CFNG. This was done in only a small number of patients but proven to provide movement through EMG and clinical outcomes data. , Subsequent clinical studies by Cardenas-Mejia, Mcneely, and Sforza found a vast majority of patients undergoing dual innervation of GFMT with masseteric and CFNG achieved spontaneous smile.
Dusseldorp conducted a retrospective case–control study to compare spontaneity in 24 single-stage innervation GFMT cases with either CFNG or the masseteric nerve alone versus 25 dually innervated (CFNG plus masseteric nerve) GFMT cases. This study was one of the first to objectively evaluate patient outcomes, utilizing video analyses of spontaneous laughter rather than clinician-rated static photos. It found that spontaneity in dually innervated patients (33%) was higher than in patients with the masseter alone (20%) but lower than in those with CFNG alone (75%), although no statistically significant difference was detected among the groups. Interestingly, when they compared objective evaluations spontaneity to clinician’s evaluations, clinicians were often wrong. There were no significant differences observed in oral commissure movement or eFACE scores among these groups.
While there are limited data comparing single-stage to 2 stage CFNG during dual innervation GFMT, the 2 stage approach ensures that the distal ends of both the masseteric nerve and CFNG contain viable axons at the time of coaptation to the GFMT. This theoretically allows for more synchronized innervation of motor units in the GFMT from both sources. However, some surgeon are performing dual innervation in a single-stage surgery. If this is found to yield comparable outcomes, it could eliminate the need for multiple operations and potentially expedite the restoration of smiles.
Dual Innervation with Cross-masseter Innervation of Gracilis Free Muscle Transfer
A relatively new technique is the use of a cross-masseter nerve to innervate the GFMT. A 2022 study of 8 patients utilized a single sural nerve to cross a contralateral facial nerve as well as the contralateral masseteric nerve. In the second stage of the surgery, typically 9 months later, the single distal tip of the CFNG was connected to the obturator nerve of a GFMT. The cross-masseter and cross-facial innervations were successful. When smiling and biting simultaneously, the authors found oral commissure excursion was greater than with the activation of each individual component. In spontaneous smile, the authors found commissure excursion to be higher than that provided by only the facial nerve (smile only) in most adult patients treated. Similarly, they found that in most patients, the excursion of smile without ipsilateral masseter activation was similar or slightly higher than that when patient activated the ipsilateral masseter alone. The authors suggest that the masseteric nerve works synergistically with the ipsilateral CFNG for smile activation. However, the physiologic basis of dual innervation remains incompletely understood. Deciphering the specific contributions of individual nerves is challenging, other teams have proposed that there could be a mechanistic competition between 2 innervating nerve sources, though this requires further investigation. Nevertheless, dual innervation for GFMT has exhibited promising results, justifying the continuation of research in this area.
Other donor nerve options: hypoglossal and spinal accessory nerve
In settings where a CFNG or masseteric nerve may not be possible, powering the GFMT with a hypoglossal or SAN coaptation is a viable option. These are reserved for specific situations given the morbidity compromising the donor nerve, potentially when the underlying condition compromises the trigeminal nerve, and it is, therefore, not available for use.
In GFMT innervated by SAN, 10 cm of the SAN are dissected and tunneled beneath the platysma muscle to reach the recipient site. The SAN has approximately 1400 axons available for innervation of the muscle transplant; however, it carries the donor site morbidity with ipsilateral trapezius weakness and shoulder pain. , The most robust study of SAN innervated GFMT followed 56 patients and found the majority of patients was able to achieve a full dental display with a smile after 6 to 12 months, and interestingly, the authors felt a comparable percentage had a spontaneous smile comparable to their cohort of patients undergoing GFMT innervated by a CFNG. However, due to high donor site morbidity, the SAN is rarely used, and surgeons that described the prior study have now adopted the use of the masseteric nerve.
While historically hypoglossal nerve transfers were associated with high donor site morbidity in the form of hemilingual atrophy and deviation leading to dysarthria and dysphagia, newer techniques involving partial nerve transfers and limited hypoglossal manipulation with the use of cable grafting have shown improved donor site outcomes. While it has been shown to provide adequate resting tone, the requirement of hypoglossal-driven GFMT voluntary contraction via tongue protrusion limits its spontaneity and utility. ,
Vectors in free muscle reanimation design
While powering the GFMT is vital to success, the vectors of distribution of smile action are equally as important in helping patients achieve a pleasant and symmetric smile. A Duchenne smile, or one of genuine pleasure, is characterized by increased upper-lateral dental display, upward excursion of the upper lip by muscles such as zygomaticus major, and contraction of the lower eyelid leading to wrinkling of the crow’s feet. On the contrary, a pleasant, or social, smile, like that of the Mona Lisa is created by lateral excursion of the oral commissure without increased upper lip dental display. In addition, a natural smile also activates the lower lip depressors, such as the depressor labii inferioris. Therefore, the vectors of muscle action on the mouth during smile are complex and free muscle transfer should ideally aim to recreate these naturally subtle vectors of movement. Surgeons must balance the goal of a multidimensional smile with the added soft tissue bulk that additional vectors of free muscle transfer may necessitate.
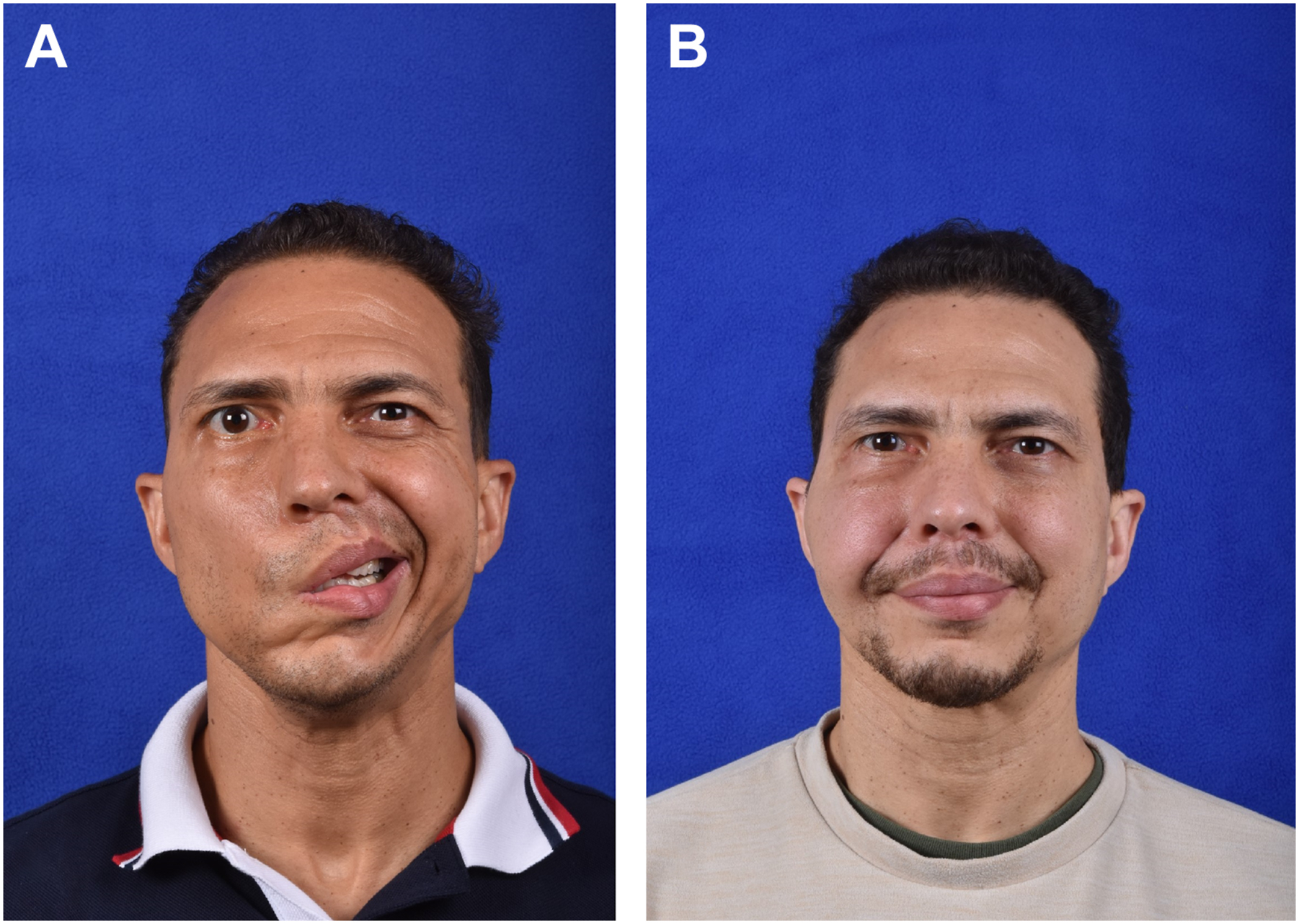
Single vector
In 2014, Bhama and colleagues published a 10 year review of 148 GFMT patient outcomes. Using one muscle paddle, this single-vector technique was placed from the modiolus of the mouth and inset onto periosteum at the temple. Using FACE-gram to quantify outcomes, they found a mean of 8 mm increase in smile excursion on the affected side, measured at the commissure, though dental display was not investigated. This single vector undoubtedly provides enhanced symmetry over the preoperative state; however, the smile was found to be more social in nature and less natural appearing ( Fig. 2 ).