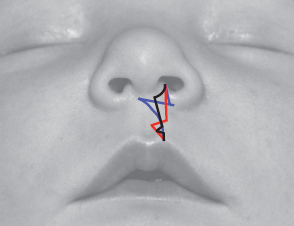
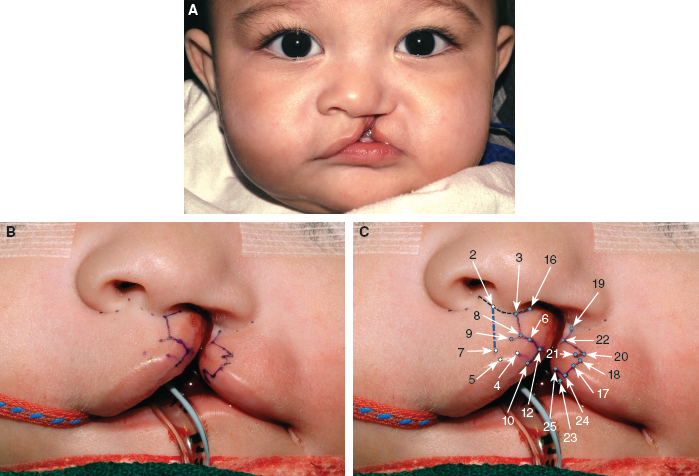
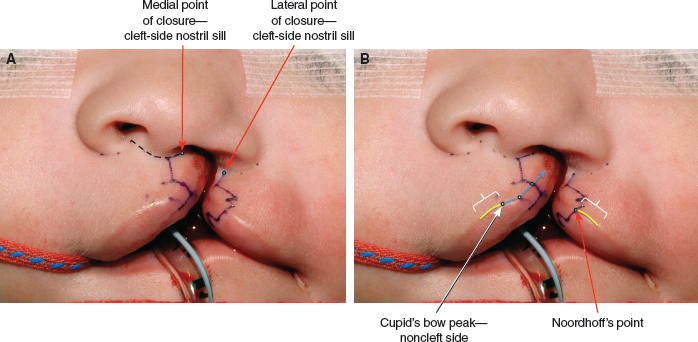
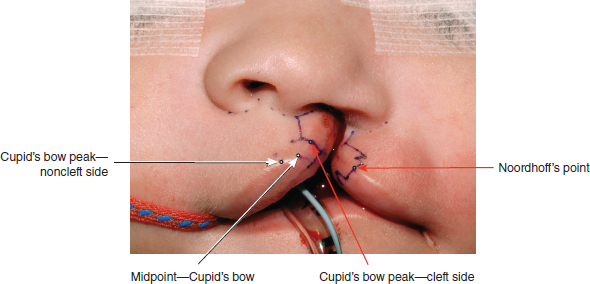
45 ○ The goal of the anatomic subunit approximation technique is to bring the medial and lateral lip elements together along the seams of anatomic subunits. ○ The anatomic subunit approximation technique is a modification of the Rose and Thompson repairs. In most cases it also incorporates a modification of the inferior triangle repair. ○ At the height of the lip, closure points in the nostril sill are chosen to achieve: – Nostril margins of equal circumference – Alar base symmetry from the anterior view ○ The noncleft side Cupid’s bow peak should be designed where the upward concavity of the bow meets the upward convexity of the lateral lip element. No corresponding upward convexity exists on the cleft side of the medial lip element. This convexity must come from the cleft side lateral lip lateral to Noordhoff’s point. ○ Medial and lateral lip roll elements approximate in an end-to-end fashion such that the subunit of the roll is not interrupted by a complex scar. ○ Tension of the repair is optimally positioned above the roll, thus accentuating the pout of the lip. ○ An inferior triangle is used when required. ○ Lateral lip element markings vary to accommodate the vertical height of the lateral lip element. ○ Noordhoff’s point should not be compromised. Lateral lip element transverse length need not be sacrificed to achieve vertical height. ○ The anatomic subunit approximation technique can be used in all cases of unilateral cleft lip. Dr. Samuel Noordhoff of the Chang Gung Memorial Hospital in Taipei, Taiwan, used a modification of Millard’s rotation-advancement repair; Dr. Hugh Thomson, at the Hospital for Sick Children in Toronto, Canada, performed a modification of the Randall-Tennison inferior triangle repair.1–6 Both of these highly skilled surgeons were able to achieve wonderful results, but there are drawbacks to each technique. Common to both of these repairs is the principle of medial lip element elongation using tissue from the lateral lip element. By incorporating the Rose-Thompson principle, achieving length by the approximation of curved or angled lines, the amount of tissue borrowed from the lateral lip can be reduced. Burget and Menick7 contributed the concept of anatomic subunits as it applies to nasal reconstruction. Other influences have probably contributed to the anatomic subunit approximation technique as well.8 Rotation-advancement repairs are “cut-as-you-go” techniques. If the original rotation incision is inadequate to achieve a balanced Cupid’s bow, the surgeon is obliged to consider a back-cut, which introduces additional scar and lowers the transverse limb of the repair. Similarly, if the leading edge of the advancement incision is too short, because the vertical height of the lateral lip element is short (often the case in complete clefts), length must be gained at the expense of lateral lip element transverse length. These maneuvers should be considered compromises. In contrast, the anatomic subunit approximation technique requires the surgeon to commit to a plan before incisions are made to achieve the end goals of balance, preservation of key landmarks, and respect for anatomic subunits. If carried out in the proper sequence, checkpoints along the way allow for evaluation and modification of the original plan to ensure that these goals are met. The anatomic subunit approximation technique is a modification of the Rose9 and Thompson10 repairs. In many cases it is also a modified inferior triangle repair. In contrast to the Thompson repair, the angles are positioned just above the cutaneous roll elements of the medial and lateral lip elements. The straight line repairs of Rose and Thompson have been further modified so as to ascend the lip along a line symmetrical with the noncleft-side philtral column and then ascend superolaterally, bordering the lip-columella junction, to the point of closure in the nostril sill. In minor clefts, the Rose-Thompson principle is sufficient. For most patients with more significant canting of the Cupid’s bow, a small triangle is also positioned above the cutaneous roll. The lengthening achieved by the Rose-Thompson effect significantly reduces the size of the inferior triangle compared with a typical inferior triangle repair. Noordhoff’s vermilion triangular flap is used to correct any vermilion height deficiency of the medial lip element. The repair respects and retains all key landmarks and produces a cutaneous scar positioned along the seams of anatomic subunits. The tension of the repair is positioned above the roll. This accentuates the pout of the lip and allows for the roll elements to approximate end-to-end so the subunit of the roll is not interrupted. At first glance, the anatomic subunit approximation technique may appear to involve the excision of excessive cleft marginal tissue. However, the repair produces a scar in the upper half of the lip that lies intermediate in position to those produced by the rotation-advancement repair and the inferior triangle repair (Fig. 45-1). The scar of the inferior triangle repair is more lateral in the upper part of the lip, indicating that more lateral lip skin is discarded with this repair. Fig. 45-1 The anatomic subunit approximation technique produces a scar in the upper half of the lip that lies intermediate in position to those produced by the rotation-advancement repair and the inferior triangle repair. The rotation-advancement repair, on the other hand, discards more medial lip in the form of the C-flap, which is truly discarded in many incomplete cleft repairs and is displaced from the lip into the sill in complete cleft repairs. Further discard of valuable red lip occurs when lateral lip transverse length is sacrificed to achieve vertical height when the lateral lip element is vertically short. Medial and lateral lip elements thus share more equally in the discard of cleft marginal tissues in the anatomic subunit approximation technique. Furthermore, Noordhoff’s point, and therefore transverse lateral lip element length, is never compromised to achieve vertical height. All patients with unilateral cleft lip are candidates for the anatomic subunit approximation technique. The vertical limb (greater height) of the repair will vary in slope to mirror the noncleft-side philtral column. With minor clefts, the inferior triangle above the cutaneous roll may not be required. Lateral lip markings will vary depending on the vertical height of the lateral lip element. Patients with a contralateral minor-form cleft should be considered for a synchronous bilateral cleft lip repair. This approach provides the best opportunity to achieve symmetry of the Cupid’s bow and of the resultant scar, and provides the ideal opportunity for reconstruction of the prolabial deficiencies of the cutaneous roll, vermilion, and median tubercle.11 For patients with complete clefts, the treatment algorithm in Table 45-1 can be applied. I believe the greatest benefit of presurgical orthodontics used to improve the alignment of the alveolar arches is the increased symmetry of the skeletal nasal base. This is particularly beneficial when significant discrepancy exists in the anteroposterior positions of the alar bases. The anatomic subunit approximation technique can be performed if presurgical orthodontics have not been used. Lip adhesion is not required. Table 45-1 Treatment Algorithm for Patients With Complete Clefts M&T, Myringotomy and ventilation tubes; NAM, nasoalveolar molding; VPI, velopharyngeal insufficiency. Diagrams for this chapter are simplified relative to the original description; the numerical descriptions of the points are described in the text (Fig. 45-2). At the height of the lip, within the nostril sill, two points are chosen: the medial point of closure in the nostril sill (point 16) and the lateral point of closure in the nostril sill (point 19) (Fig. 45-3, A). These points are not distinct anatomic points and as such are the most difficult to describe. The medial point of closure in the nostril sill is positioned lateral to the curve of the lip columellar crease. It will be positioned more medially in complete clefts and more laterally in incomplete clefts. The lateral point of closure in the nostril sill is then chosen on the lateral lip element, relative to the medial point of closure in the nostril sill such that when these two points approximate, two goals are accomplished: (1) nares of equal circumference and (2) symmetry of the alar bases from the anterior view. This is confirmed by manipulation of the medial and lateral lip elements. If the lateral lip is sufficiently tethered and the medial and lateral lip elements cannot be brought together, the lateral lip element should be released first. In the same patient, it would be possible to choose these two points differently and still succeed. These points do not represent true anatomic points; rather they are two points relative to one another such that when they approximate they achieve the previously mentioned goals. Along the vermilion-cutaneous junction, the midline (point 4) and the noncleft-side Cupid’s bow peak (point 5) are marked (Fig. 45-3, B). The noncleft-side Cupid’s bow peak is not marked at the highest point of the curve of the lip. It is marked where the straight portion of the noncleft-side half bow meets the convexity of the lateral lip element. No such convexity occurs on the cleft side of the medial lip element. This curve of the bow on the cleft side will come from the lateral lip element lateral to Noordhoff’s point. The cleft-side peak of the Cupid’s bow (point 6) is positioned on the vermilion-cutaneous junction on the cleft side of the medial lip element equidistant from the midline (point 4). Fig. 45-2 Left unilateral complete cleft lip. A, Preoperative appearance. B and C, Presurgical markings. Fig. 45-3 Left unilateral complete cleft lip medial lip presurgical markings. A, At the height of the lip, within the nostril sill, two points are chosen. The medial point of closure in the nostril sill (point 16 on Fig. 45-2, C) is positioned lateral to the curve of the lip-columellar crease. The lateral point of closure in the nostril sill (point 19 on Fig. 45-2, C) is then chosen on the lateral lip element, relative to the medial point of closure in the nostril sill such that when they approximate, the nares are of equal circumference and the alar bases are symmetrical from the anterior view. B, The noncleft-side Cupid’s bow peak (point 5 on Fig. 45-2, C) is marked where the straight portion of the noncleft-side half bow meets the convexity of the lateral lip element. No such convexity occurs on the cleft side of the medial lip element. This curve of the bow on the cleft side will come from the lateral lip element lateral to Noordhoff’s point. Fig. 45-4 The base width of the inferior triangle (c) is calculated. The total lip height (a; line 2-7 on Fig. 45-2) and greater lip height (b; line 3-8 on Fig. 45-2) are measured from points just above the cutaneous roll above the peaks of the Cupid’s bow to the height of the philtral column in the lip-columellar crease. Approximately 1 mm of lengthening occurs by a Rose-Thompson effect, thereby reducing the required size of the inferior triangle. Along a line perpendicular to the vermilion-cutaneous junction and passing through the cleft-side peak of the Cupid’s bow, point 8 is marked just above the cutaneous roll (at the junction between the cutaneous roll and the “flat” portion of the upper lip). Caudally, from point 8 along this line the incision line will continue across the free border of the lip into the mucosa. From point 8, the incision line will ascend the lip along a line symmetrical with the noncleft-side philtral column to the level of the lip-columellar crease. From the height of the philtral column (point 3), the incision line will traverse superolaterally just outside the lip-columellar crease to the medial point of closure in the nostril sill (point 16). Measurements are taken from the heights of the philtral columns at the lip-columellar crease to the points marked above the peaks of the Cupid’s bow above the cutaneous roll (Fig. 45-4). The total lip height is measured with the lip at rest. The greater lip height is measured with gentle downward traction on the lip to unfurl the medial lip and predict the tension on the lip after repair. The lesser lip height (base width of the small inferior triangle) is equal to the total lip height minus the greater lip height and less 1 mm:
Unilateral Cleft Lip Repair: Anatomic Subunit Approximation Technique
David M. Fisher
KEY POINTS
RECONSTRUCTION PRINCIPLES
PATIENT SELECTION AND EVALUATION
MANAGEMENT ALGORITHM
Presurgical orthodontics (NAM)12
Age 2 weeks to cleft lip repair
Lip repair/primary rhinoplasty
Age 3 to 6 months
Palatoplasty ± M&T
Age 10 to 14 months
Lip revision
Age >3 years as required
VPI correction
Age >4 years as required
Lobule rhinoplasty
Age >7 years as required
Alveolar bone graft
Mixed dentition
Definitive septorhinoplasty
Age >12 as required
Orthognathic surgery
At skeletal maturity, as required
SURGICAL TECHNIQUE
Surgical Planning and Markings
Medial Lip Markings
Measurements and Calculations
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine