Cylindromas are cutaneous tumors first described in the medical literature over 150 years ago. They are now known to occur on an inherited basis as a result of mutations in the tumor-suppressor gene CYLD . The discovery of this gene has provided novel insights into this rare skin tumor syndrome. As well as enabling genetic counseling of affected patients, the knowledge of CYLD function has led to steps toward development of novel therapeutics, with CYLD- regulated signaling pathways as the target for this approach.
Key points
- •
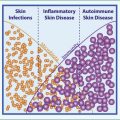
Cylindromas, trichoepitheliomas, and spiradenomas are tumors of the skin appendages occurring in familial cylindromatosis, multiple familial trichoepithelioma, and Brooke-Spiegler syndrome.
- •
The tumor-suppressor gene CYLD was discovered in 2000 and mutations in this gene are responsible for the development of the three tumor syndromes, collectively termed CYLD cutaneous syndrome.
- •
This dominantly inherited syndrome is highly penetrant; however, severity may vary.
- •
Molecular characterization of CYLD function in skin biology has led to new mechanistic insights into tumorigenesis in the care of these patients and paved the way for novel therapeutic strategies.
| BCL3 | B-cell lymphoma 3-encoded protein; a component of the NF-κB pathway, deubiquitinated by CYLD. |
| BSS | Brooke-Spiegler syndrome; a condition caused by a mutation in CYLD with cylindroma and trichoepithelioma occurring together with the related tumor spiradenoma. |
| CK | Cytokeratin; a protein that forms intermediate filaments, providing mechanical support to epithelial cells. Expression of particular cytokeratins is often tissue specific. |
| CYLD | The cylindromatosis gene |
| CYLD | The protein encoded by the cylindromatosis gene |
| FC | Familial cylindromatosis; a condition caused by a mutation in CYLD with the cylindroma as the main tumor type. |
| IKK | IκB kinase; this complex activates NF-κB. |
| MAP3K7 | Mitogen-activated protein kinase kinase kinase 7; forms a complex that activates NF-κB. |
| MFT | Multiple familial trichoepitheliomas; a condition caused by a mutation in CYLD with the trichoepithelioma as the main tumor type. |
| NEMO (IKK-γ) | NF-kappa-B essential modulator (inhibitor of nuclear factor kappa-B kinase subunit gamma); a subunit of the IKK complex that activates NF-κB. |
| NF-κB | Nuclear factor-κB; a family of five transcription factors involved in a range of cellular functions, and negatively regulated by CYLD. |
| RELA/p65 | v-rel avian reticuloendotheliosis viral oncogene homologue A; a transcription factor and member of the NF-κB family. |
| TRAF | Tumor necrosis factor receptor associated factor; proteins in this family interact with tumor necrosis factor receptors and are involved in activation of pathways, such as NF-κB. |
| TRK | Tropomysin receptor kinase or tyrosine receptor kinase; a signaling pathway that may be a potential target for cylindromas. |
Introduction
Tumors of the skin appendages occur sporadically and as part of inherited syndromes. Although these tumors have been described in the medical literature for many years, it is only recently that advances in genetics have allowed clinicians to further understand the origin of these lesions and delineate the clinical syndromes with which they are associated.
Skin appendages are derived from the embryonic ectoderm and include three histologically distinct structures: (1) the pilosebaceous unit (hair follicle and sebaceous glands), (2) the eccrine sweat gland, and (3) the apocrine gland. Tumors of these adnexal structures are classified according to their differentiation as follicular, sebaceous, eccrine or apocrine. Cylindromas are a type of skin appendage tumor thought to arise from hair follicle stem cells. Most present as papules on the skin, mainly on the face and scalp, which can be difficult to differentiate clinically. Diagnosis is often made on histologic assessment of skin biopsy. Although found only rarely on a sporadic basis, cylindromas are the characteristic tumor occurring in multiple numbers in several syndromes.
The autosomal-dominant condition familial cylindromatosis (FC; OMIM 132700 ) is now known to be caused by a germline mutation in the gene CYLD . The first reported case of a patient with FC was described by Ancell in 1842 ( Fig. 1 ) and since then cylindroma, a benign skin appendage tumor, has continued to fascinate, with new mechanistic understandings and insights unfolding up to the present day.
In addition to FC, cylindromas are also found in two additional related tumor syndromes. Multiple familial trichoepitheliomas (MFT; OMIM 601606 ) is a condition defined by the trichoepithelioma, a small skin-colored tumor mainly found on the face, with cylindromas coexisting in lower numbers. Brooke-Spiegler syndrome (BSS; OMIM 605041 ) is considered an overlap between FC and MFT, and here cylindroma and trichoepithelioma occur together with another related tumor, spiradenoma. Key early descriptions of these conditions, which led to the eponymous “BSS,” include a report of a British family with multiple trichoepitheliomas by Brooke in 1892, and an Austrian case of cylindromas by Spiegler in 1899.
Cue forward to the year 2000, and the CYLD gene was discovered by positional cloning and Sanger sequencing. In-depth study of pedigrees with FC using a genetic technique called “linkage analysis” pinpointed the CYLD locus to chromosome 16q, which led subsequently to identification of the gene itself. With this came the confirmation that FC, MFT, and BSS are not in fact separate entities, but overlapping phenotypes resulting from mutations leading to loss of functional CYLD. CYLD functions as a recessive tumor-suppressor gene, and cylindromas show loss of heterozygosity at the CYLD locus as a result of a somatic second-hit on top of a pre-existing germline mutation. Collectively, these conditions may be termed CYLD cutaneous syndrome, because individual labels do not prognosticate.
The discovery of CYLD paved the way for several major steps forward that have occurred in the past 16 years. The mechanisms of tumor formation in the skin can now be investigated and understood on a molecular genetic basis. In addition, the wider role of CYLD has been explored and the cell signaling pathways it regulates have become better understood.
This article provides an overview of the features of the cutaneous tumors that arise in CYLD mutation carriers. Current knowledge of the gene and its function are reviewed, before considering how insights gained from this scientific information may be used toward investigating novel therapeutic strategies in patients.
Introduction
Tumors of the skin appendages occur sporadically and as part of inherited syndromes. Although these tumors have been described in the medical literature for many years, it is only recently that advances in genetics have allowed clinicians to further understand the origin of these lesions and delineate the clinical syndromes with which they are associated.
Skin appendages are derived from the embryonic ectoderm and include three histologically distinct structures: (1) the pilosebaceous unit (hair follicle and sebaceous glands), (2) the eccrine sweat gland, and (3) the apocrine gland. Tumors of these adnexal structures are classified according to their differentiation as follicular, sebaceous, eccrine or apocrine. Cylindromas are a type of skin appendage tumor thought to arise from hair follicle stem cells. Most present as papules on the skin, mainly on the face and scalp, which can be difficult to differentiate clinically. Diagnosis is often made on histologic assessment of skin biopsy. Although found only rarely on a sporadic basis, cylindromas are the characteristic tumor occurring in multiple numbers in several syndromes.
The autosomal-dominant condition familial cylindromatosis (FC; OMIM 132700 ) is now known to be caused by a germline mutation in the gene CYLD . The first reported case of a patient with FC was described by Ancell in 1842 ( Fig. 1 ) and since then cylindroma, a benign skin appendage tumor, has continued to fascinate, with new mechanistic understandings and insights unfolding up to the present day.
In addition to FC, cylindromas are also found in two additional related tumor syndromes. Multiple familial trichoepitheliomas (MFT; OMIM 601606 ) is a condition defined by the trichoepithelioma, a small skin-colored tumor mainly found on the face, with cylindromas coexisting in lower numbers. Brooke-Spiegler syndrome (BSS; OMIM 605041 ) is considered an overlap between FC and MFT, and here cylindroma and trichoepithelioma occur together with another related tumor, spiradenoma. Key early descriptions of these conditions, which led to the eponymous “BSS,” include a report of a British family with multiple trichoepitheliomas by Brooke in 1892, and an Austrian case of cylindromas by Spiegler in 1899.
Cue forward to the year 2000, and the CYLD gene was discovered by positional cloning and Sanger sequencing. In-depth study of pedigrees with FC using a genetic technique called “linkage analysis” pinpointed the CYLD locus to chromosome 16q, which led subsequently to identification of the gene itself. With this came the confirmation that FC, MFT, and BSS are not in fact separate entities, but overlapping phenotypes resulting from mutations leading to loss of functional CYLD. CYLD functions as a recessive tumor-suppressor gene, and cylindromas show loss of heterozygosity at the CYLD locus as a result of a somatic second-hit on top of a pre-existing germline mutation. Collectively, these conditions may be termed CYLD cutaneous syndrome, because individual labels do not prognosticate.
The discovery of CYLD paved the way for several major steps forward that have occurred in the past 16 years. The mechanisms of tumor formation in the skin can now be investigated and understood on a molecular genetic basis. In addition, the wider role of CYLD has been explored and the cell signaling pathways it regulates have become better understood.
This article provides an overview of the features of the cutaneous tumors that arise in CYLD mutation carriers. Current knowledge of the gene and its function are reviewed, before considering how insights gained from this scientific information may be used toward investigating novel therapeutic strategies in patients.
Skin tumors associated with germline cylindromatosis mutations
Clinical Features
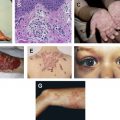
Cylindromas are benign, well-circumscribed, smooth, pale pink nodular tumors, often with arborizing vessels visible ( Fig. 2 ). The tumors are slow growing and vary in size from a few millimeters to more than 5 cm. In severe cases, tumors may cover most of the scalp, which led to the previously used term “turban tumor.” Spiradenomas are benign nodular tumors that are often blue-black in color. They tend to be painful and can grow up to 10 cm in diameter. Trichoepitheliomas are benign tumors, presenting as skin-colored papules. They are mainly found on the face, and are small, usually no more than 2 to 5 mm across. All benign, these skin appendage tumors occur in FC, MFT, and BSS.
Tumors usually start to occur in the second or third decades and accumulate throughout adulthood and most patients with a CYLD mutation present with more than one tumor type. Mutations in CYLD are transmitted in an autosomal-dominant fashion and affect males and females equally. The expression and penetrance of tumor development can vary, however, and there have been reports of a female preponderance to tumors in mutation carriers.
Histologic Features
Cylindromas are thought to arise from precursor cells in the hair follicle epithelium, although previously there has been debate as to the cell of origin, and whether they derive from the follicular, apocrine, or eccrine line (see Fig. 2 ). Cylindromas are nonencapsulated nodular tumors extending into the dermis. They consist of well-defined nests of basaloid cells in a jigsaw pattern, separated by an eosinophilic basement membrane. The term cylindroma is based on the description of the nests of basaloid cells that resemble cylinders when cut in cross-section. Spiradenomas lack the organized structure of cylindromas. They comprise a dense basophilic cellular pattern, vessels may be obvious, and there is often a lymphocytic infiltrate. Some individual lesions show histologic features consistent with both cylindroma and spiradenoma, and have been given the overlap term spiradenocylindromas. Indeed, cylindroma and spiradenoma may represent extremes of a spectrum of the same tumor type, with the transition to spiradenoma being influenced by epigenetic modulation of cell-signaling pathways, such as Wnt. Both tumor patterns express cytokeratins seen in hair follicles, such as CK14 and CK17, and also have regions where cytokeratins seen in eccrine glands are present, such as CK18 and CK77 ( Fig. 3 ). Trichoepitheliomas are nontender skin-colored nodules, with islands of basaloid cells, sometimes displaying peripheral palisading.
Tumor-Associated Morbidity
Although benign, presence of these tumors carries significant morbidity for CYLD mutation carriers. They can frequently be painful, or may bleed or ulcerate, necessitating removal by repeated episodes of surgery. The tumors and the surgical procedures to reduce tumor burden can be disfiguring. Tumors occurring in the ear canal, a favored site for tumor formation, can occlude patency of the canal, resulting in a conductive deafness. Patients can develop painful spiradenomas within pubic skin, resulting in sexual dysfunction. When the tumors cover the head extensively, the scalp skin may need to be grafted and reconstructed. In addition to the physical burden of disease, psychological consequences including depression may occur in those affected.
Malignant Transformation of Benign Tumors
Cylindroma and spiradenoma may undergo malignant transformation into cylindrocarcinoma and spiradenocarcinoma, respectively. This happens infrequently, with fewer than 50 reported cases in the literature. Malignant change is more likely to arise in cylindromas occurring as a result of a CYLD mutation than in solitary sporadic tumors because there are many more lesions in these patients. Clinical features that raise suspicion of malignant transformation include ulceration, rapid growth, pain, bleeding, color change, and the lesion becoming tethered or fixed. This may inform clinical advice given to patients on when to report changing lesions to their dermatologist. Tumors invade locally and may also metastasize to organs including the stomach, thyroid, liver, and lung. Histologically, cylindrocarcinoma may display highly pleomorphic irregular cells with atypical mitoses and disruption of the usual ‘jigsaw’ pattern. Spiradenocarcinomas are composed of solid islands of tumor cells that may show either a squamous or a basaloid pattern. Basal cell carcinomas have been reported to occur in conjunction with trichoepitheliomas, but the direct association between these tumors is unusual. Trichoblastoma, a variant of trichoepithelioma, has been reported to transform into trichoblastic carcinoma, which can metastasize.
Mosaic Presentations
In some patients, the tumors associated with a mutation in the CYLD gene are found in a distinctive linear arrangement, corresponding to the lines of Blaschko. These are areas of skin that each arise from a single epidermal cell. If a somatic mutation in CYLD occurs at the postzygotic stage of embryonic development in an individual with a background of a pre-existing germline mutation, then all the cells arising from the single mutated cell are homozygous for a mutation in CYLD and have the propensity to develop cutaneous tumors.
Associated Tumors
A small proportion of patients, estimated at less than 5%, develop low-grade salivary gland tumors, typically membranous basal cell adenoma.
Related posts:
 Basic Science Insights into Clinical Puzzles
Basic Science Insights into Clinical Puzzles
 Establishing Tolerance to Commensal Skin Bacteria
Establishing Tolerance to Commensal Skin Bacteria
 Dermatologic Manifestations of Monogenic Autoinflammatory Diseases
Dermatologic Manifestations of Monogenic Autoinflammatory Diseases
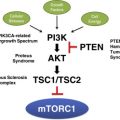 Mosaic Disorders of the PI3K/PTEN/AKT/TSC/mTORC1 Signaling Pathway
Interleukin-22 and Cyclosporine in Aggressive Cutaneous Squamous Cell Carcinoma
Mosaic Disorders of the PI3K/PTEN/AKT/TSC/mTORC1 Signaling Pathway
Interleukin-22 and Cyclosporine in Aggressive Cutaneous Squamous Cell Carcinoma
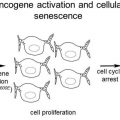 Melanocytic Nevi and the Genetic and Epigenetic Control of Oncogene-Induced Senescence
Melanocytic Nevi and the Genetic and Epigenetic Control of Oncogene-Induced Senescence
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


