Donovan bodies, granulomatous reaction without caseation, pseudoepitheliomatous hyperplasia
Giemsa stain, silver stain
Herpes genitalis
Herpes simplex hominis type II
Intranuclear inclusions
Cytopathology, culture, serology
Lymphogranuloma venereum
Chlamydia trachomatis
Granulomatous reaction without caseation
Serology
Molluscum contagiosum
DNA pox virus group
Intracytoplasmic inclusion
Cytopathology, histopathology
Syphilitic chancre
Treponema pallidum
Ulceration, chronic inflammation vasculitis
Darkfield, fluorescence, silver stain, serology
Tuberculosis
Mycobacterium tuberculosis
Acid-fast bacilli (AFB), granulomatous reaction with caseation
AFB stain, AFB culture
Modified from Wilkinson EJ. Benign diseases of the vulva. In: Kurman RJ, ed. Blaustein’s pathology of the female genital tract. 4th ed. New York: Springer-Verlag, 1994.
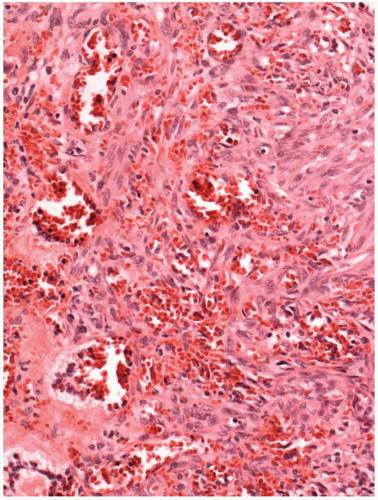
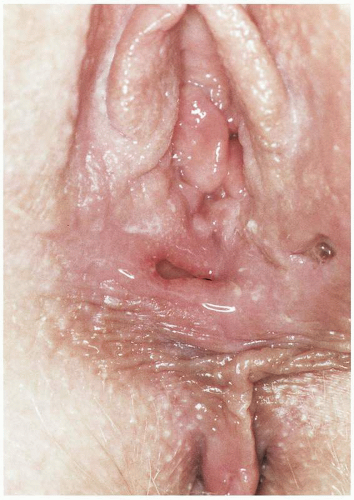
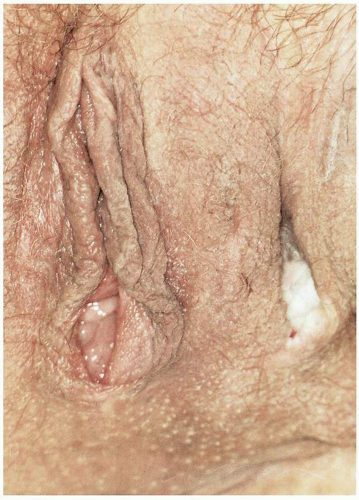
Figure 8.2. Multiple vestibular ulcerations in patient with erosive vaginitis and known AIDS. Complete microbiologic and serologic evaluation was negative and biopsy demonstrated inflammation.
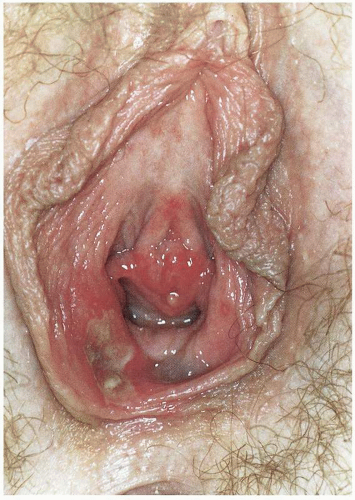
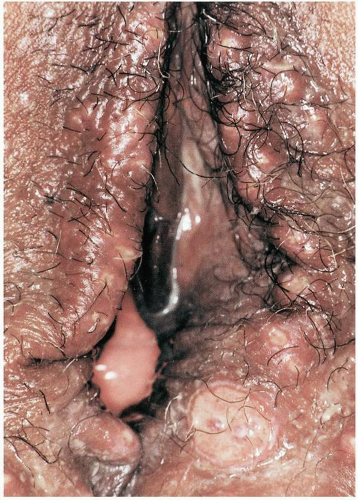
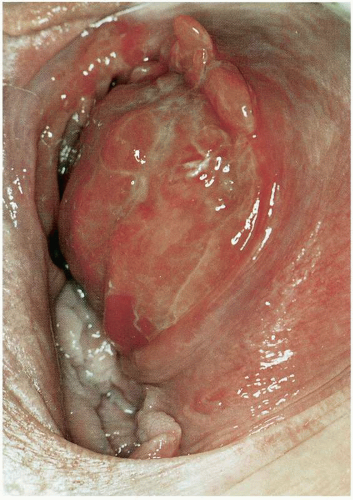
Figure 8.3. Deep “punchedout” ulcer in AIDS patient with negative microbiologic and serologic evaluation (darkfield, VDRL, Gram stain, Chlamydia assay, and HSV culture). Biopsy demonstrated inflammation.
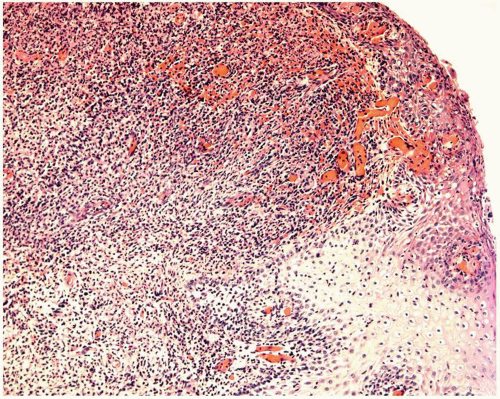
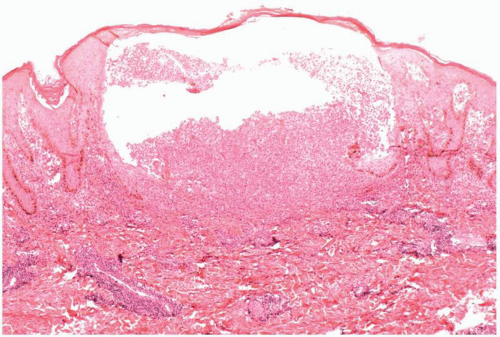
Figure 8.4. Kaposi’s sarcoma. At low magnification the spindle cell neoplasm is evident within the superficial dermis. Some unusual prominent superficial vessels are also present. The overlying epithelium abuts the neoplastic process.
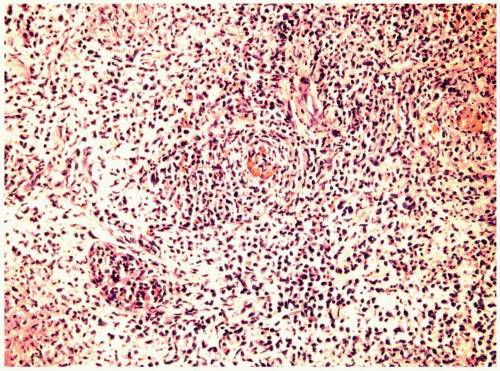
Figure 8.5. Kaposi’s sarcoma. A higher magnification demonstrates the multiple small, blood-filled vessels and spindle cells enmeshed within the dermal collagen.
DEFINITION
The acquired immunodeficiency syndrome (AIDS) is a consequence of infestation of helper lymphocytes with the retrovirus human immunodeficiency virus (HIV), resulting in failure of the host immune defense system and ultimately death as a consequence of the failure of the body’s defense mechanism.
CLINICAL PRESENTATION
Vulvar disease may be a primary presenting complaint in HIV-infected patients whose HIV status is unknown. More commonly, ulcerative disease discovered on the vulva is observed in patients who are known to be seropositive for HIV. The ulcers are frequently multiple and may involve the perianal, vulvar, and vaginal surfaces. They are frequently painful and may or may not demonstrate evidence of superimposed infection. Although usually the patient’s HIV status is known, it must be remembered that these patients may have no other clinical stigmata of AIDS and therefore may present complaining solely of vulvar and perianal ulceration. A high clinical index of suspicion must be maintained.
The diagnosis is made by exclusion. Given the inability to differentiate vulvar ulceration purely on clinical criteria, it is necessary to obtain assays for those agents that commonly cause vulvar ulceration. Ulcers should be cultured for herpes virus. Darkfield or immunofluorescent examination should be accomplished to evaluate for Treponema pallidum. Serologic studies specific for syphilis also should be obtained. Serology for Chlamydia trachomatis as the etiologic agent in lymphogranuloma venereum should be obtained. Cultures for Hemophilus ducreyi, the etiologic organism in chancroid, should be considered. If the HIV status of the patient is not known, then she should be counseled to obtain an HIV assay. If all assays return negative and the HIV assay is positive, the presumptive diagnosis of primary HIV-induced vulvar ulceration may be made. Biopsy of the ulceration should be accomplished to assist in the diagnosis, but nonspecific inflammation will be observed typically. Biopsy will assist though in ruling out entities such as Kaposi sarcoma, Behçet disease, and vulvar carcinoma.
MICROSCOPIC FINDINGS
Kaposi sarcoma may involve the vulva in women with AIDS, but the lesions are usually multiple and found in other cutaneous sites. The lesions of Kaposi sarcoma evolve over time from a patch to a plaque to a nodular lesion.
The microscopic features in the patch phase include a vascular neoplasm composed of thin-walled, irregularly shaped vessels with poorly defined margins that are peripherally separated by dermal collagen. Mononuclear inflammatory cells, consisting predominately of lymphocytes and plasma cells, are found within the interstitial tissues and perivascular spaces. As the lesion develops to a plaque and then nodular mass, the vessels become more numerous and their irregular shape becomes more extreme. Surrounding the angulated and slitlike vascular spaces, atypical spindle cells are evident, that, in the nodular stage, are a prominent feature and form a spindle cell neoplasm with atypical spindle cells. The tumor is poorly demarcated, highly vascular, and has infiltrative margins. Herpesvirus type 8 (HHV-8) is associated with this tumor, and the HHV-8 can be demonstrated by immunohistochemistry. The tumor cells also usually express CD31, CD34, and Desmin.
The main differential diagnosis is bacillary (epithelioid) angiomatosis, which is diagnosed by identifying the bacterium Rochalimaea henselae. This bacterial rod can be identified on silver stain, such as Warthin-Starry stain. When the Kaposi sarcoma is relatively solid, other spindle cell neoplasms, including angiosarcoma and fibrous histiocytoma, may be considered in the differential diagnosis.
The epithelioid neoplastic cells of angiosarcoma contain multilocular cytoplasmic vacuoles. Angiosarcomas are typically more vascular than Kaposi sarcoma. Fibrohistiocytomas are immunoreactive for α1-antitrypsin and α1-antichymotrypsin. They have a storiform arrangement of the spindled neoplastic cells and lack the blood-filled, irregular vascular spaces of Kaposi sarcoma.
CLINICAL BEHAVIOR AND TREATMENT
Initiation of antiretroviral regimen should be accomplished in the newly diagnosed but untreated HIV-positive patient. Ulcerations may also occur in the mouths of patients who are HIV positive and may be a primary manifestation of HIV. These ulcerations often do not heal in response to numerous pharmacologic agents such as acyclovir, ketoconazole, or topical steroids. Moderately high doses of oral steroids have been efficacious in resolving these oral ulcerations. Dosages of prednisone consist of 40 mg per day for 1 week, followed by 20 mg of prednisone per day for the second week. This regimen may be considered in a patient with vulvar ulceration secondary to HIV in whom all appropriate evaluations have ruled out secondary causes for the ulcerations and in whom antiretroviral agents such as zidovudine have not effected a response.
PROGRESSIVE THERAPEUTIC OPTIONS
Progressive therapeutic options are as follows:
After confirmation of HIV seropositivity and negative assessment for secondary etiologies, initiate antiretroviral therapy with compounds such as zidovudine or lamivudine plus zidovudine.
Consider systemic steroid intervention with oral prednisone 40 mg per day for 1 week, followed by 20 mg per day for 1 week.
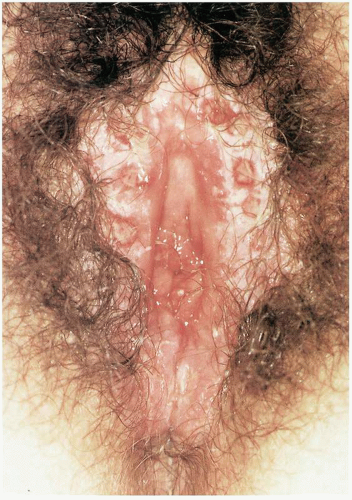
Figure 8.6. Painful ulcer in a patient with oral ulcerations and episodes of abdominal pain. Biopsy demonstrated vasculitis consistent with Behçet disease. Evaluation (serologic and microbiologic) for other potential pathogens was negative. Acyclovir therapy resulted in resolution of ulcer and decreased frequency of oral ulcerations.
DEFINITION
Behçet syndrome is a clinical triad consisting of oral ulcers and genital ulcers associated with ophthalmologic inflammation.
GENERAL FEATURES
Behçet disease is a multisystem inflammatory disease resulting from a primary vasculitis. The etiology is unknown, although genetic and immunologic features have been observed. The disease is most common in Asia, particularly Japan, and in Mediterranean countries, particularly Turkey. A much lower prevalence is noted in patients of northern European extraction. There is also the observation that the HLA-B51 antigen has a higher prevalence in patients with Behçet syndrome.
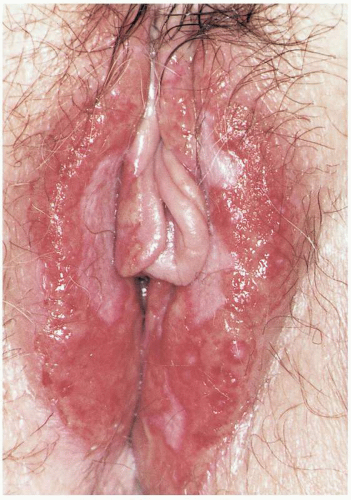
Figure 8.7. Deeply invasive ulcers (2 cm) in a patient with aphthous oral lesions and inflammatory bowel disease. Biopsy demonstrated vasculitis consistent with Behçet disease. Therapy was initiated with prednisone and azathioprine (Imuran).
CLINICAL PRESENTATION
Patients will most commonly present with multiple, painful vulvar ulcers. Numerous systems may be involved with clinical manifestations ranging from mild discomfort due to the ulceration, to life-threatening ischemia secondary to the underlying vasculitis with associated thrombophlebitis. Systems involved may include eyes, joints, central nervous system (CNS), gastrointestinal tract, and skin and mucosal surfaces. Progressive eye disease may eventuate in blindness; however, not all cases have ocular changes. CNS involvement may manifest as headaches, which may progress to seizures related to encephalopathy. Gastrointestinal disease with colitis may progress to perforation of the colon with sepsis and death.
Figure 8.8. Behçet disease. The severe inflammatory infiltrate predominantly consists of lymphocytes with some plasma cells, granulocytes, and eosinophils. Several vessels have microthrombi.
Patients who present to the gynecologist for evaluation will usually present complaining of painful vulvar ulcerations that preclude intercourse. The ulcers may be deep, and fenestration of the labia as well as gangrene of the labia may occur. The ulcers will be quite tender to touch. Examination of the patient’s buccal mucosa will frequently demonstrate multiple similar oral ulcerations.
The international diagnostic criteria for Behçet disease include, in addition to the observation of oral ulcerations, two additional clinical observations that must be made from the following:
Recurrent genital ulcerations
Eye lesions (uveitis, retinal vasculitis)
Dermatologic lesions (erythema nodosum, papular-pustular lesions, or acneiform lesions)
A positive pathergy test (intradermal injection of sterile water resulting in formation of a papule or pustule 48 hours later)
MICROSCOPIC FINDINGS
The key histologic feature is necrotizing arteritis that is typically associated with endothelial cell swelling that may occlude the arterial lumen. Associated venous thrombosis is also commonly observed. A chronic perivascular inflammatory infiltrate is typically present that can extend into the vascular wall of the involved vessels and be associated with homogenization of the media of the involved vessels.
ADJUNCTIVE STUDIES
The vulvar ulcerations should be cultured for herpes virus. Immunofluorescent or darkfield examination should be performed to rule out syphilis. Appropriate serologic studies should be obtained as well, such as Venereal Disease Research Laboratory (VDRL) or rapid plasmin reagin (RPR). The patient should be counseled for and receive screening for HIV status. Likewise, chlamydial serology should be obtained to assess for the possibility of lymphogranuloma venereum.
Figure 8.9. Behçet disease. The overlying epithelium is lost in this deep biopsy from an ulcerated area. There is a marked deep inflammatory infiltrate that is predominantly perivascular with vasculitis.
DIFFERENTIAL DIAGNOSIS
The diagnosis of Behçet disease must be suspected when vulvar ulcerations are observed. Other diseases to be included in this differential are herpes, syphilis, pemphigoid, pemphigus, Crohn disease, lymphogranuloma venereum, and AIDS. Exclusion of Crohn disease may be difficult; patients with Crohn disease typically do not have oral ulcerations. Crohn disease of the vulva is usually located more laterally, involving the skin lateral to the labia majora, resulting in deep-seated “knifelike” lacerations between the labia majora and the medial thighs. Behçet tends to involve the more medial aspects of the vulva. Biopsy may be necessary to differentiate the two conditions because both may involve bowel. Crohn disease is a granulomatous disease of the vulva, whereas Behçet disease is a primary vasculitis. Pemphigus and cicatricial pemphigoid may involve the oral mucosa and eventuate in ulcers. To differentiate these conditions from Behçet disease will require biopsy of vulvar skin and submission for direct immunofluorescent studies. Indirect immunofluorescent studies of serum may also be of assistance in evaluating for these two conditions. The ultimate diagnosis of Behçet syndrome will require the exclusion of these causes of vulvar ulcerations.
CLINICAL BEHAVIOR AND TREATMENT
The ulcerations typically recur and are usually associated with oral ulcers. Management of vulvar Behçet disease is accomplished primarily with application of topical steroids. Moderate-strength steroids such as betamethasone 0.1% applied twice daily for 1 to 2 weeks may result in alleviation of the inflammatory response. In an effort to control pain this may be augmented with topical applications of 2% viscous lidocaine or 5% Xylocaine ointment. Vigorous local hygiene consisting of sitz baths may also be comforting. If this fails to alleviate discomfort, then perilesional injections of triamcinolone (Kenalog-10) may be accomplished, resulting in wheal formation under the lesion. Although the use of birth control pills has been advocated to control vulvar disease, their use should be carefully considered, especially if patients note symptoms in other organ systems. Birth control pills are relatively contraindicated in patients with vascular disease. Anecdotal reports of the efficacy of acyclovir in managing vulvar Behçet disease may prompt a clinical trial; however, there is no known association between herpes virus and Behçet disease. With disabling genital ulceration it may be necessary to initiate systemic steroids in dosages of 20 to 60 mg per day, with subsequent tapering after disease activity is reversed. Failure of systemic steroids to control the disease may require the initiation of immunosuppressant therapy. Azathioprine at 1 to 2 mg/kg per day may result in a significant clinical response and the ability to diminish steroid dosage. Careful monitoring should be accomplished when using immunosuppressant therapy with azathioprine (complete blood count, liver function tests, amylase and lipase levels). This medication should be used by those familiar with its use and potential toxicity. Immunosuppressant therapy should be initiated only to control severe disease. Cyclosporine is an immunosuppressant that may be of benefit in patients who are unable to tolerate azathioprine; however, disease activity must be severe to warrant initiation. Long-term concerns include the association between cyclosporine and renal dysfunction, as well as the development of neoplasm. Lastly, colchicine at l.5 mg per day may be considered, although it seems to be most effective in managing erythema nodosum observed with Behçet disease. The role of colchicine in managing vulvar ulcerations is not defined.
PROGRESSIVE THERAPEUTIC OPTIONS
Progressive therapeutic options are as follows:
Meticulous vulvar hygiene with sitz baths.
Topical betamethasone 0.1% ointment twice daily for 2 weeks and then taper use.
Topical therapy with viscous lidocaine gel 2% or 5% Xylocaine ointment.
Perilesional injection of triamcinolone (Kenalog-10), creating two wheals under the ulcer.
Consider trial of acyclovir 200 mg PO 5 times per day.
Consider a trial of estrogen-containing oral contraceptive if no evidence of multisystem vasculitis is present.
Consider trial of colchicine 1.5 mg PO per day.
For severe disease unresponsive to previous interventions, initiate oral prednisone at 20 to 60 mg per day and begin taper after clinical response is noted.
For significant disease unresponsive to systemic steroid therapy, consider azathioprine (Imuran) starting at 1 to 2 mg/kg per day, with subsequent increase in dosage to 2.5 mg/kg per day if no untoward toxicity noted (careful monitoring of complete blood count, liver function tests, lipase, amylase). With severe disease dose may be started at 2.5 mg/kg per day.
For patients unresponsive to azathioprine, consider cyclosporine at 3 to 5 mg/kg per day with careful monitoring of blood parameters (complete blood count, liver function tests, cholesterol, triglyceride, electrolytes, urea nitrogen, creatine, creatinine clearance). Patients should be counseled extensively about the concern for renal dysfunction and potential development of extragenital neoplasia. Immunosuppressant therapy should be used only by those familiar with its appropriate dosage and side effects.
Figure 8.10. Multiple ulcerated papules and ulcers in various stages of development. These lesions have been present for approximately 2 to 3 weeks in a patient who had intercourse 4 weeks before presentation. The lesions were extremely tender. Herpes culture was negative. VDRL was nonreactive, and Gram stain demonstrated nonspecific findings. HIV screen was negative.
DEFINITION
Chancroid is a sexually transmitted disease caused by the organism Haemophilus ducreyi.
GENERAL FEATURES
Chancroid is a disease primarily of the tropics and subtropics and commonly observed in areas of prostitution. The disease is rarely seen in industrialized nations. Epidemics have been noted in the United States, especially the south and southeastern United States. The disease more commonly affects men than women. There is a frequent association with HIV seropositivity. The organism H. ducreyi is a gram-negative, facultative anaerobic bacillus that tends to exhibit streptobacillary chaining on Gram stain and culture.
CLINICAL PRESENTATION
After an initial incubation period as short as 10 days, papules will arise on the vulva in the region of the labia, fourchette, and vestibule. Rarely, lesions may also be noted in the vagina and on the cervix. These are usually asymptomatic, unlike the vulvar lesions. The papules will become pustular and ulcerate. The subsequent ulcers are tender but not indurated and have a purulent erythematous base that is friable. The surface of the ulcer may appear grayish if superinfection is present. Autoinoculation is common, and hence lesions in various stages of development will be seen in the same patient (papules, pustules, and ulcers). Lesions may be present for weeks or months in patients before symptoms become bothersome and prompt medical care.
The ulcer may be single, but multiple ulcers can occur. The initial ulcer(s) measures 1 to 2 mm in diameter, but multiple ulcers often coalesce, resulting in larger ulcers approaching 3 cm in diameter. The ulcers often have an irregular border that is somewhat undermined and surrounded by a red halo. There will be minimal to no induration, and hence the term soft chancre is often used to describe the ulcer associated with H. ducreyi. Unilateral or bilateral inguinal adenopathy often occurs within 1 to 2 weeks, with flocculent tender nodes. With progression of the disease, a bubo develops. Rupture of the bubo, with formation of chronic draining inguinal sinuses, may eventually result. Similarly, ulcerations on the vulva that remain untreated may form chronic draining sinus tracts.
MICROBIOLOGY
Chancroid is caused by H. ducreyi, a gram-negative, nonmotile bacillus that grows in pairs and parallel chains in culture. Because skin tests may be negative, and biopsies with special stains may not identify the organism, culture is usually necessary for accurate identification of the organism and diagnosis(248). Non-culture diagnostic tests using polymerase chain reaction (PCR) are available and have enhanced our ability to diagnose chancroid.
Culture isolation of H. ducreyi requires selective media (gonococcal agar base and Mueller-Hinton agar base with vancomycin), incubated at 33°C in carbon dioxide in a humid atmosphere. Most laboratories do not have culture capabilities for this organism, and often superinfection of the vulvar ulcerations results in contamination with other organisms, making Gram stain diagnosis impossible. In such cases a presumptive diagnosis based on the clinical presentation must be made, and appropriate cultures obtained for those conditions considered in the differential diagnosis.
MICROSCOPIC FEATURES
The key histopathologic feature is a granulomatoustype reaction with lymphocytes and plasma cells predominating. Gram stain demonstrates gram-negative organisms that may be present in large numbers in parallel chains. If ulceration is present with secondary infection, the inflammatory changes may be mixed.
DIFFERENTIAL DIAGNOSIS
The two primary diseases that may be confused with chancroid are ulcerations resulting from herpes simplex virus (HSV) and ulcerations secondary to T. pallidum (syphilis).
It may be extremely difficult to differentiate herpetic lesions from those secondary to H. ducreyi. Herpetic lesions tend to be more painful and are associated with systemic manifestations when presenting as a primary infection. Herpetic lesions do not typically evolve through a papular-pustular state, but more commonly present as vesicles that subsequently ulcerate. Urinary symptoms are commonly noted with primary herpetic infections. Differentiation between the two conditions requires isolation of herpes simplex by culture or demonstration on Tzanck smear.
Differentiation between chancroid and syphilis is relatively less complicated. Syphilitic chancres are not typically multiple unless autoinoculation has resulted in “kissing” lesions. The chancre of syphilis is typically nontender and is somewhat indurated (the hard ulcer). Syphilitic chancres have fewer tendencies to have a grayish, “dirty” base. One does not see papular-pustular evolution in various stages of development. Diagnosis of syphilis is made by darkfield or immunofluorescent examination and sequential serology.
Primary HIV ulcerations should be considered in the differential diagnosis. These ulcers may be deeply invasive, demonstrating varying degrees of tenderness. The HIV-positive individual with vulvar ulcerations should be evaluated for all infectious causes of such ulcerations before designating the ulcerations as primarily HIV-induced. Such individuals are at risk for chancroid, herpes, and syphilis.
CLINICAL BEHAVIOR AND TREATMENT
Left untreated, chancroid may persist in women for several months, resulting in scarring, fistulae, and draining inguinal abscesses. Rarely, if remission recurs without treatment, relapse may be noted at the site of the original infection. With initiation of treatment there should be prompt resolution of the vulvar ulcerations, if the appropriate diagnosis has been made and if antibiotic resistance is not problematic. Initial therapy should entail oral administration of erythromycin 500 mg four times per day for 7 days. Alternative regimens include ceftriaxone 250 mg IM for one dose or azithromycin l g PO for one dose. For those patients allergic to these regimens, ciprofloxacin 500 mg PO may be administered twice daily for 3 days, provided the patient is not pregnant. Ciprofloxacin is contraindicated in pregnancy.
For patients with suppurating inguinal adenopathy, assistance may be obtained via drainage of the bubo under local anesthesia. The abscess should be entered through normal skin, lateral and superior to the abscess. If there is reaccumulation of pus within the bubo, a repeat needle aspiration may be necessary. The bubo does not require surgical drainage; aspiration is sufficient.
Appropriate HIV screening is indicated in all individuals with a diagnosis of chancroid, and appropriate counseling should be administered.
PROGRESSIVE THERAPEUTIC OPTIONS
Progressive therapeutic options are as follows:
Erythromycin 500 mg PO four times daily for 7 days (or) ceftriaxone 250 mg IM once (or) azithromycin l g PO once (or) ciprofloxacin 500 mg PO two times daily for 3 days. (Ceftriaxone and azithromycin are less effective as single-dose therapy in HIV-infected individuals.*)
Needle aspiration superiorly and laterally through noninfected skin to drain an inguinal bubo.
Figure 8.11. Decubitus ulcer overlying the left ischial tuberosity in a paraplegic patient. An identical lesion was present over the right ischial tuberosity.
DEFINITION
A decubitus ulcer is most commonly seen in paralyzed patients who do not use adequate padding to prevent necrosis of skin and underlying tissue resulting from pressure against the bony pelvis.
CLINICAL PRESENTATION
The paralyzed patient with a decubitus ulcer will not present until secondary infection has induced a localized process resulting in a significant discharge or until an ulcer is palpated on self-examination. The ulcer will overlie a bone prominence and will on occasion be sufficiently deep to expose the bone. In such instances the risk of osteitis exists. The most common locations of the ulcers are under the pubic rami, occurring when a patient sits on the arm of a wheelchair for prolonged periods, or just above the ischial tuberosities, occurring when maximum pressure is exerted on the buttocks when seated.
Figure 8.12. Decubitus ulcer inferior to the pubic ramus in a paraplegic woman who commonly straddles the arm rest of her wheel chair.
MICROSCOPIC FINDINGS
Decubitus ulcers are generally not biopsied and are usually recognized by their distinctive locations in the setting of the bed-ridden or wheelchair-confined patient. The histopathologic features are nonspecific, and the depth of ulceration is highly variable. In all cases, the epithelium is lost and the underlying dermis has a chronic inflammatory infiltrate without evidence of vasculitis. Organisms may be identified on silver or Brown and Brenn stains, but are confined to the surface of the ulcer.
DIFFERENTIAL DIAGNOSIS
All etiologies of vulvar ulcerations may be considered in the differential diagnosis, but the typical location of the ulcerations over the ischial tuberosities or just under the pubic rami within the vestibule of the vulva usually will not warrant further studies. Biopsy will exclude invasive squamous cell carcinoma, appropriate cultures assist in evaluating for herpes virus, and darkfield examination and serology will rule out syphilis.
CLINICAL BEHAVIOR AND TREATMENT
Once these deep-seated chronic ulcers have formed, it is difficult to effect normal skin healing and architecture. The underlying problem of paralysis with lack of sensation still exits and cannot be corrected; therefore pressure necrosis is always a distinct possibility. Appropriate padding on the wheelchir and education concerning avoidance of hard surfaces while seated will be the mainstay of therapy. Evidence of infection may warrant antibiotics.
Figure 8.13. Multiple ulcers of uncertain duration, culture positive for HSV type 2. Acyclovir therapy was instituted for primary herpes. Patient has monthly recurrences for 5 to 7 days.
PROGRESSIVE THERAPEUTIC OPTION
The progressive therapeutic option is as follows:
Education concerning appropriate bed care and padding to protect the ischial tuberosities and the pubic rami when seated
Figure 8.14. Multiple tender ulcers of approximately 3 days duration associated with fever and dysuria. The culture was positive for HSV type 1. Acyclovir therapy was instituted for primary herpes. No recurrence has been noted for 8 months.
Figure 8.15. A lesion on the buttock of an HIV-positive patient. The ulcer has been present for 7 months and is, on evaluation, culture-positive for HSV. Prompt resolution of the ulcer occurred with initiation of acyclovir therapy.
DEFINITION
Herpes virus infection is an acute, recurrent, or chronic inflammatory process caused by the herpes simplex virus, usually type II (HSV II).
GENERAL FEATURES
Herpes simplex is a double-stranded DNA virus belonging to the same family as varicella-zoster, cytomegalovirus, and Epstein-Barr. Two serotypes of herpes simplex exist—HSV-I and HSV-II. Although HSV II is more commonly associated with genital infection, HSV type I may also be a pathogen for the vulva. HSV is considered a sexually transmitted disease; however, infection can be acquired by other direct contact. The herpes virus is the most common cause of vulvar infectious ulcers in the United States. It most commonly affects adolescent and young sexually active individuals.
Figure 8.16. Herpes present for 2.5 months in a patient with pancytopenia and an unknown HIV status.
CLINICAL PRESENTATION
There are three clinical HSV disease states: initial primary infection, initial nonprimary infection, and recurrent infection. Initial primary infections occur in patients who have never been exposed to HSV and do not possess protective antibodies. The clinical manifestations of the virus will typically occur after 3 to 7 days of incubation. Initial symptoms of pruritus and burning will be followed in 24 to 72 hours by the occurrence of a vesicular eruption on the vulva. The vesicles may continue to present over a number of days. Rupture of these vesicles will result in diffuse ulcerations that may coalesce. These ulcerations are exquisitely painful. Systemic symptoms including fever, headache, and malaise often occur and can be severe. Usually there will be viral infection of the urethra and bladder, and dysuria will be a common symptom in primary infections. This may progress to acute urinary retention. Primary lesions will usually persist for 2 to 6 weeks, followed by healing without scar formation. Immunocompromised patients, including patients with AIDS, may develop a disseminated infection, which will frequently terminate in death.
Figure 8.17. Herpesvirus infection. This biopsy is from a regressing vesicle. Necrosis with acute inflammation is evident in the epithelium. The viral changes are found at the edge of the intraepithelial abscess.
Multiple extragenital herpes lesions and significant systemic symptoms should alert the clinician to this possibility. Chronic herpes infection may also occur in these individuals, usually presenting as a chronic non-healing ulcer or ulcers. Culture of such ulcers for herpes virus is usually diagnostic.
Patients with nonprimary, first-episode herpes and patients with recurrent disease will have significantly less discomfort and less evidence of systemic disease than patients with initial primary disease. Patients with nonprimary, first-episode infections will have been infected subclinically at some point in the past and have circulating antibodies to HSV. These circulating antibodies will ameliorate the disease process. The vulvar manifestations may be so minor as to be unobserved in both nonprimary initial infections and recurrent infections. Painful ulcers will usually be present, but will not generally be as widespread as with primary episodes. The ulcers will not persist beyond 1 to 2 weeks.
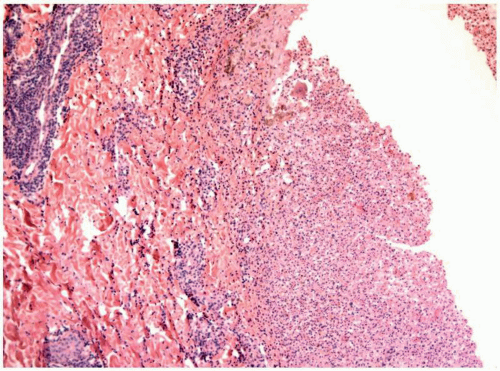
Figure 8.18. Herpesvirus infection. Acute and chronic inflammatory cells are present in the superficial dermis and about vessels beneath the vesicle.
Occasionally, secondary to autoinoculation, the disease may be discovered in additional body sites other than the vulva. Of particular note is involvement of the fingers, buttocks, and oral-labial mucosa. The latter may be secondary to oral-genital sex with the infecting partner. The diagnosis is suspected in all patients with vulvar ulcerations. Initial primary infections with significant systemic symptoms are classic in appearance. Nonprimary initial infections and recurrent infections may be so minor as to elude the clinician’s observant eye. This will not usually be the case. Confirmation of diagnosis is imperative for initiation of therapy and for appropriate preventative counseling.
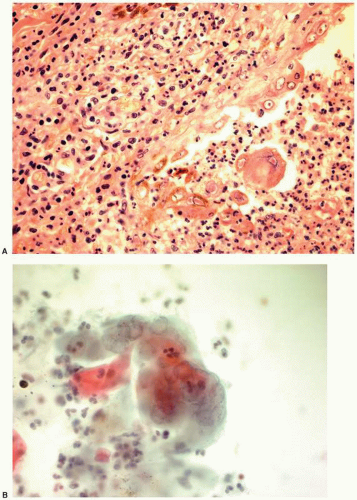
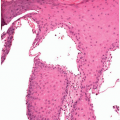
Figure 8.19. A: Herpes simplex virus infection. A higher magnification of the herpes ulcer demonstrates the viral epithelial changes. The nuclear chromatin of some of the involved keratinocytes is clear, and others have typical intranuclear inclusions. B: HSV infection; cytologic smear of an unroofed vesicle. Multinucleated cells are present with nuclear chromatin change, including “ground glass” appearance of the nuclear chromatin in some cells and intranuclear inclusions in a few cells. These cytologic findings are characteristic of HSV infection.
MICROSCOPIC FEATURES
Acute herpes infection within the epithelium is characterized by epithelial nuclear changes that first are seen as homogenization of the nuclear chromatin of the epithelial keratinocyte giving a “ground glass” appearance. The keratinocytes become multinucleated and, as the virus replicates within the nucleus, eosinophilic intranuclear inclusions will be evident. With cell death there is karyorrhexis and cell lysis with release of the assembled viral particles into the vesicle and on to the epithelial surface when ulceration occurs. The intraepithelial vesicle contains predominately acellular fluid and is lined by epithelial cells that show viral cytopathologic changes. These changes are most evident along the epithelial edge of the vesicle. The ulcerated vesicle has an eroded and ulcerated epithelium with an acute and chronic inflammatory infiltrate that involves the dermis or submucosa beneath the ulcer. At this stage the typical viral cytopathologic findings may not be evident, although immunohistochemical techniques for herpes virus antigen may demonstrate the presence of virus within the intact epithelial cells as well as within endothelial cells. The histopathologic features cannot distinguish a primary from a secondary herpes virus infection, nor can herpes type I or II infections be distinguished.
ADJUNCTIVE STUDIES
Tzanck smears, a cytologic scraping of the ulcer or contents of the vesicle, or cervical or cervical-vaginal cytologic preparations (Pap smears), may be used for the initial clinical evaluation. The gold standard of diagnosis is the herpes culture. In addition to culture, monoclonal antibodies to herpes virus can be employed in immunofluorescent or immunohistochemical techniques to identify the virus within the nucleus of the involved cells. In addition, PCR or other molecular techniques can also be used to identify herpes virus. Viral culture for herpes virus should be obtained on all patients with vulvar ulcerations. The greatest recovery rate will be noted in those lesions that are in the vesicular stages, with culture taken from scraping the vesicle wall and including the contents of a vesicle. Early ulcerative lesions will also return high positive recovery rates, but ulcers of longer duration are falsely negative in approximately half the cases (82% recovery rate for ulcerative primary lesions and 43% recovery rate for ulcerative recurrent lesions). It is therefore imperative to culture the lesion early in the course of the disease. Serologic studies for herpes virus antibody titers may be obtained, and these may be helpful in differentiating those patients who have initial primary lesions from those who have initial nonprimary lesions. This is not usually clinically germane and is therefore usually not cost-effective. The presumptive diagnosis of HSV infection is usually made on clinical evaluation, and definitive diagnosis awaits culture result. For the patient who presents after several days or weeks of discomfort, culture results may be falsely negative.
DIFFERENTIAL DIAGNOSIS
It is important to consider the differential diagnosis of vulvar ulcerations and obtain appropriate evaluation in addition to herpes cultures. One must consider the possibility of a primary syphilitic infection. Although chancres are classically nontender, superimposed infection may result in tenderness. Darkfield or immunofluorescent examination and serologic studies should be obtained. Human immunodeficiency virus may be a cause of primary vulvar ulceration and should be considered in the differential diagnosis. Likewise the immunocompromised patient with a herpetic infection may be at increased risk for disseminated herpes virus infection or secondary infection, and this information should be available to the treating physician. Behçet disease may present with vulvar ulcerations, oral ulcerations, and visual disturbances. There are no serologic assays for Behçet disease; clinical diagnosis is based on the international classification system for Behçet disease. Pemphigus and pemphigoid may present with vulvar ulcerations, and diagnosis will be based on histologic and immunohistologic studies.
CLINICAL BEHAVIOR AND TREATMENT
Acute herpes virus infection involving the genital tract will typically heal, without scar formation, within 6 weeks. Recurrent (nonprimary) episodes of infection are common and may occur for years following the primary infection. The severity and duration of the recurrent episodes typically decrease over time until the patient becomes asymptomatic.
Initial treatment of the patient with herpes vulvar disease is based on control of the symptoms. Analgesics and antipruritics may be necessary to control systemic manifestations of primary infections. Urinary retention will often require placement of a suprapubic catheter. Intraurethral catheters will be uncomfortable due to the urethral irritation caused by the primary infection. If a transurethral catheter is used for bladder drainage, appropriate topical anesthetic gel should be placed on the catheter and urethra before insertion. Cool soaks will augment the analgesic effect of orally administered analgesics. Salt water sitz baths may be beneficial. Therapy with acyclovir is indicated in primary infections. The dose is 200 mg five times daily for approximately 7 to 10 days. Alternatively, the drug may be administered as 400 mg three times daily as a more convenient dosing form. Patients with significant systemic symptoms or findings who are incapable of taking oral acyclovir or who are suspected of having disseminated disease should be admitted to receive intravenous acyclovir at 5 mg/kg every 8 hours for 5 to 7 days. For immunocompromised patients, higher dosages or oral therapy are recommended for moderate disease (400 mg 5 times daily) and hospitalization should be strongly considered with suspicion of disease dissemination.
Treatment for recurrent genital herpes is 200 mg PO five times daily for 5 days, provided the infection is noted early in the disease state. If therapy is initiated early for recurrent genital herpes, viral shedding may be reduced and the duration of the episode may be reduced as well.
For the patient with significant recurrent disease, prophylactic use of acyclovir may be considered. This may be administered as 400 mg twice daily. The decision to initiate acyclovir prophylaxis should be based on a reasonable assessment of the patient’s number of recurrences. It would be less than cost-effective to initiate therapy for one episode of recurrence per year. It is also imperative that patients use safe and efficient contraception while taking prophylactic acyclovir. This may be continued for 12 months, at which time reassessment must be considered. Long-term side effects of acyclovir remain to be defined. The potential for side effects versus benefits should be weighed. The possibility of acyclovir resistance must also be considered. With chronic use of acyclovir, especially in immunocompromised patients, emergent of resistant strains of herpes virus may have significant implications for the patient.
Patients should be advised that asymptomatic viral shedding may occur at any time in the absence of clinically obvious herpes lesions. Patients should abstain from any form of direct contact when obvious lesions are present and should use barrier contraception with contraceptive foams or gels with antiherpetic activity. Patients will often require extensive counseling concerning the future ramifications of what will be a lifelong infection with the herpes virus. It should be clear to the patient that the herpes virus will reside in a dormant state in the dorsal root ganglion of S2, S3, and S4 and may at any time recur due to unknown factors. Emphasis should be placed on the potential risk for a future pregnancy delivered through a birth canal with an obvious herpetic lesion. Neonatal infection with herpes has a high mortality rate.
PROGRESSIVE THERAPEUTIC OPTIONS
Progressive therapeutic options are as follows:
Initial primary infection: acyclovir 200 mg PO five times daily for 7 to 10 days.*
Oral analgesics and antipruritics for systemic symptoms.
Suprapubic or urethral catheterization for urinary retention (preferably suprapubic).
For recurrent herpes: acyclovir 200 mg PO five times daily for 5 days.**
Prophylaxis for recurrent herpes of significant impact: acyclovir 400 mg twice daily for 1 year and reassess and counsel patient appropriately. Appropriate effective contraception should be mandatory when taking prophylactic acyclovir.
For the immunocompromised patient (AIDS): In patient with moderate primary disease consider increasing the acyclovir dose to 400 mg five times daily and determine length of therapy by response.
Only gold members can continue reading. Log In or Register to continue