Key points
- •
To understand the underlying structural anatomy of the face, including the superficial musculo-aponeurotic system (SMAS), originally described by Mitz and Peyronie in 1976, platysma and supporting ligaments.
- •
To identify the structural support issues that may be apparent after skin-only facelifts.
- •
To assess different SMAS elevation and suspension techniques including right angle SMAS plication, lateral SMASectomy, extended SMAS technique, lamellar high SMAS technique and their indication for different groups of patients.
- •
To critically assess the importance of differential vectors of pull for both SMAS and skin flaps.
- •
To understand why structural suspension of the SMAS is important in achieving natural and lasting results in facial rejuvenation.
Introduction
Surgical rejuvenation of the aging face has evolved into one of the most common aesthetic surgical procedures performed throughout the world. As surgeons have better identified and understood the underlying structural anatomy of the face, a variety of techniques have developed over the last several decades which have shared a common goal of treating the anatomic changes associated with facial aging.
Initially, patient and surgeons focused on correction of the skin laxity that occurs with facial aging, attempting to tighten loose skin rather than reconstructing the underlying foundation of the facial structure. Consequently, these techniques often created the stigma of being ‘pulled too tight’ or what has been described as ‘wind-tunnel appearance’. The appearance of tightened jowls from the nasolabial fold to the preauricular region with residual laxity of the zygoma and midface tissues created a sub-optimal result indicative of a skin-only facelift which Hamra described as a lateral sweep.
A significant challenge associated with these types of facelifts lies in the fact that the skin serves only as a redraped, covering function. With its inherent anatomical elasticity, skin does not possess the structural integrity to support underlying sagging muscle, fat or deeper support structures. The SMAS, anatomically, is a structural support layer that is inherently inelastic. Utilizing the SMAS and platysma, either by plication, resection, or extended or lamellar dissection, to elevate sagging facial tissues and create facial contour serves as a method whereby tension can be transferred to a non-elastic structure away from the skin. Subsequently, problems associated with excessive skin tension, such as poor scarring, tragal retraction, earlobe malposition and an excessively tight look can be avoided.
Anatomy
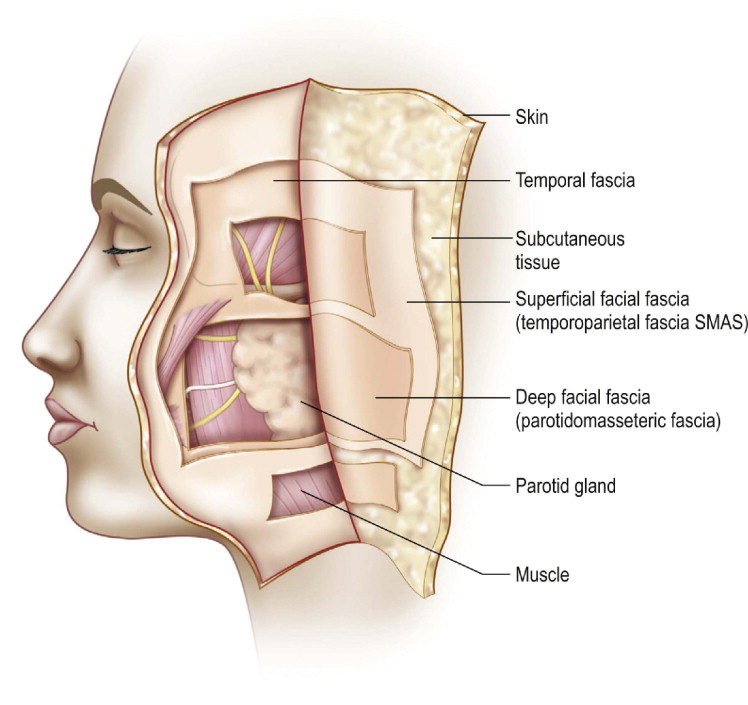
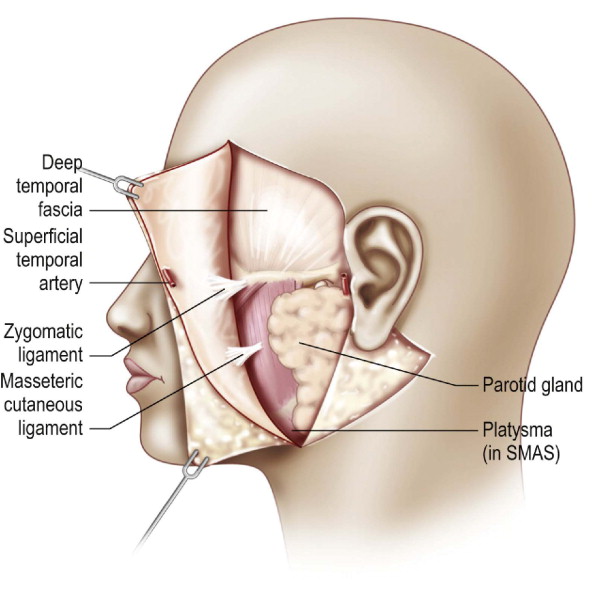
The SMAS is a well defined portion of the superficial facial fascia. The superficial facial fascia is a discrete fascial layer that forms a continuous sheet throughout the face and neck extending into the malar region, the lip and the nose ( Figure 11.1 ). In the forehead, temporal area and scalp, it is defined as the temporoparietal fascia (aka the superficial temporal fascia), which separates the subcutaneous tissue from the underlying muscles and the deep facial fascia and nerves. The SMAS represents an upward extension of the superficial cervical fascia into the face. The temporoparietal fascia, in corollary, is an extension of the SMAS into the temporal and scalp regions. The SMAS is thickest over the parotid gland, the temporal region (as the temporoparietal fascia) and the scalp (as the galea). The SMAS is thinnest over the masseter muscle and the malar region; great care must be taken during dissection in this region so that the flap can be thick enough for facial contouring. The SMAS often varies in thickness among patients depending on their build and amount of deflational facial aging.
In its relation to facial aging, the SMAS can often be divided into fixed and mobile portions. The fixed portion lies over and is firmly adherent to the parotid gland. Subsequently, it is immobile in this position. The mobile portion lies medial to the parotid, directly over the mimetic muscles, facial nerves and parotid duct. Because it is not adherent to these structures, it is highly mobile. Elevation and mobilization of this portion of the SMAS result in movement of the midface and lower face.
During dissection of the SMAS in this area, the muscles most likely to be visualized during a facelift (orbicularis oculi, platysma, zygomaticus major) are superficial and innervated by facial nerves on their deep surface. The deepest muscles (buccinators, mentalis, levator anguli oris) are innervated on their superior surface. During dissection, as long as SMAS elevation is performed above these muscles, denervation is unlikely.
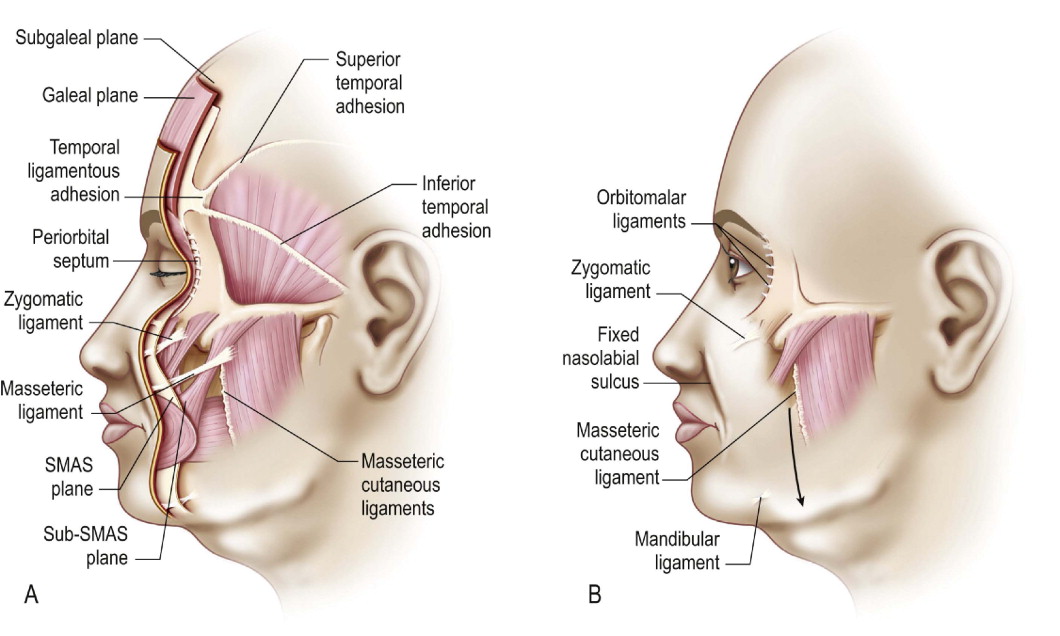
Retaining ligaments, which serve to support the facial skin in its normal anatomic position, run from the underlying fixed bony portions into the overlying dermis and between soft tissue structures of the face ( Figure 11.2 ). Stuzin et al described two types of retaining ligaments: true osteocutaneous ligaments which run from the periosteum to the dermis (such as the zygomatic and mandibular ligaments) and ligaments which are formed from the coalescence of the deep and superficial fascia that fixes the facial layers to the dermis with underlying structures (such as those connecting the parotid and the masseter to the underlying dermis through fibrous septa). In order to adequately elevate the SMAS for mobilization, the zygomaticocutaneous ligament (i.e., the first type) and the parotidomasseteric ligaments (i.e., the second type) must be divided ( Figure 11.3 ).
Indications for SMAS treatment
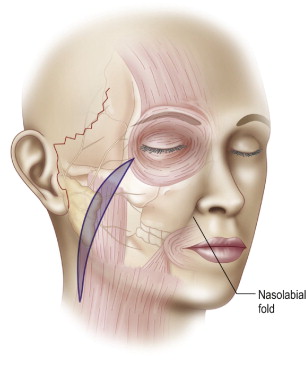
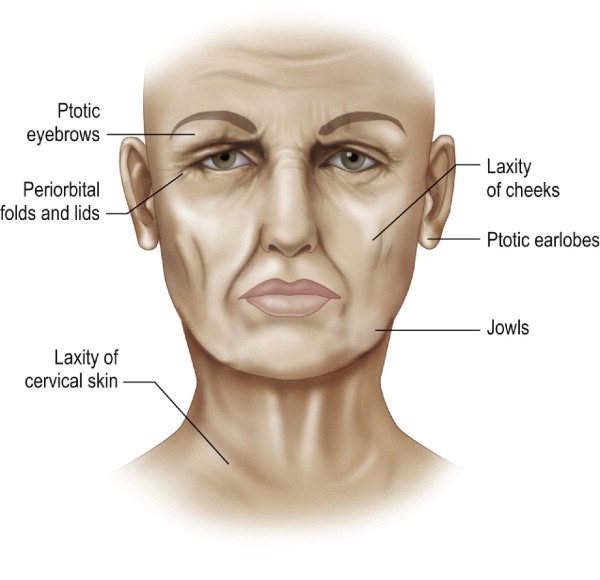
Patients who are candidates for preferential treatment of the SMAS during traditional or minimally invasive facelift techniques should be in good health to minimize surgical risk. Treatment of the SMAS will add significantly more time to the rhytidectomy (approximately 1–2 additional hours depending on which technique is utilized) and patients should be candidates to tolerate the additional anesthetic and surgical risk. In general, patients who possess the hallmarks of deep facial aging, such as deepened nasolabial folds, facial jowling and an obtuse cervicomental angle are candidates for SMAS elevation and suspension techniques ( Figure 11.4 ).
There are several options for treatment of the SMAS during rhytidectomy. For the surgeon, it is often more advantageous to decide the treatment of the SMAS (i.e., advancement vs plication) once the subcutaneous dissection has been completed. This allows the integrity of the SMAS, as well as its ability to sustain suturing techniques, to be assessed directly. If the patient is very thin, often the SMAS is fairly diminutive. After subcutaneous dissection, the lower SMAS can be grasped with a forceps and repositioned substantially to achieve the desired mobilization. In these two instances, plication of the SMAS, either through a fusiform outline parallel to the nasolabial fold or triangularly between the axis of the zygoma and the preauricular line, may be advantageous.
Baker developed the lateral SMASectomy in evolution to avoid substantial undermining of the SMAS that may place the branches of the facial nerve at risk. Generally, the technique is performed by excising a fusiform strip of SMAS along a line from the lateral orbicularis to the mandibular angle, which is parallel to the nasolabial fold. In addition, a suspension of the plastyma is performed to the mastoid fascia in an effort to treat the mandibular contour. Advantages of this technique include its ease, minimal risk, ability to be combined with short-scar techniques and its efficiency.
Lower SMAS techniques, where the SMAS incision is placed far below the zygoma, while treating the lower cheek and jowl, have the disadvantage of not adequately treating the midface or perioral region. Subsequently, these techniques have been criticized by predisposing to a lateral sweep deformity. Higher SMAS dissection techniques have the advantage of redistributing the structural components of the face while creating an effective pull in the midface triangle. Stuzin, who is credited with evolving the extended SMAS technique, places the SMAS incision below the zygoma while extending the medial incision superiorly with a triangular pennant to effectively pull the malar fat pad and midface with the composite flap. A strip of SMAS is divided laterally and resuspended posteriorly to the mastoid fascia. Marten and Connell have popularized the utility of a high SMAS technique where the SMAS incision is placed at the level of the zygoma and redirected with a superior, slightly lateral vector. These techniques have the benefit of restoring the youthful upper cheek contour and improved correction of the nasolabial fold.
Operative technique
Standard facelift incisions are marked pre-operatively. When a standard facelift incision is utilized, it is the surgeon’s preference to design the incision anteriorly along the hairline or superiorly into the temporal hair. Posteriorly, the incision can be directed along the hairline or into the occipital hair. When a short-scar facelift is utilized, access to the mandibular margin, the lower SMAS or the platysma may be limited. In instances where a short-scar design is chosen, patients usually do not require a formal neck lift or platysma tightening. Subsequently, the SMAS pull is usually directed vertically.
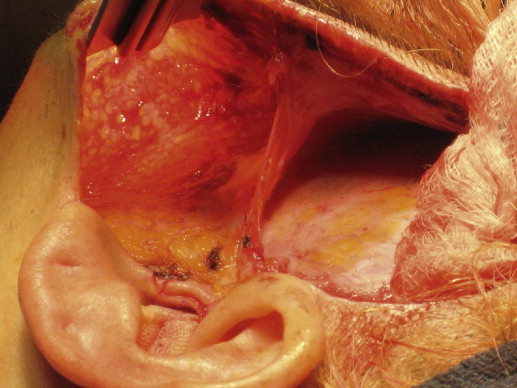
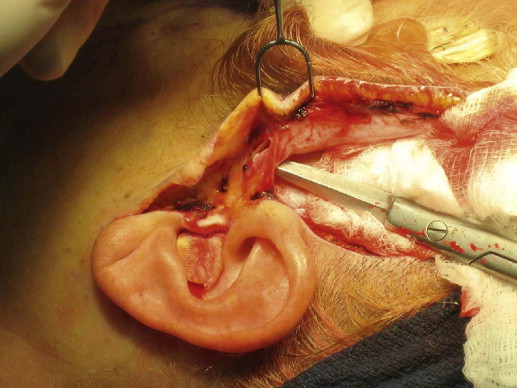
SMAS suspension or plication can also be utilized with a subcutaneous dissection or in the temporal area where dissection is performed on the deep temporal fascia. In the later instance, a mesotemporalis flap is maintained in order to protect the temporal branches of the facial nerve, which is located at the level of the superficial temporal fascia ( Figure 11.5 ). At the lateral portion of the mesotemporalis flap, the superficial temporal artery may be divided to assist with lateral advancement ( Figure 11.6 ).
Depending on the condition of the neck, treatment of the anterior platysma should also be decided upon prior to the SMAS treatment. Because the SMAS and platysma represent the same anatomical layer, treatment of each area will affect the result of the other. If platysmaplasty is performed first, the descended jowl fat is often prevented from being repositioned from the neck. Movement of the superficial fascia will be diminished after SMAS treatment, creating a loss of aesthetic contour and the inability to modify its shape. If SMAS treatment is performed prior to the platysmaplasty, descended jowl fat can be repositioned above the mandibular border, allowing aesthetic contouring of the jawline. The authors prefer SMAS treatment prior to platysmaplasty because it creates a diminished need to resect cervical fat and allows the anterior cheek to be augmented by SMAS mobility.
SMAS plication
During subcutaneous dissection, a thin, uniform, cobblestoned layer of fat should be maintained on the skin flap to preserve blood supply. Dissection in this plane allows the anterior parotid SMAS to be identified more readily. The decision to perform plication versus dissection of a SMAS flap is often decided upon intraoperatively. In general, if the SMAS is grasped with a forceps and it is easily mobile and can be repositioned 1–2 cm, plication can be successfully performed. A secondary indication is the need for additional facial fullness in the malar area especially in thin faced patients. The plication can be designed such that it acts as an autologous tissue auto-augmentation. This is particularly the case with the use of purse-string sutures in the SMAS as described by Tonnard and Verpaele (see Chapter 9 ).
There are several options for plication. In part, the design of the plication should be determined by the aesthetic result that is desired in each particular patient. For example, if a patient has deepened nasolabial folds and jowling, a fusiform plication can be designed ( Figure 11.7 ). In this technique, a surgical marker is used to design a line which extends from the malar eminence obliquely to the angle of the mandible. A fusiform or lenticular ellipse is then designed to encompass this line for the desired plication. In general, the widest portion of the ellipse is closed first in order to gauge the extent of SMAS redistribution.