Abstract
Botulinum toxin can be effective in balancing the muscles of the perioral area as they age. The author avoids paralysing the muscles of the upper lip by eliminating upper lip rhytids with CO 2 laser resurfacing and fine fillers instead. Elongation of the upper lip by reduction of resting tone with botulinum toxin usually has an ageing effect on the face. Botulinum toxin is very successful for management of ‘pebbly chin’ and softening the droop of the outer corners of the mouth. The author chooses hyaluronic acid fillers to the lateral commissures of the mouth and combines this with botulinum toxin to the depressor anguli oris if indicated. Botulinum toxin is excellent for maintaining apposition of scar margins vulnerable to tractional separation, for example a frontalis scar. It is essential for treatment of unilateral neck muscle overaction in facial paralysis, but also effective for turkey neck and horizontal banding, as well as reducing downward ‘pull’ on jowls (the Nefertiti lift).
Key words
Botox, Dysport, upper lip rhytids, neck bands, scars, Nefertiti lift, perioral lines
BOTOX 2.5 mL to 100 units, 4 units in 0.1 mL
Xeomin 2.5 mL to 100 units, 4 units in 0.1 mL
Dysport 3.5 mL to 500 Speywood units, 14.3 units in 0.1 mL
Azzalure 0.63 mL to 125 Speywood units, 10 units in 0.05 mL
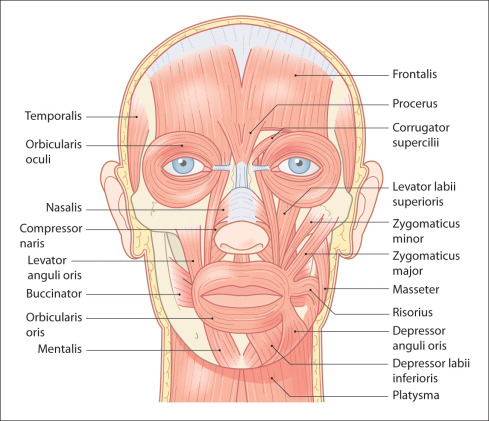
A good knowledge of the anatomy of the perioral region is essential before undertaking botulinum toxin treatment. The orbicularis oris responds well to botulinum toxin, but great care must be taken to limit diffusion into the surrounding muscles ( Fig. 10.1 ). This can be achieved by using a higher concentration of the toxin, at a smaller dose. Treatment of the wrong muscle fibres can lead to dribbling, difficulty in drinking water, slurred speech and asymmetrical smiling.
Patients with facial hemispasm frequently require botulinum toxin to a focus of spasm over the elevator of the lip. This leads to a depression of the corner of the mouth and drooling of saliva ( Fig. 10.2 ). But patients would usually rather have an embarrassing dribble than an uncomfortable spasm and twitching of the side of their face. However, this complication MUST be avoided in a cosmetic practice.

Ageing of the perioral region and neck
Ablating wrinkles does not always make a patient look younger. When considering rejuvenation of this area, examine the overall tone of the musculocutaneous complex. Also examine the skeletal support, the dentition and the shape of the nose.
Research has confirmed that ageing causes an anteropostero recession of the facial bones, which contributes to sagging. The distance from the nose to the vermilion border increases with time. The vermilion border itself shrinks, and the lips lose volume and tend to turn downwards instead of up and out.
The lip depressors and elevators induce wrinkles at the corners of the mouth and ‘marionette lines’. The mentalis muscle encourages the tip of the chin to turn upwards, creating the mental fold and sometimes a ‘pointed’ chin. Recession of the jaw will accentuate the wrinkles, from the corner of the mouth to the chin.
The platysma muscle will eventually draw the sides of the mouth towards the jaw, and this, along with facial sagging, creates jowls. Increased resting tone of the platysma creates vertical bands (turkey neck) along the line of action and ‘venus rings’, that is horizontal banding, perpendicular to the line of action.
The tip of the nose becomes pulled down with time (pointed nose) and the descent of the midface, coupled with recession of the facial bones, deepens the nasolabial folds.
Treatment
Botulinum toxin causes a flaccid paralysis of muscles that have been injected and so induces a mild elongation as the muscle spindles stop contracting. This is particularly obvious in the vertical muscles of the face, for example in the upper lip. Almost all patients may successfully have their upper lip rhytids replaced with fresh smooth skin using CO 2 resurfacing, at different intensities and depths. Examine the patient carefully and consider the likely effect of elongating a perioral muscle before injecting it. If the patient already has a long nasal-vermilion distance, for example ( Fig. 10.3 A and B), then treating upper lip wrinkles with further relaxation of the muscle will not produce a good appearance. Treatment of the nasolabial fold will also lengthen the upper lip. These patients can be offered alternative treatments such as surgery, CO 2 resurfacing and fillers ( Fig. 10.4 A and B) (see Chapter 11 ).




Perioral indications
Upper lip rhytids
Lower lip rhytids
Pebbly chin
Elevation of lip corner
Reduction of nasolabial folds
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


