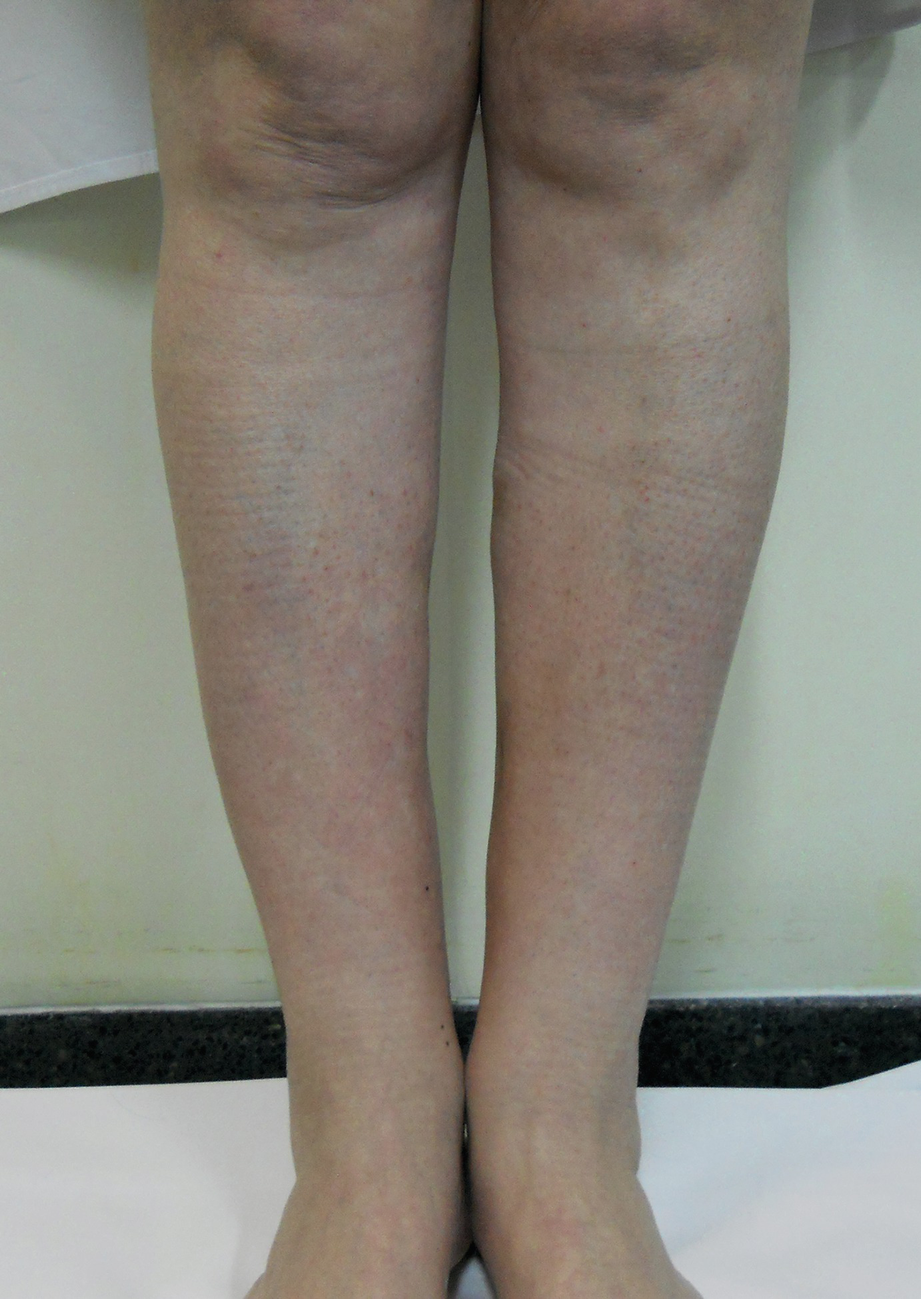
Indurations produced by injected paraffin in the calves

The indurated, rock-hard areas are marked for excision
Farmacological Treatments:
Oral corticosteroids
Minocycline
Tetracycline
Allopurinol
Tacrolimus
Etanercept
Imiquimod
There is currently no international consensus about which of these is the best medical treatment or about how long treatment should be continued. We refer readers back to Chap. 7, where we discussed the general therapeutic considerations that are most appropriate, along with a comprehensive review of diseases caused by the injection of silicone and other oils. The manifestations of disease produced by the injection of substances to modify body contour and the degree of tissue involvement are both so varied and their accurate evaluation so imprecise, that it is necessary to have a multidisciplinary team and a classification system to identify the stage of disease at which each patient presents, before treatment is initiated, so that their long-term prognosis can be estimated and the most appropriate treatment decisions made.
The clinical presentation, severity, and progression of disease must always be taken into account when trying to select the best treatment. For all patients, it is necessary to perform a histopathological and microbiological study to confirm the presence of granulomas and diagnose any possible infection, taking into account that the chronic evening fever characteristic of silicone-related disease may be due to common bacterial, fungi or even viral infections (see clinical case at the end of this chapter Figs. 8.4 and 8.5), even to atypical mycobacteria.
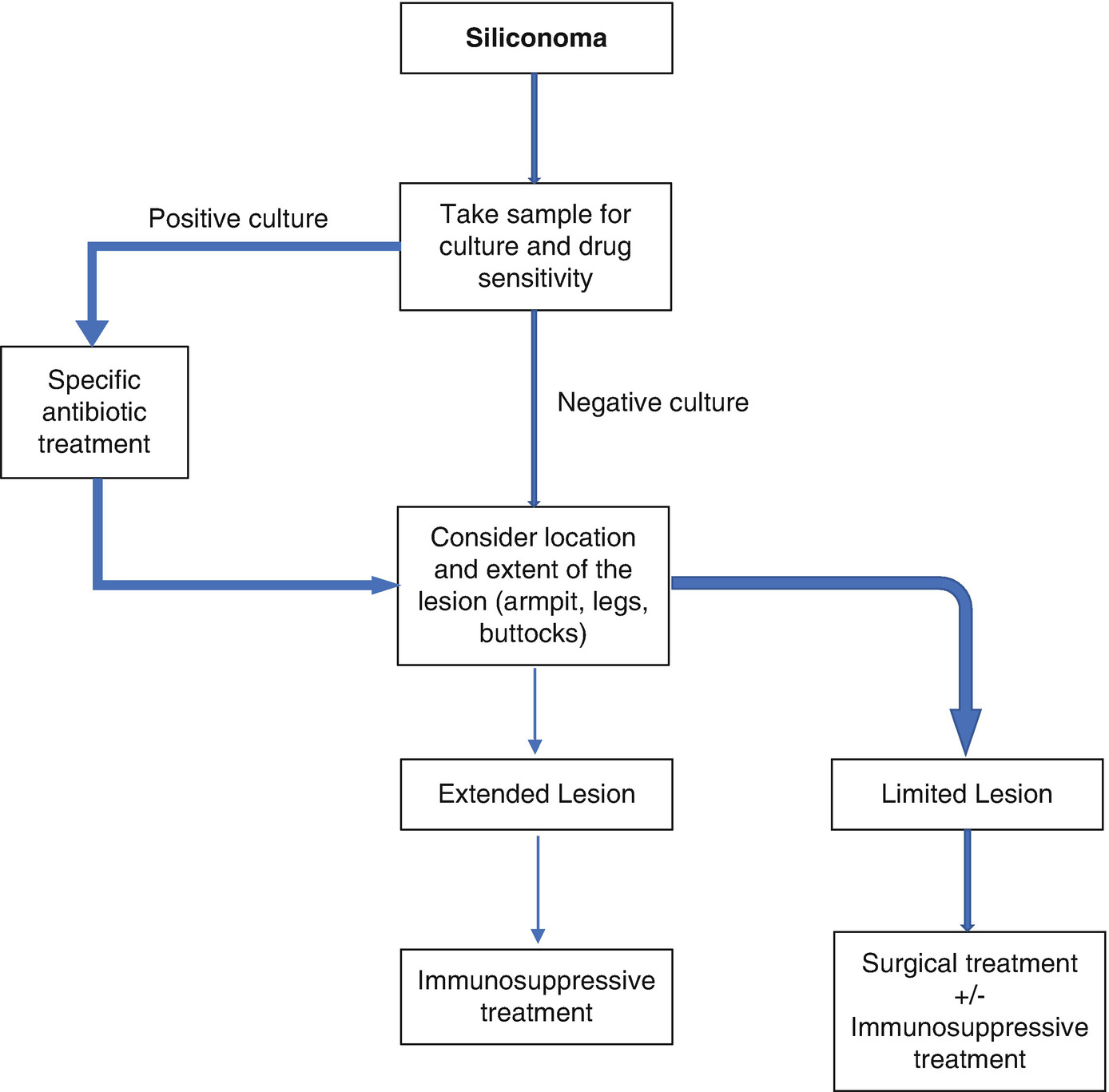
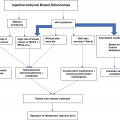
Therapeutic algorithm for siliconomas. First approach
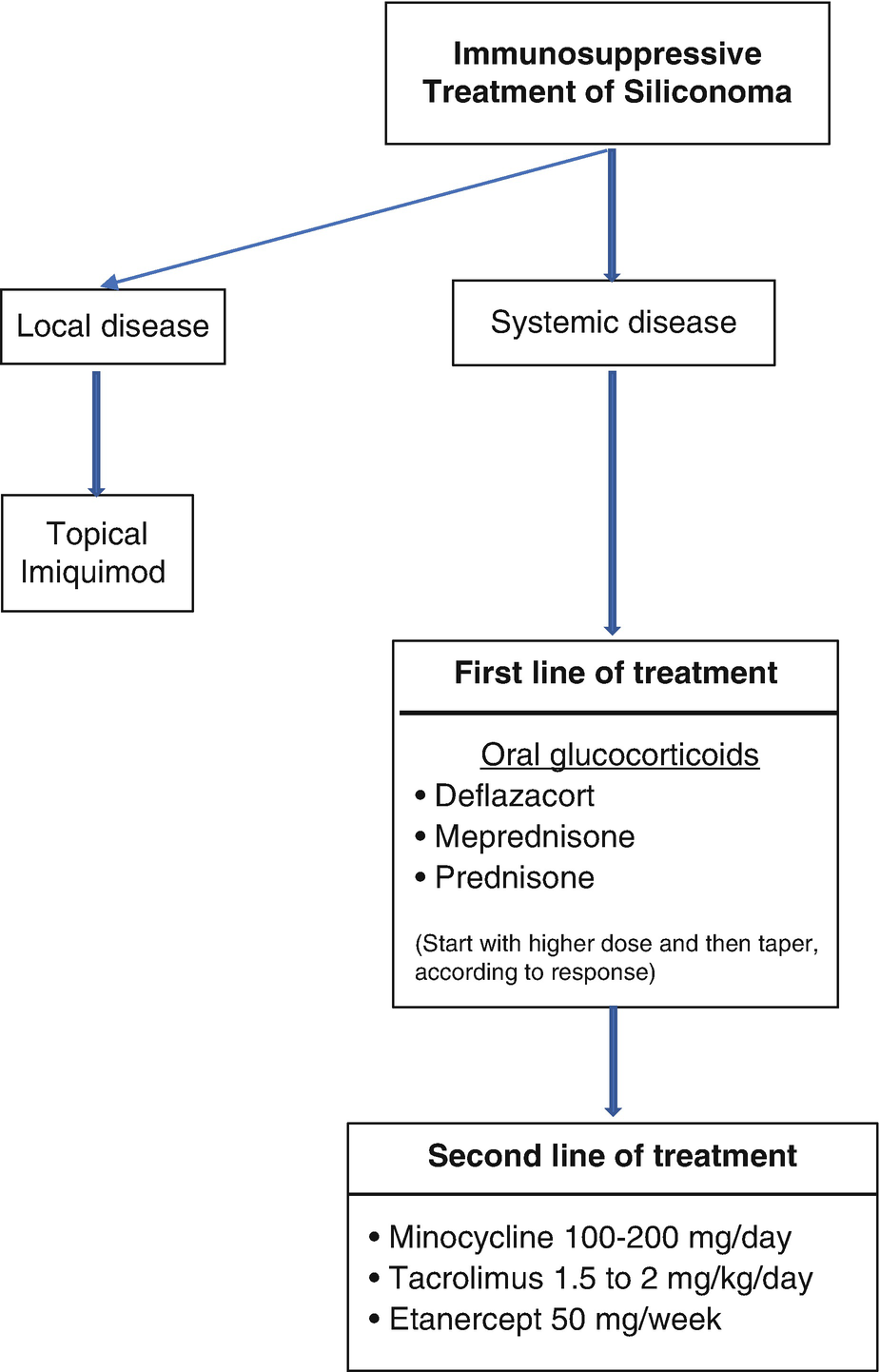
Therapeutic algorithm: immunosuppressive treatment of siliconomas
Oral Systemic Corticosteroids
Of all the pharmaceutical treatments listed above, the use of oral systemic corticosteroids has the greatest number of publications. However, there is no particular corticosteroid or dose recommended at this time.
A recent publication [1] described three patients in whom deflazacort was used. The first clinical case involved a 55-year-old woman with a 1-month lesion on her lower lip and a painless, progressively growing nasolabial groove. Silicone had been injected locally 9 years earlier. Treatment was started with deflazacort 15 mg/day, and the dose progressively decreased until it was withdrawn after 40 days of treatment.
The second case involved a woman with a lesion on her lower lip and an indurated chin, 1 month in duration, caused by the injection of silicones 16 years before. She was initially treated with 30 mg/day of deflazacort, a dose that was progressively reduced until it was discontinued after 1 month. However, the lesion worsened off steroids, so the same treatment was reinstated at an initial dose of 30 mg/day, which was gradually tapered to 7.5 mg/day for a total course of treatment of 10 months.
Finally, we describe the treatment of a 43-year-old woman who had had silicone injected into her lips and cheeks 10 years before. After 3 years, she developed an inflammatory lesion, with episodes of remission and exacerbation. She was treated surgically without improvement and started deflazacort treatment that she was told she should continue indefinitely. For all three patients, the author noted reduced inflammatory symptoms but persistent local induration on steroids.
Another publication [2] describes a 53-year-old woman who, after breast reconstruction with a silicone prosthesis, presented 5 years later with a clinical picture of anorexia, weight loss, and cervical lymphadenitis, caused by non-necrotizing granulomas. She was treated, with good results, using 3 mg/day of deflazacort on a permanent basis.
Another author [3] describes treatment administered to a 61-year-old woman, who had undergone silicone injection into the lower lip a few years earlier but then developed fevers, as well as erythematous, painful nodules on the chin and in the malar region. Initially she was treated with antibiotics (amoxicillin/clavulanate) with slight but transient improvement. She then experienced an excellent response to 0.5–1.0 mg/kg prednisone, though she continued to have occasional exacerbations of variable intensity.
In 2014, a paper was published describing the successful treatment of seven patients with different types of injury due to the injection of various substances, like silicone and paraffin. All were treated with 10–20 mg/ day of prednisone. The most severe cases also received triamcinolone subcutaneously, directly in the most evident nodules. Although these authors attributed success to these treatments, we consider injecting corticosteroids into nodules counterproductive, since they induce atrophy of the skin and fat, thereby intensifying the deformity and increasing the risk of fistulae.
Other authors [5] combined prednisone with limecycline (a type of tetracycline) for a 56-year-old patient who presented with a facial dermatosis, after having received an unknown filling material 9 years earlier. She was treated with 20 mg/day of prednisone, with a decreasing dose, and 150 mg of limecycline every 12 hours for 20 days and then 150 mg/day for 20 weeks. The size of the patient’s lesions gradually decreased.
Minocycline
One publication [6] describes the treatment provided to a 43-year-old patient with an extensive facial siliconoma, the product of the injection of silicone in the nasal region administered approximately 18 months before. The lesion produced severe and widespread deformation, mainly caused by fluctuating, erythematous nodules. Initially, the patient was treated with prednisone, but once diagnosed with glucose intolerance, possibly induced by corticosteroids, she was successfully treated with minocycline at a dose of 100 mg/day for 10 months. She experienced rapid improvement, including regression of the induration and erythema, which remained stable for a full year of follow-up. The authors justified the use of minocycline, by noting its anti-inflammatory and immunomodulatory effects.
A second, older publication [7] describes another two patients in whom minocycline was used successfully. The first was a 49-year-old patient with diffuse, erythematous, and indurated facial edema. She also had cervical lymphadenopathy. Eight years earlier, dimethyl siloxane oil had been administered. The first treatment given was prednisone at 1 mg/kg/day, but the patient developed glucose intolerance, so the dose of prednisone had to be decreased, and twice-daily minocycline 100 mg was added. Rapid improvement was observed, with complete resolution at 2 months. Prednisone was discontinued at 4 months, after which the patient was maintained on minocycline, 100 mg once daily.
The second patient was a 39-year-old woman who had had liquid silicone injected into her breast 5 years before. She developed indurated erythematous lesions and axillary adenopathy 2 months after the injections. Treatment was started with 100 mg of minocycline, twice daily, with improvement noted after 3 weeks.
Tetracycline
For tetracycline, we identified just two case reports.
The first [8] describes the clinical course of a 55-year-old transsexual patient, on antiretroviral treatment for HIV, who presented with extensive buttock lesions, which had evolved over 4 years. Seven years earlier, the patient had had a large volume (approximately 3 liters) of liquid silicone injected into the buttocks. Initially, the patient performed self-injections of subcutaneous triamcinolone into the lesions, but the improvement was minimal, and cutaneous atrophy had begun. When she consulted, she first underwent a biopsy and cultures that ruled out the presence of fungi, bacteria, and mycobacteria. She was then prescribed with minocycline, 100 mg/day, plus the combination of trimethoprim, 80 mg, and sulfamethoxazole, 400 mg, twice daily. For financial reasons, the patient was only able to purchase one of the medications and exhibited minimal improvement after 3 months of treatment. Since the latter was far cheaper, minocycline was changed to tetracycline, 500 mg, twice daily; and celecoxib, 200 mg, was added, twice per day. After the next 3 months, significant improvement was achieved. Then, again to accommodate the patient’s financial resources, tetracycline was changed to doxycycline, 100 mg, twice daily.
The decision to replace minocycline and trimethoprim-sulfamethoxazole with tetracycline and celecoxib was made based upon a previous publication [9], in which a patient with similar lesions was successfully treated with minocycline plus celecoxib after treatment with corticosteroids failed.
Allopurinol
Allopurinol is one of the treatments used for cutaneous sarcoidosis. Its mechanism of action for such lesions is poorly understood, though it is believed to inhibit the formation of multinuclear giant cells and, in this way, the formation of granulomas.
As examples of allopurinol’s use with siliconomas, we present three recent publications [10], the first involving a 62-year-old woman with painful nodules located on her eyelids, upper lip, and malar region. Liquid silicone had been administered 7 years previously. She was treated with allopurinol, 300 mg/day, with disappearance of the lesions over the following 2 months and no recurrence after 1 year.
The next case [11] is that of a 44-year-old woman with erythematous nodules of 9 months duration, who had been treated with intralesional triamcinolone repeatedly without improvement. Liquid silicone had been infiltrated in her thighs and legs 5 years before. Treatment with minocycline was started, 200 mg/day, but the patient only was able to afford it for the first month. It was replaced with allopurinol, 300 mg every 12 h. After 3 months, the patient had experienced a reduction in the number and size of her lesions, as well as marked improvement in her pain and erythema.
In another publication [12], a 56-year-old woman presented with firm nodules in the frontal region of her head. Treatment was initiated as allopurinol, 200 mg/day, which was increased to 300 mg/day after 4 weeks and this dose maintained for 3 months. After 8 weeks, improvement was observed in her lesions.
Tacrolimus
Tacrolimus is an immunosuppressant primarily used after allogeneic transplants, since it reduces the activity of T lymphocytes and interleukin 2. It is also used to treat severe dermatitis. One publication we found [13] reported seven patients with lesions caused by silicone injections. Prior to receiving tacrolimus, the patients had received an average of six different medical treatments for their siliconomas, with little response. All were treated with tacrolimus in a dose of 0.8–1.0 mg/kg twice daily, combined with prednisone 2.5–5 mg/day. After 18 months of treatment, five patients continued to exhibit excellent improvement in their lesions, especially nodules, plaques, angioedema, and panniculitis. Two patients had experienced total remission. Improvement initially was noticed within 2 weeks of commencing treatment.
Etanercept
Etanercept is a dimeric protein composed of two parts: one is a portion of human immunoglobulin and the other a receptor for tumor necrosis factor (TNF). The drug binds specifically to the latter, blocking and inhibiting it, thereby blocking the biochemical mechanisms that cause an inflammatory response. Some authors [14] claim that it may be an option for siliconomas when other treatments have failed. The recommended dose would be the same as that used for the treatment of rheumatoid arthritis: either 50 mg subcutaneous weekly or 25 mg twice weekly.
Imiquimod
Imiquimod is a molecule that acts as a ligand in 7 Toll-like receptors (TLR 7) in the innate immune system, where it induces local responses involving interferon α, β and γ, and tumor necrosis factor (TNF) α, as well as some interleukins. A single case report has been published documenting its satisfactory use in a patient with siliconomas [15].
Clinical Cases
We present the clinical case of a 38-year-old woman with no personal history of interest, who consulted us for very painful erythematous skin lesions, with indurated plaques, on both legs after she underwent paraffin injections to thicken her ankles (see Figs. 8.1 and 8.2). For approximately 4 years prior to seeing us, the patient had been receiving monthly intramuscular corticosteroid injections, but her lesions had persisted, limiting her mobility. She also had seen other physicians and surgeons in consultation, without receiving satisfactory answers.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


