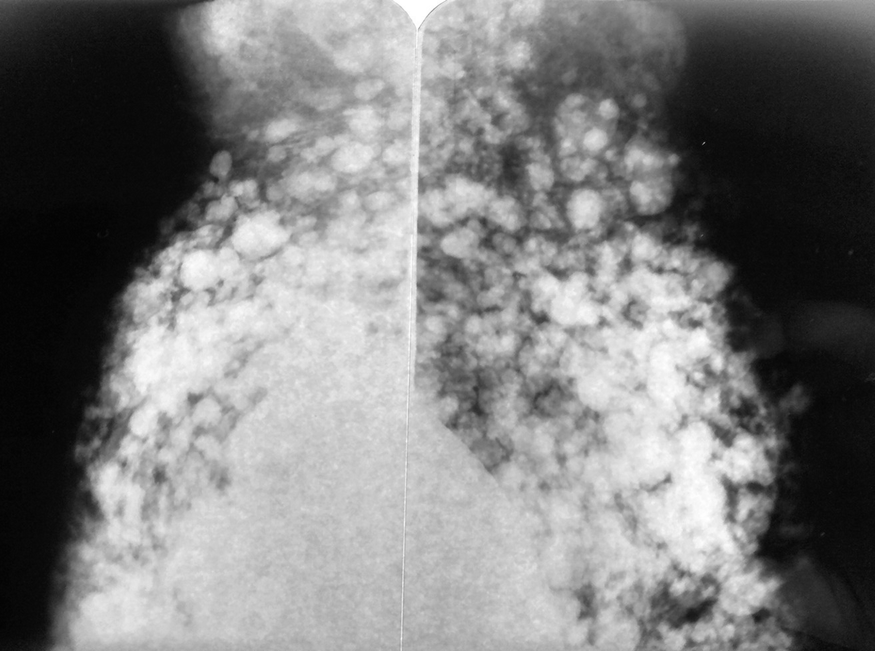
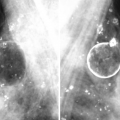
Silicones in the axilla. Mammography showing silicone in the axilla. Bilateral mammography is observed in an oblique view, in breasts with prosthetic implants from which there is abundant silicone that not only spread through the breast but also migrated to the axilla
Silicone in the axilla. Mammography showing more detail of the axillary region. Note that a large part of the axilla is filled with silicone
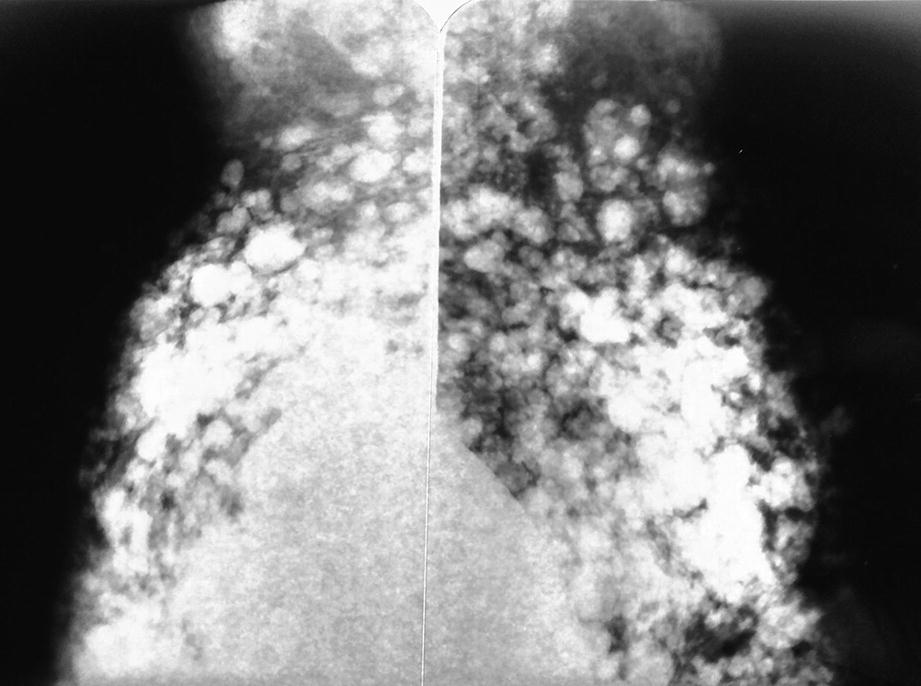
Silicone in the axilla. The lower axillary region is already affected by the migration of silicone
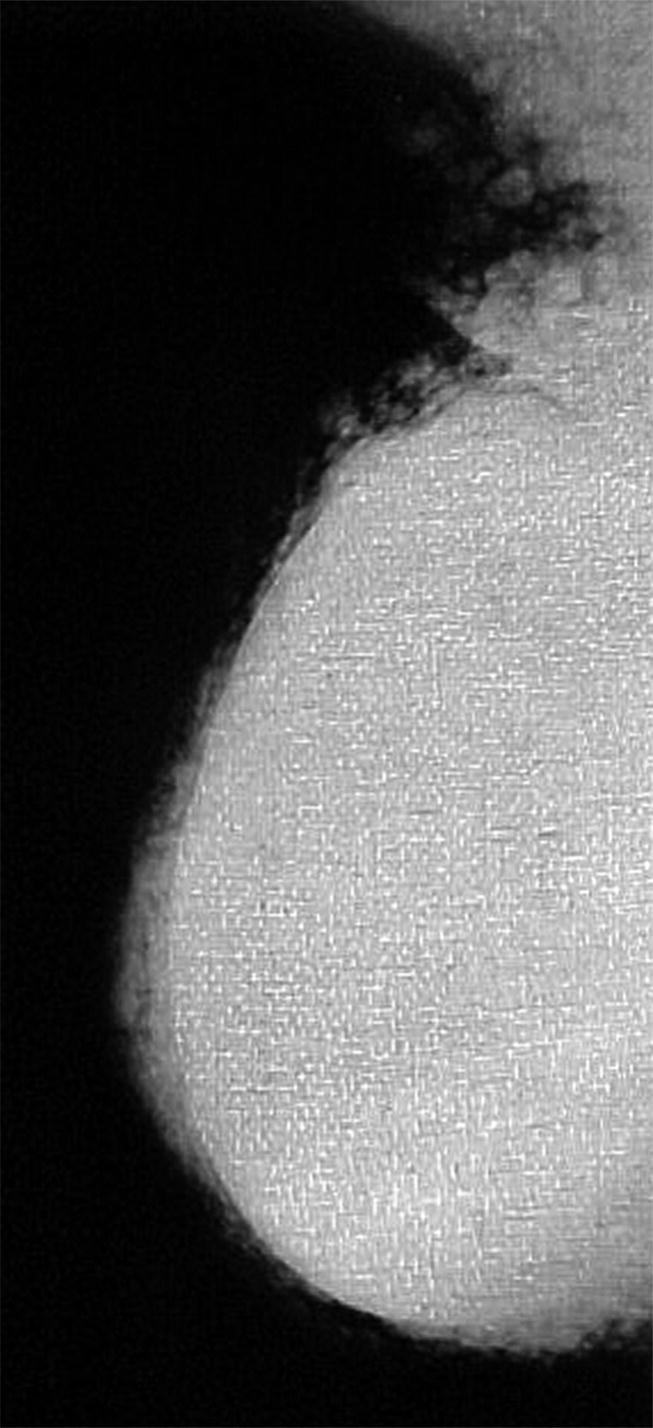
Silicone in the axilla. Mammogram where opacities are seen as a result of the past injection of silicone
The quantity of silicone is usually minimal, affecting no more than two or three lymph nodes. Any larger quantity of silicone or number of affected lymph nodes is usually accompanied by clinical symptoms when discovered.
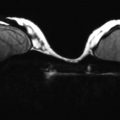
Ultrasound is also useful in these circumstances, typically revealing very dense images characterized by regular edges and a marked acoustic shadow; this has been called a “snowstorm” or “broken television” appearance.
The aforementioned methods are usually sufficient to make a diagnosis of axillary siliconomas. Magnetic resonance imaging, sestamibi-28 scintimammography, or 18F-FDG PET/CT can be used when there are doubts about the etiology of the axillary formation. As expressed by D’hulst, however, employing 18F-FDG PET/CT to identify reactive adenitis due to silicones in lymph nodes is not as specific as performing mammography. A percutaneous biopsy should always be considered when the potential presence of carcinoma metastases is still in doubt [30].
Pathology
Granulomatous Lymphadenopathy Due to Silicones
The migration of small silicone particles via the lymphatic route to lymph nodes can produce granulomatous lymphadenopathy [3, 31, 32]. The most frequently affected lymph nodes are axillary lymph nodes, but migration can also occur to other lymph node clusters, like supraclavicular and mediastinal nodes [33, 34]. Such adenopathy can occur in two clinical contexts: in a patient who has had a prosthesis implanted for purely aesthetic reasons; or in a patient whose prosthesis was implanted during postmastectomy breast reconstruction. In the latter situation, in addition to the patient’s natural anguish, there is the very real possibility that the adenopathy represents metastatic spread of a previously treated carcinoma.
Silicone lymphadenopathy can hinder the intraoperative study of the “sentinel node” in patients who previously had a prosthesis implanted for cosmetic reasons but then, over time, developed a carcinoma.
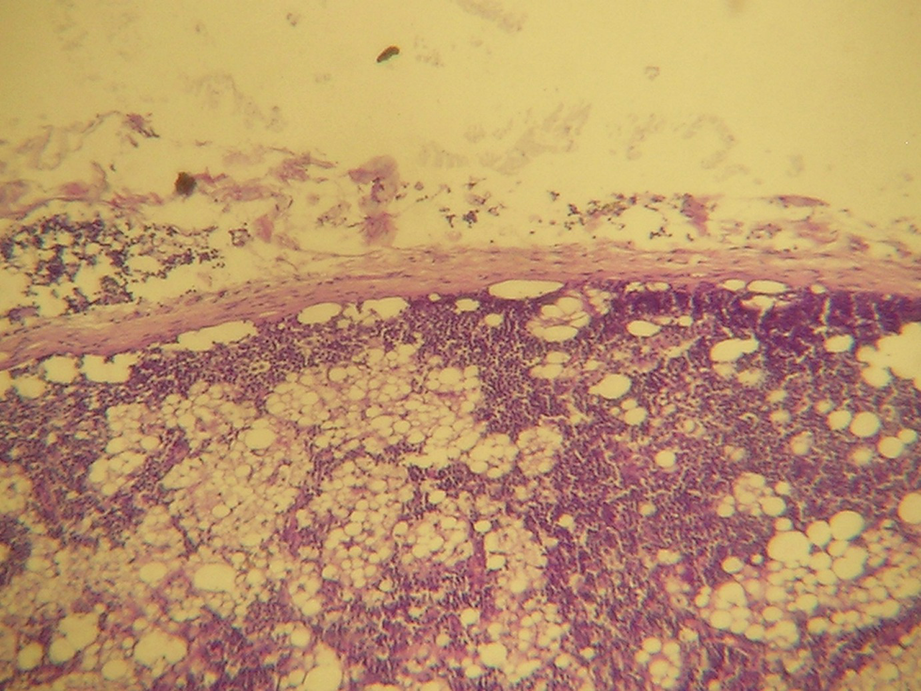
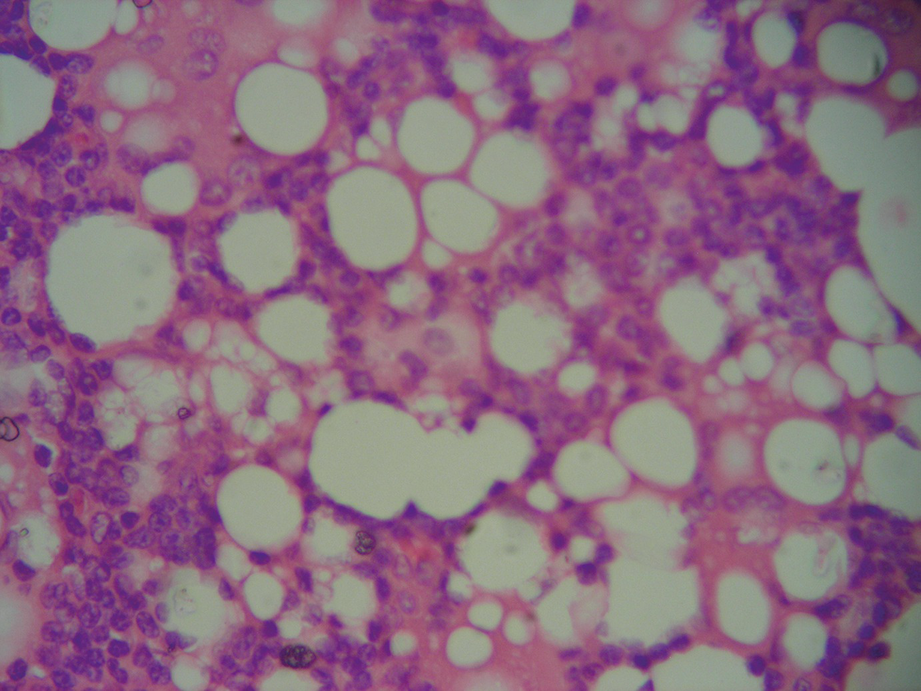
Silicone in the axilla. A lymph node with deposits of silicone and micro-vacuolated histiocytes in the lymphatic sinuses (100× magnification)
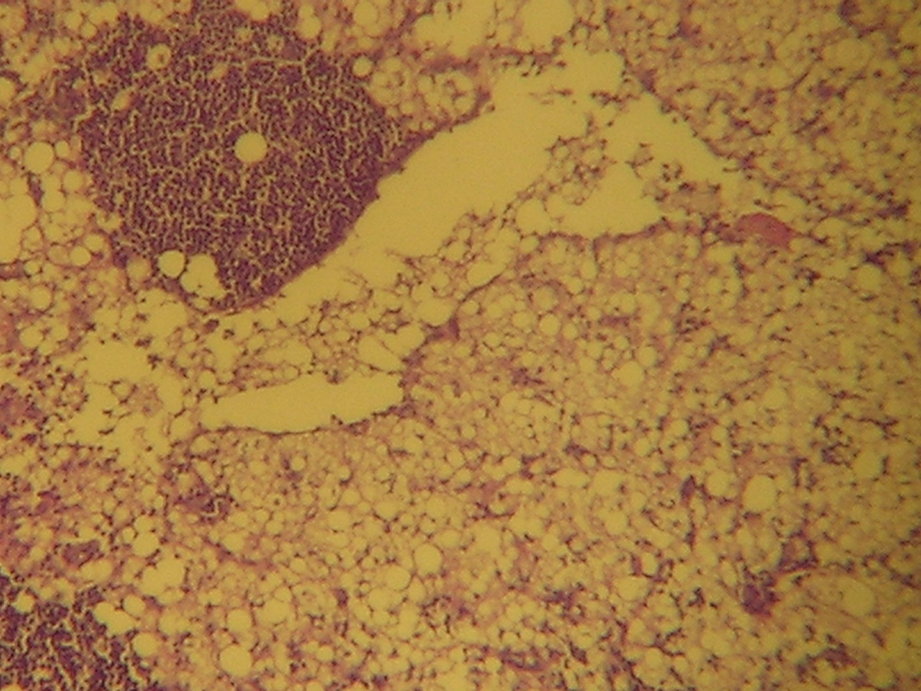
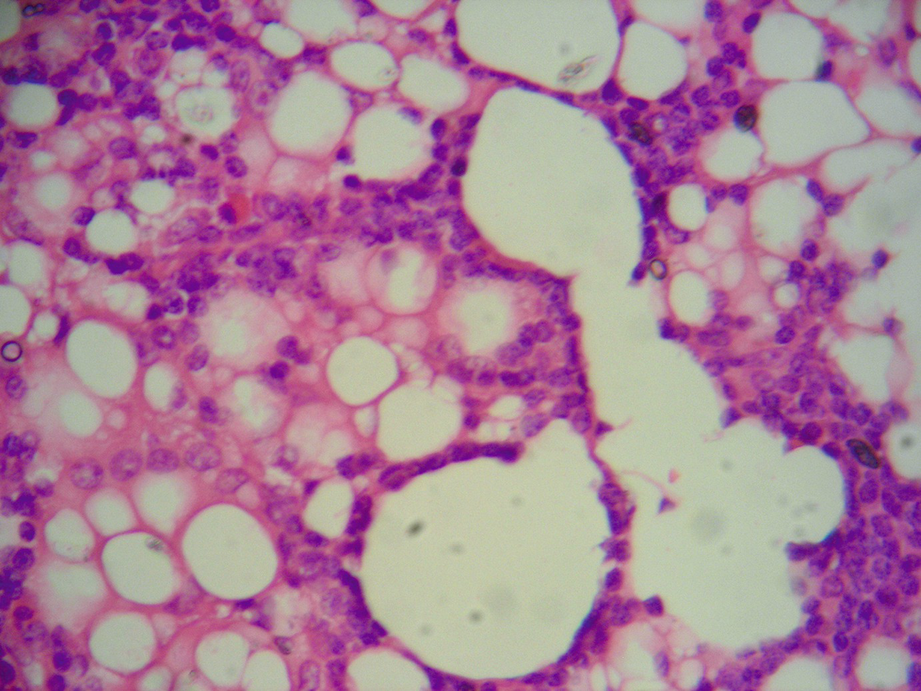
Silicone in the axilla. Dilated lymph node sinuses with silicone deposits and micro-vacuolated histiocytes (200× magnification)
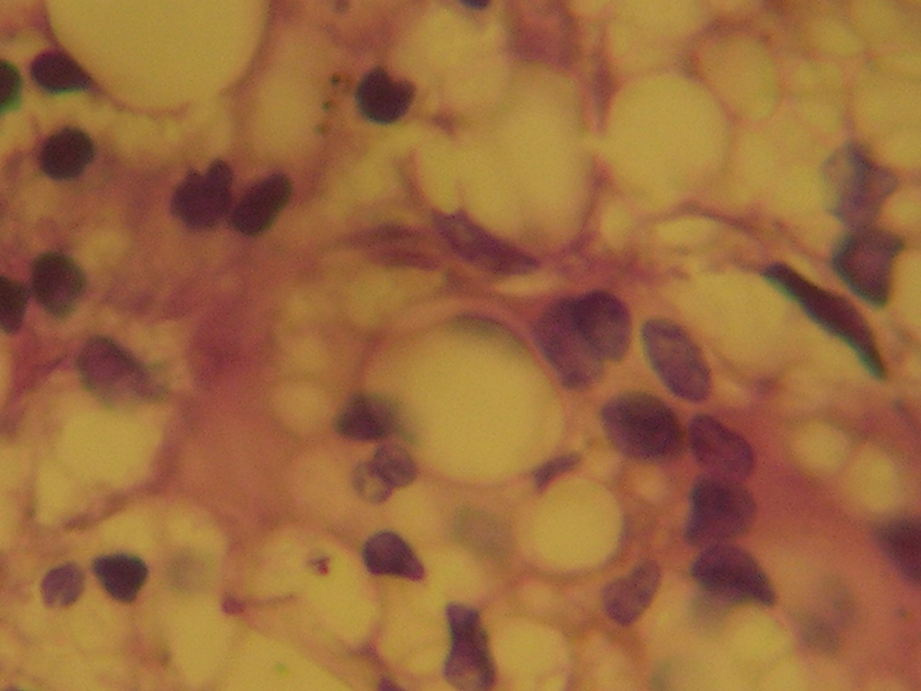
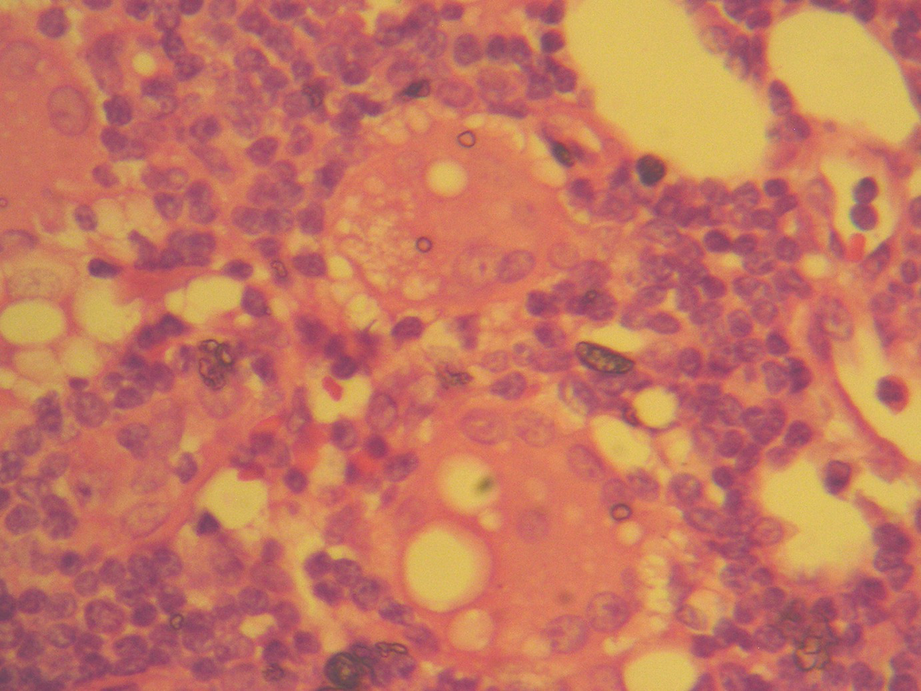
Silicone in the axilla. Silicone lumps and micro-vacuolated histiocytes in lymph nodes (450× magnification)
Silicone in the axilla. Silicone lumps in lymph nodes (450× magnification)
Axillary Lymphadenopathy Due to Silicones with Metastasis of Infiltrating Ductal Carcinoma
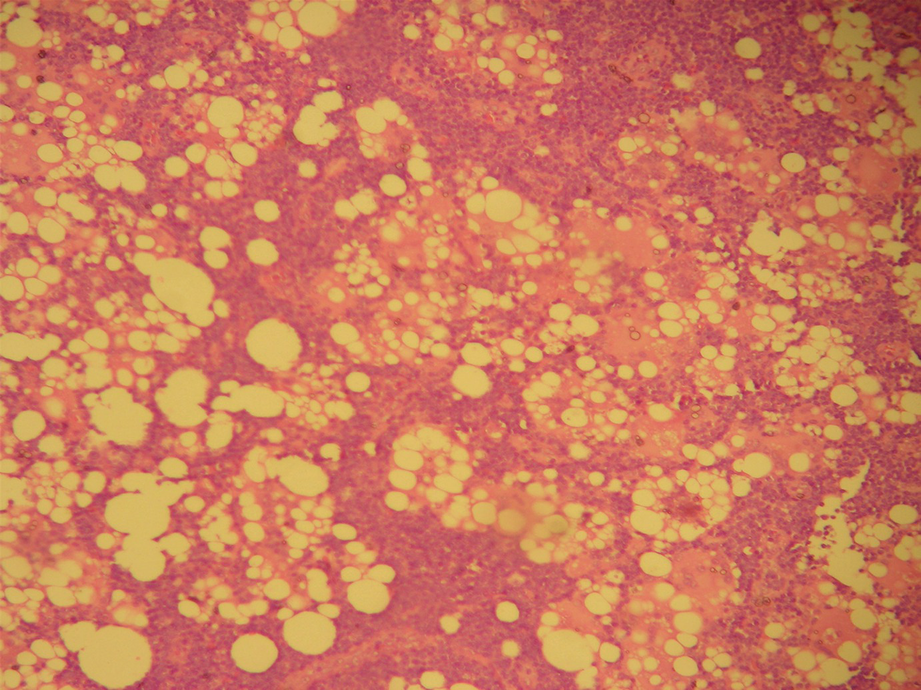
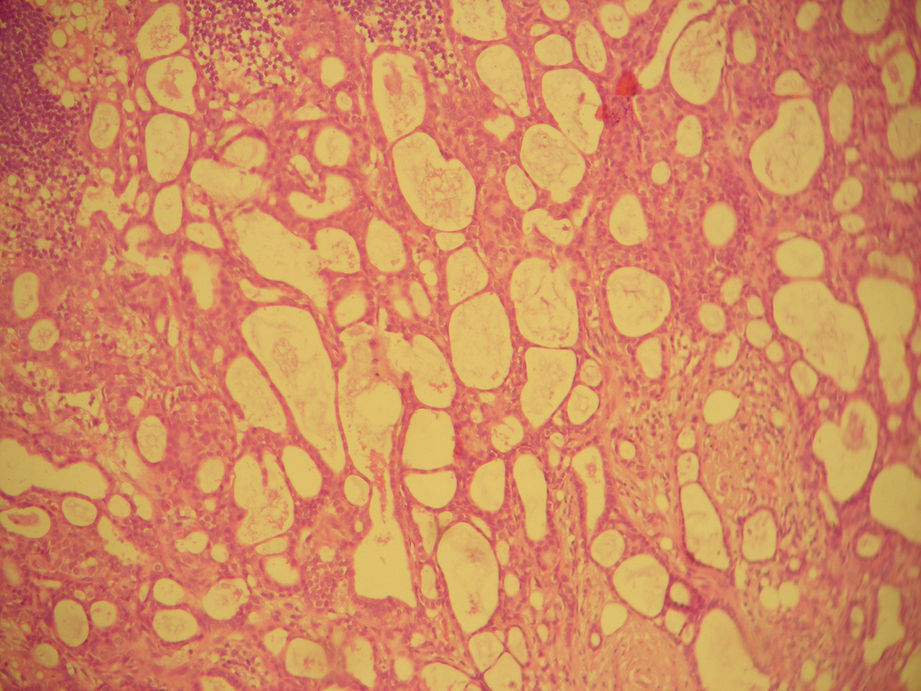
Silicone in the axilla. Axillary lymph node, post lymphadenectomy, in a patient with an infiltrating ductal carcinoma (NOS) and siliconoma in the breast. This field corresponds to an area of the lymph node without metastasis, but with silicone lymphadenopathy; the clear spaces of different diameter in the lymphatic sinuses have clumps of silicone and some isolated multinucleated giant cells (100× magnification)
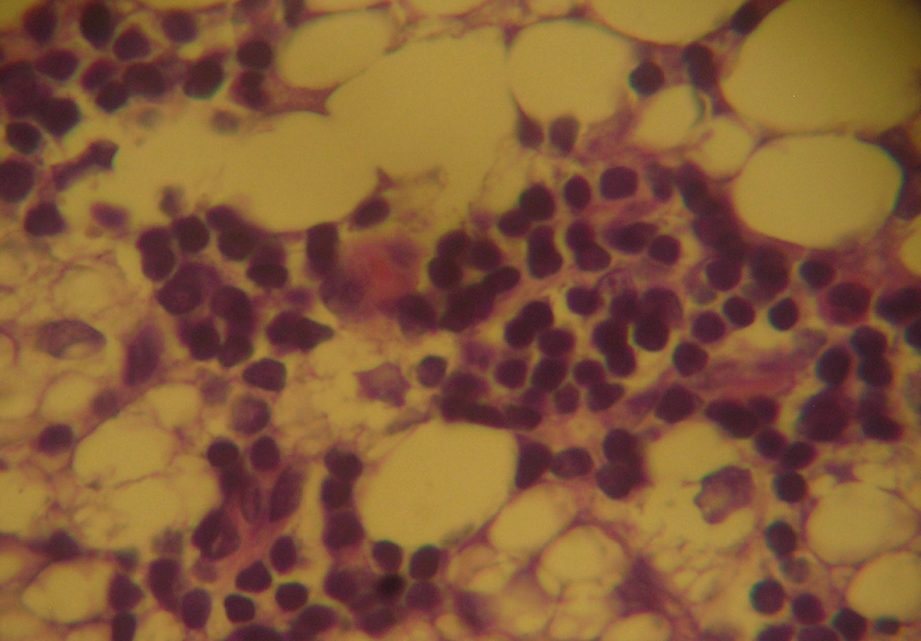
Silicone in the axilla. Similar to Fig. 14.9, at higher magnification (450× magnification)
Silicone in the axilla. Similar to Fig. 14.9, at higher magnification (450× magnification)

Silicone in the axilla. Giant multinucleated cell with vacuoles of silicone of different diameter in the cytoplasm (450× magnification)
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


