Trapezius Muscle and Musculocutaneous Flaps
K. F. HAGAN
S. J. MATHES
EDITORIAL COMMENT
The editors caution the reader to use this flap only when the transverse cervical artery is known to be intact. The transverse cervical artery often is ablated during a radical neck dissection; therefore, the major source of blood supply to the flap is interrupted.
The trapezius muscle is the basis for muscle and musculocutaneous flaps that are of great usefulness in reconstructing defects of the head and neck and of the upper back (1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12). Its location makes it frequently the flap of choice for defects of the occipital, parotid, and cervical spine areas. In addition, it may be used for intraoral and anterior neck coverage. The posterior trapezius musculocutaneous flap should be considered the flap of choice for defects of the lateral face, posterior scalp and neck, and the upper third of the posterior trunk.
ANATOMY
Muscle Function
The muscle may be functionally separated into three parts (Fig. 133.1). The upper occipital and cervical part acts to elevate the shoulder, holding it in normal postural position by slight, continuous, tonic contraction. This action is not shared with other muscles (although the levator scapulae exerts an upward pull on the scapula, it does not have the same effect on the shoulder girdle), and hence denervation of the trapezius or functional loss of its upper fibers will result in the shoulder-drop deformity (13, 14).
The medial fibers, originating from the upper thoracic region, pull the scapula backward toward the midline and act to square the shoulders. This function is shared with the rhomboid muscles.
The inferior fibers from the lower thoracic region act in concert with the upper fibers to rotate the scapula, assisting in abduction of the arm above the horizontal plane; however, loss of function of lower fibers alone usually has minimal effect on arm abduction because the serratus anterior is a more powerful rotator of the scapula than the trapezius. Therefore, selective loss of the middle and inferior fibers has no significant clinical sequelae (see Fig. 133.1).
The trapezius is a broad, flat, triangular-shaped muscle that, when combined with its contralateral mate, forms a trapezium (see Fig. 133.1). It originates medially from the external occipital protuberance, the medial part of the superior nuchal line of the occipital bone, the ligamentum nuchae, and the spinous processes of the seventh cervical and all the thoracic vertebrae. The superior portion of the muscle that originates from the occipital and upper thoracic areas inserts into the posterior aspect of the lateral third of the clavicle
(Figs. 133.1 and 133.2). The middle portion, originating from the lower cervical and upper thoracic areas, inserts onto the acromion and the superior spine of the scapula. The inferior fibers, originating from the lower thoracic vertebrae, insert into the base of the spine of the scapula. The muscle overlies the splenius capitis, levator scapulae, supraspinatus, rhomboidus minor and major, and the upper medial portion of the latissimus dorsi muscle.
(Figs. 133.1 and 133.2). The middle portion, originating from the lower cervical and upper thoracic areas, inserts onto the acromion and the superior spine of the scapula. The inferior fibers, originating from the lower thoracic vertebrae, insert into the base of the spine of the scapula. The muscle overlies the splenius capitis, levator scapulae, supraspinatus, rhomboidus minor and major, and the upper medial portion of the latissimus dorsi muscle.
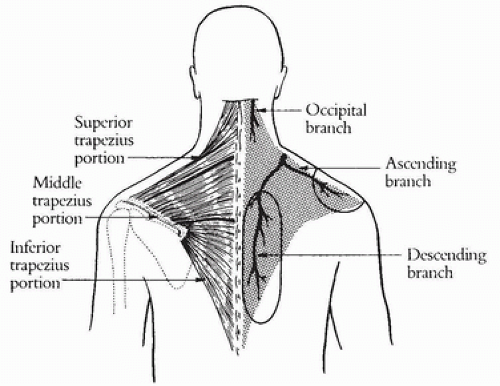 FIGURE 133.1 Trapezius anatomy. The relationship of the three functional portions of the trapezius muscle to the vascular supply to the trapezius is demonstrated. The location of the anterior and posterior skin islands is shown. |
The vascular supply consists of a dominant pedicle and several minor pedicles (Figs. 133.1, 133.2, 133.3B). The dominant blood supply originates from the transverse cervical artery and vein, a branch of the subclavian artery or thyrocervical trunk and associated veins. This vascular pedicle courses between the sternocleidomastoid and the scalenus muscles, crosses the anterior margin of the trapezius, and enters the deep surface of the muscle at the base of the neck. It then divides into ascending and descending branches that are the basis for the separate superior and inferior musculocutaneous flaps. The descending branch courses along the deep surface of the muscle, between the spine and the scapulae, supplying musculocutaneous perforators to the overlying skin. The ascending branch, which may occasionally arise as a separate branch from the thyrocervical trunk, courses laterally on the deep surface of the superior portion of the muscle, giving perforating vessels to the overlying skin just posterior to the clavicle. The average length of this dominant pedicle is 4 cm, with an average diameter of 1.8 mm.
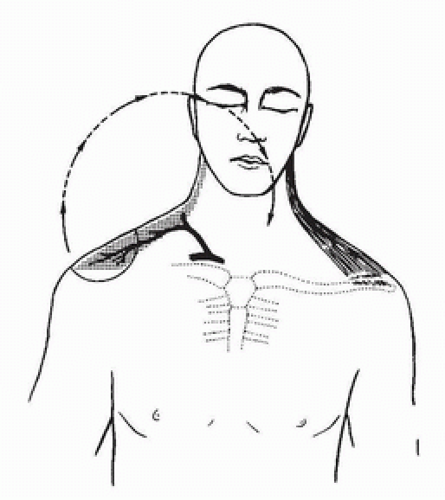 FIGURE 133.2 Trapezius muscle, anterior view. The anterior portion is inserted into the clavicle. The anterior skin island flap, based on the anterior branch of the transverse cervical artery, is illustrated with its arc of rotation. |
Several minor pedicles also supply this muscle. The largest of these is a branch of the occipital artery (which arises from the external carotid). It supplies the superomedial portion of the muscle (see Fig. 133.1). This branch is the basis for McCraw’s technique for augmenting the Mutter flap with the upper portion of the trapezius (9). It is approximately 3 cm long and 1 mm in diameter.
The remaining minor pedicles consist of perforating branches of the posterior intercostal arteries and veins that enter the muscle along the midline adjacent to the cervical and thoracic vertebral bodies. These are 1 to 2 cm in length and 0.5 mm in diameter.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


