Introduction
The trapezius muscle, with its unique triangular shape and great length, extends from the occiput down to the 12th thoracic vertebra and consists of descending, transverse, and ascending parts; its complexity renders a systematic description challenging. Since the upper trapezius myocutaneous flap was first published by McCraw et al. and Demergasso and Piazza in 1979 and the lower trapezius myocutaneous flap by Baek et al. and Mathes and Nahai in 1980, the pedicled trapezius flap has been a standard procedure in head and neck reconstruction. In 1981, the trapezius muscle was classified as a type II pattern of circulation (one dominant vascular pedicle plus minor pedicles) according to Mathes and Nahai.
Since then, different opinions on the vascular anatomy of all flap modifications have led to confusion and technical problems during flap harvesting. To avoid any misunderstandings in flap planning and elevation, all flaps related to the trapezius discussed below are defined by their supplying arteries.
Regional Anatomy ( Figs 39.1–39.4 and Fig 11.1 , Fig 11.4 , Fig 11.7 )
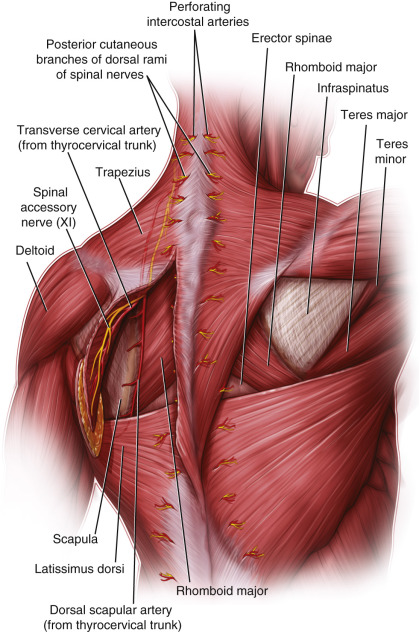
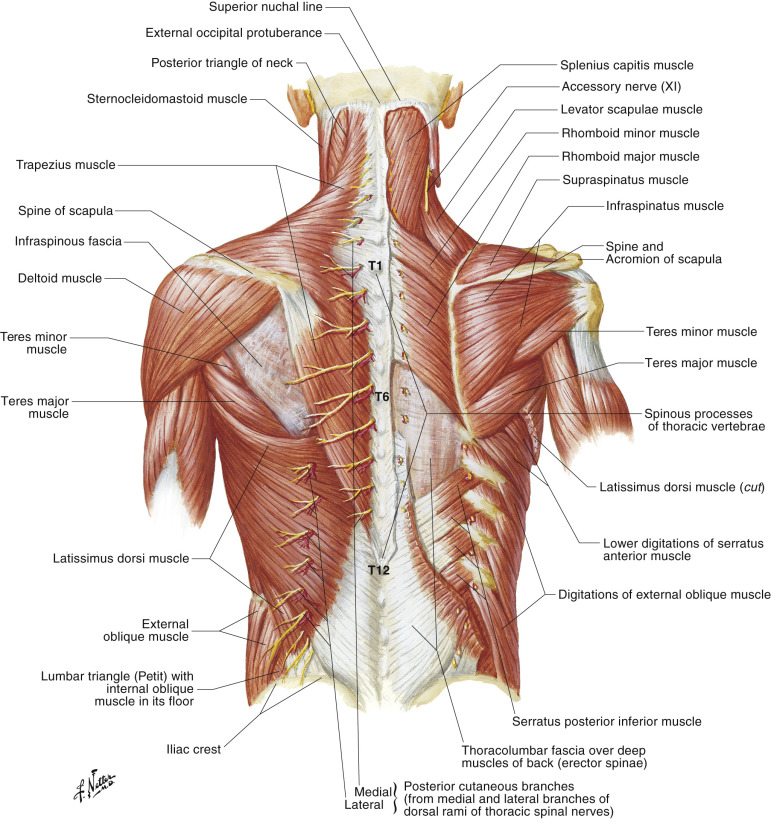
The trapezius muscle is the most superficial muscle on the posterior aspect of the neck and thorax. The underlying layer is composed of the levator scapulae, the major and minor rhomboid muscles, and the latissimus dorsi below the 7th thoracic vertebra.

The trapezius is divided into three parts: the descending or superior part, the transverse or middle part, and the ascending or inferior part. The descending (superior) part originates at the external occipital protuberance, the superior nuchal line, and the nuchal ligament down to the spinous process of C7 and inserts into the lateral third of the clavicle. This part mainly acts to elevate the scapula. The transverse (middle) part originates at the spinous processes of the 1st–5th thoracic vertebrae and inserts into the acromion. This part mainly acts to retract the scapula. The ascending (inferior) part is attached proximally to the spinous processes of the 6th–12th thoracic vertebrae and inserts into the spine of the scapula. This part mainly acts to depress the scapula.
Only the transverse (middle) part (= upper trapezius flap) and the ascending (inferior) part (= lower trapezius flap) of the trapezius are widely used in reconstructive surgery.
The anatomy of the underlying muscles is important for harvesting trapezius flaps.
- •
The levator scapulae muscle originates from the transverse processes of the 1st–4th cervical vertebrae and inserts into the superior angle of the scapula. It supports the function of the descending (superior) part of the trapezius in elevating the scapula.
- •
The rhomboid minor muscle originates from the spinous processes of the 6th and 7th cervical vertebrae and inserts into the medial border of the scapula above the spine of the scapula. It supports the function of the trapezius in retracting and elevating the scapula.
- •
The rhomboid major muscle originates from the spinous processes of the 1st–4th thoracic vertebrae and inserts into the medial border of the scapula below the spine of the scapula. Similar to the rhomboid minor, it supports the function of the trapezius in retracting and elevating the scapula.
Arterial Anatomy of the Region ( Figs 39.1–39.4 and Fig. 11.7 )
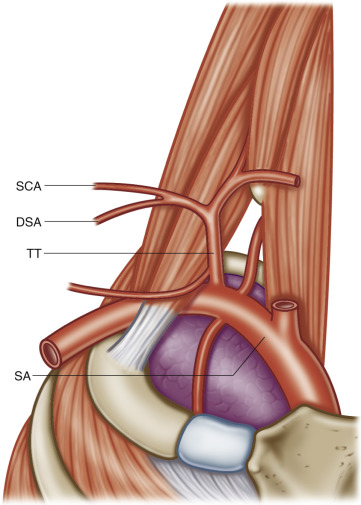
The posterior muscles of the neck are mainly supplied by arteries branching off the subclavian artery either directly or indirectly via the thyrocervical trunk. Only the descending (superior) part of the trapezius is supplied by branches of the occipital artery, which is the largest posterior branch of the external carotid artery. The surgically more important parts of the trapezius are supplied by two either direct or indirect branches of the subclavian artery. The complicated vascular anatomy and the difficult and often misused vascular terminology have caused problems in the planning and harvesting of trapezius flaps. For this reason, special emphasis is placed here on the vascular supply of the transverse (middle) part (= upper trapezius flap) and the ascending (inferior) part (= lower trapezius flap) of the trapezius muscle. The transverse (middle) part of the trapezius is supplied by the superficial cervical artery (SCA; superficial branch of the transverse cervical artery). The ascending (inferior) part of the trapezius is supplied by the dorsal scapular artery (DSA; deep branch of the transverse cervical artery). Minor intercostal perforators add to the blood supply of the most inferior part of the trapezius.
The SCA arises from a common trunk with the dorsal scapular artery in 30% (in these cases forming the transverse cervical artery) with a superficial (superficial cervical artery) and a deep branch (dorsal scapular artery), with the suprascapular artery in 22% or with both the dorsal scapular and the suprascapular arteries in 24%. These trunks may be branches of the thyrocervical trunk in the great majority of the cases or of the subclavian artery. In the remaining 24%, the superficial cervical artery arises independently from either the thyrocervical trunk (22%) or the subclavian artery (2%). The SCA usually has an ascending and a descending branch. In any case, the artery lies deep to the trapezius muscle and superficial to the levator scapulae and rhomboids.
The DSA arises from a common trunk with the superficial cervical artery in 30% (see above) or the suprascapular artery (4%), or with both the dorsal scapular and the suprascapular arteries in 24%. In the remaining 42%, it originates directly from the subclavian artery (37%), the thyrocervical trunk (1%), the internal thoracic artery (1%), or the costocervical trunk (3%). In cases in which the dorsal scapular artery is a direct or indirect branch of the subclavian artery, it pierces through the brachial plexus. In any case, the DSA lies deep to the levator scapulae and rhomboids. In between the minor and major rhomboid, it always gives rise to the branch to the ascending (inferior) part of the trapezius (trapezius branch of the dorsal scapular artery). The DSA terminates in a descending branch under the rhomboid major muscle.
Venous Anatomy of the Region
In general, the arteries in the neck are accompanied by two veins. These venae comitantes drain into a large vein crossing the neck horizontally, the so-called “transverse cervical vein.” This main collector of the neck drains into the venous angle.
The veins of the trapezius muscle accompany the arteries until they cross the anterior border of the muscle. Then, their courses differ from those of the arteries and form one (55%), two (42%), or more (3%) so-called transverse cervical veins. In the majority of cases, these veins pass the brachial plexus laterally and terminate in the external jugular vein (80%). In the remainder, they terminate in the subclavian vein (12%) or in both the external jugular and the subclavian vein (8%).
Nerves in the Region ( Figs 39.1, 39.3, 39.4 and Fig. 11.7 )
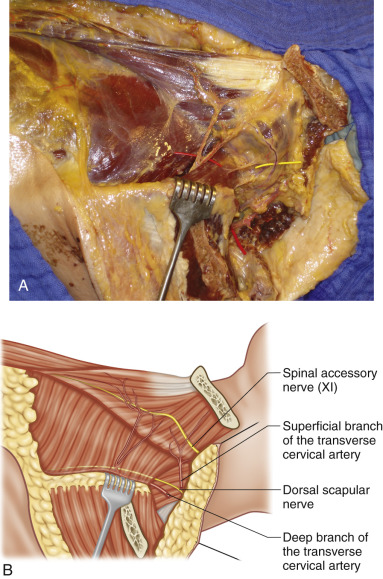
The trapezius muscle is supplied by the spinal accessory nerve (11th cranial nerve). It also receives proprioceptor fibers via a branch of the cervical plexus. The spinal accessory nerve (11th cranial nerve) crosses superficial to the SCA in 60% and deep in 33%. In the remaining 7%, one artery runs superficial and one deep to the nerve. The nerve accompanies the SCA superiorly and the trapezius branch of the DSA inferiorly. The levator scapulae and the rhomboids are supplied by the dorsal scapular nerve (DSN) from the brachial plexus. The dorsal scapular nerve pierces through the middle scalene muscle and runs deep to levator scapulae and the rhomboids, thus accompanying the descending branch of the DSA.
Flap Anatomy ( Figs 39.1–39.7 and Fig. 11.7 )
With the complex vascular supply of the whole trapezius muscle and the surrounding area, any classification or description of flap types is difficult. Mathes and Nahai stated that the trapezius muscle has one dominant (descending/deep branch of the transverse cervical artery or, respectively, the dorsal scapular artery) pedicle and some minor vascular pedicles (type II). According to our findings from hundreds of cadavers and those of most other authors, there are at least two dominant pedicles (the SCA and the DSA) and some minor pedicles (the occipital artery and the intercostal perforators) with respect to the whole muscle. In practice, the whole muscle is never harvested as one flap, so, as such, this is not relevant to reconstructive surgery. The various flaps utilize only parts of the trapezius muscle, as a vessel carrier.
The clearest and most logical way to classify flaps is to define them by their vascular pedicle. A subdivision into upper or lower flaps is no longer necessary, and categorizing them into vertical or transverse flaps, according to the skin island, does not lead to misunderstandings.
According to the vascular supply of the trapezius muscle, a trapezius flap can be elevated on four different pedicles and we refer to them here as four types:
- •
Type 1 . A trapezius flap based on the occipital artery. This usually includes the superior descending part of the muscle and a transverse skin island.
- •
Type 2 . A trapezius flap based on the SCA (superficial branch of the transverse cervical artery). Parts of the middle transverse fibers (upper flap) of the muscle are included. The skin island may be planned to be transverse or vertical. The flap can be harvested as myocutaneous or osteomyocutaneous (including a part of the scapular spine; Fig. 39.6 ) based on the ascending branch, or as a myocutaneous flap based on the descending branch of the SCA.
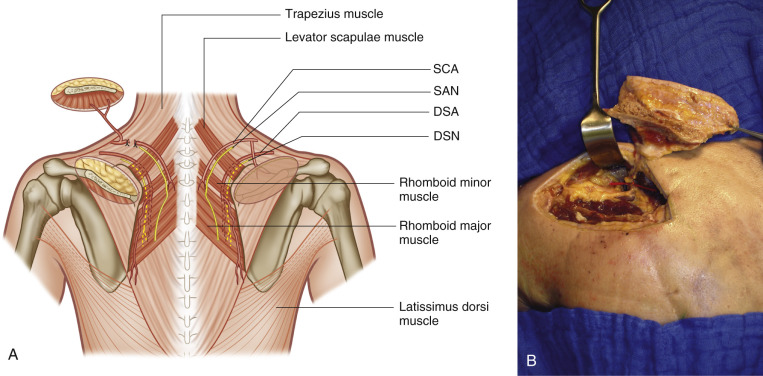
Figure 39.6
Elevated osteomyocutaneous flap based on the ascending branch of the superficial scapular artery. (A) Schematic drawing: SCA, superficial cervical artery; SAN, spinal accessory nerve; DSA, dorsal scapular artery; DSN, dorsal scapular nerve. (B) Cadaver dissections.
- •
Type 3 . A trapezius flap based on the DSA (deep branch of the transverse cervical artery). Parts of the inferior ascending (lower flap) fibers are included ( Fig. 39.7 ). The skin island is planned to be vertical in a myocutaneous flap or the muscle is elevated without skin.
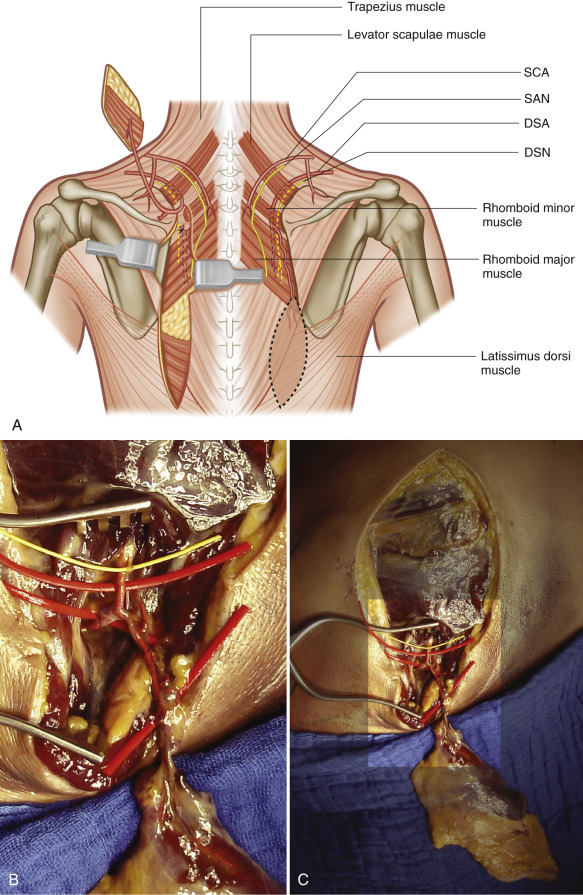
Figure 39.7
Elevated myocutaneous flap based on the dorsal scapular artery. (A) Schematic drawing: SCA, superficial cervical artery; SAN, spinal accessory nerve; DSA, dorsal scapular artery; DSN, dorsal scapular nerve. (B) Cadaver dissections.
- •
Type 4 . A trapezius muscle flap based on the intercostal arteries in a turnover technique.
In some publications it is not clear whether more than one pedicle artery is included (DSA and SCA or SCA and occipital artery) to ensure vascularization. If an island flap is correctly prepared, there is no need to include two arteries and a large muscle cuff. When the flap is elevated this way, most of the muscle function or the accessory nerve itself will be sacrificed.
The trapezius muscle plays two important roles in shoulder function: stabilizing and moving the scapula on the one hand and elevating the shoulder on the other. It is of the utmost importance to preserve as much function as possible to minimize donor site morbidity. Careful dissection and elevation as an island flap are essential.
Myocutaneous perforators, except those from the intercostal arteries, are extremely thin and rare, so that, in our opinion, perforator flaps cannot be recommended. The donor site should always be closed directly. Skin grafts in the shoulder region, especially over the acromion and the spine of the scapula, can lead to deforming scars and functional problems.
Flap elevation based on the SCA or on the DSA (arterial supply classification types 2 and 3 as described above) is useful in clinical practice, and so it is given particular attention in the following description.
The myocutaneous flap based on the occipital artery (arterial supply type 1), as first published by McCraw, is rarely indicated in the era of microsurgical procedures. Disadvantages such as time loss, very bulky tissue, and a donor site that is difficult to close directly prevented it from becoming a standard procedure.
A turnover muscle flap of the ascending (lower) part (arterial supply type 4) needs further clinical evaluation. Our anatomic investigations showed constant intercostal perforators, mostly around the fifth and sixth intercostal spaces, which should allow defect coverage of the middle and lower part of the thoracic spine and even the upper part of the lumbar spine.
Arterial Supply of the Flap ( Figs 39.1 and 39.2 and Fig. 11.7 )
The lower trapezius muscle can be classified as a type V muscle according to Mathes and Nahai, having one dominant pedicle and secondary segmental vascular pedicles. The lengths of the feeding vessels (SCA, intercostal arteries, DSA) given below are not the pedicle lengths, but the lengths of the dominant vessels until they divide into the first branches.
Trapezius Flap Based on the SCA
Dominant:
superficial branch of the transverse cervical artery
Length: 4.7 cm (range 4.5–4.9 cm)
Diameter: 4.0 mm (range 3.8–4.2 mm)
The SCA divides into a descending (inferior) branch and an ascending (superior) branch. The descending branch runs medial to the scapula and superficial to the levator scapulae muscle and the rhomboid muscles. The descending branch is accompanied by the spinal accessory nerve. The ascending branch runs down to the spine of the scapula.
Minor:
posterior intercostal arteries
Length: 3.1 cm (range 1.7–4.5 cm)
Diameter: 0.7 mm (range 0.5-0.9 mm)
Our cadaver dissections showed constant intercostal arteries supplying the lower part of the trapezius muscle between the third and sixth intercostal spaces. To our knowledge, there is very little clinical experience with flaps based on intercostal branches. We also see rare indications to perform these flaps in a turnover procedure to cover defects in the lower and middle part of the thoracic spine.
In any case, as described by Ogawa et al. when large pedicled flaps based on the SCA or even DSA are created, microvascular augmentation can be helpful when an anastomosis is created between the recipient site and the intercostal perforators.
Trapezius Flap Based on the DSA
Dominant:
deep branch of the transverse scapular artery
Length: 5.83 cm (range 5.20–6.46 cm)
Diameter: 3.3 mm (range 2.95–3.65 mm)
This branch runs deep to the levator scapulae and the minor rhomboid muscles. The flap-feeding vessel (trapezius branch) appears between the minor and major rhomboid muscles, and lies deep to the trapezius and superficial to the rhomboid major muscle.
Minor Pedicles:
posterior intercostal arteries
Minor pedicles of the ascending (lower) part of the trapezius muscle constantly branch off from the dorsal intercostal vessels from the third to the sixth intercostal spaces.
The lower trapezius muscle can be classified as a type V muscle according to Mathes and Nahai, having one dominant pedicle and secondary segmental vascular pedicles.
Variation of Arterial Origin ( Fig. 39.5 , Table 39.1 )
Frequent changes in the anatomic nomenclature of the arteries in the posterior cervical triangle (lateral cervical region), coupled with lack of knowledge of the gross anatomy and incorrect use of the nomenclature of these arteries, have presented difficulties in musculocutaneous flap planning. In particular, the term “transverse cervical artery” (A. transversa colli, cervicis) and its associated branches (the superficial branch, superficial cervical artery; and the deep branch, dorsal scapular artery) have been used frequently over the past several decades with different meanings.
| SCA | DSA | SSA | |
|---|---|---|---|
| Origin from a vessel | |||
| Thyrocervical trunk | 22 | 37 | 12 |
| Subclavian artery | 2 | 1 | 27 |
| Internal thoracic artery | 0 | 1 | 11 |
| Costocervical trunk | 0 | 3 | 0 |
| Origin from a trunk | |||
| Cervico-dorsal trunk (30%) | |||
| Thyrocervical trunk | 16 | 16 | – |
| Subclavian artery | 13 | 13 | – |
| Internal thoracic artery | 1 | 1 | – |
| Cervico-scapular trunk (22%) | |||
| Thyrocervical trunk | 17 | – | 17 |
| Subclavian artery | 3 | – | 3 |
| Internal thoracic artery | 2 | – | 2 |
| Dorsoscapular trunk (4%) | |||
| Thyrocervical trunk | – | 3 | 3 |
| Subclavian artery | – | 1 | 1 |
| Cervico-dorsoscapular trunk (24%) | |||
| Thyrocervical trunk | 20 | 20 | 20 |
| Subclavian artery | 3 | 3 | 3 |
| Internal thoracic artery | 1 | 1 | 1 |
An investigation of these arteries in 498 sides of necks showed the following results. The superficial cervical artery, the dorsal scapular artery, and the suprascapular artery arose from the subclavian artery either as direct branches or from trunks. A cervico-dorsal trunk gave origin to the superficial cervical and dorsal scapular arteries, a cervico-scapular trunk gave rise to the superficial cervical and suprascapular arteries, a dorsoscapular trunk provided origins for the dorsal scapular and suprascapular, and a cervico-dorsoscapular trunk gave origin to the superficial cervical artery, the dorsal scapular artery, and the suprascapular artery. Each of these trunks, in turn, arose from either the subclavian artery or the thyrocervical trunk.
The superficial cervical artery supplies the middle (transverse) part of the trapezius and travels with the accessory nerve. It is a direct branch from either the thyrocervical trunk (22%) or the subclavian artery (2%). More commonly, the superficial cervical artery arises from trunks, i.e. cervico-dorsal trunk (30%), cervico-scapular trunk (22%), or cervico-dorsoscapular trunk (24%).
The dorsal scapular artery supplies the lower (ascending) part of the trapezius and travels with the dorsal scapular nerve. It is a direct branch from the subclavian artery (37%), the thyrocervical trunk (1%), the internal thoracic artery (1%), or the costocervical trunk (3%). More commonly, the dorsal scapular artery arises from trunks, i.e. cervico-dorsal trunk (30%), dorsoscapular trunk (4%), or cervico-dorsoscapular trunk (24%).
The suprascapular artery supplies the supra- and infraspinatus muscles and travels with the suprascapular nerve. It is a direct branch from the subclavian artery (12%), the thyrocervical trunk (27%), or the internal thoracic artery (11%). The suprascapular artery arises from trunks, including the cervico-scapular trunk (22%), the dorsoscapular trunk (4%), and the cervico-dorsoscapular trunk (24%).
This labeling convention necessitates omitting the term “transverse cervical artery,” since this term has been misleading and misused over the years, and, even if used in its genuine sense, this artery is found in the minority of cases.
The anatomic findings proved a constant blood supply of the lower trapezius muscle via the dorsal scapular artery as the main vessel, regardless of the origin of this artery. However, the arc of rotation of the lower trapezius flap changes depending on the origin of its artery.
Venous Drainage of the Flap
Trapezius Flaps Based on the SCA and the DSA
Primary:
the usually double accompanying veins are slightly larger in diameter and of the same length as the respective artery.
The termination is in the transverse cervical vein, which eventually drains into the venous angle. Proximally, at the level of the anterior border of the trapezius muscle, the veins generally run separate from the arteries. They can build a single vein, two veins, or rarely three, all of which are called transverse cervical veins, and they can drain into different systems (external cervical vein, subclavian vein, or both) in the posterior triangle of the neck. This variability is only important for the pedicled flap based on the SCA, because the course of the veins and their relationship to the brachial plexus and the accessory nerve can limit their arc of rotation.
Flap Innervation ( Figs 39.1, 39.3, 39.4 and Fig. 11.7 )
Sensory:
trapezius flap based on the SCA
It is possible to preserve partial innervation of the skin island using acromial branches of the cervical plexus.
Sensory:
Trapezius flap based on the DSA
No axial sensory nerve is available for this flap, but to recover some sensibility, if necessary, it could be possible to include one or more posterior cutaneous branches of intercostal nerves in the skin island.
There is no useful way to restore sensibility by including a sensory nerve in a flap based on the DSA.
Motor:
spinal accessory nerve (cranial nerve XI)
The trapezius flaps are not suitable for functional muscle reconstruction because of their central role in shoulder function. Harvesting the whole muscle would cause unacceptable donor site morbidity. It is of greatest importance to elevate the flap (including a part of the muscle) in such a way as to preserve as much function as possible.
Flap Components
Trapezius Flap Based on the SCA
The trapezius flap based on the SCA is usually harvested as a myocutaneous flap. If needed, a segment of the scapular spine (10 × 2 cm) can be included for an osteomyocutaneous flap. To avoid shoulder instability, at least 2 cm of the acromion (lateral part) should be left intact. When a skin island is not indicated, the muscle alone can be transferred.
Trapezius Flap Based on the DSA
The trapezius flap based on the DSA is usually indicated as a myocutaneous flap. In rare cases, a muscle flap without skin can be performed.
Advantages
Trapezius Flap Based on the SCA
- •
The pedicled myocutaneous trapezius flap based on the SCA provides a fast and easy procedure to reconstruct defects of the hypopharynx, oropharynx, and upper esophagus.
- •
The island flap is thin and pliable with a limited arc of rotation according to the anatomic situation.
- •
The flap, transferred as an osteomyocutaneous flap, is an alternative to free tissue transfer for reconstruction of combined defects. After ablative surgery, the mandible and the floor of the mouth can be reconstructed.
- •
The donor site of the flap is in the same operative field and often, especially after neck dissection, the vascular pedicle has already been dissected.
- •
Short operating time, acceptable donor site morbidity (preserved accessory nerve and primary closure), and minimal bulk contribute to a good result.
Trapezius Flap Based on the DSA
- •
The myocutaneous island flap is a reliable, thin, and pliable flap, allowing a wide arc of rotation.
- •
It is especially suitable for problematic ipsi- or contralateral defects in the occipital and dorsal neck region and over the thoracic spine, which this flap can cover without microsurgery.
- •
For soft tissue defects in the lower face and anterior neck, it is also a good alternative to other flaps, and the donor site morbidity is low.
- •
A free flap based on the DSA can be dissected with a very long pedicle.
Disadvantages
Trapezius Flap Based on the SCA
- •
In one-third of individuals, the accessory nerve passes between the pedicle artery and vein, so that one vessel has to be severed and restored, or the accessory nerve has to be sacrificed or divided and sutured.
- •
The upper part of the trapezius muscle (descending and middle part) has to be divided during pedicle dissection.
- •
The wide variability of the draining veins limits a reliable flap transfer.
- •
The bone segment should not exceed 10 × 2 cm to ensure vascularization, which limits the indication to smaller bone defects.
Trapezius Flap Based on the DSA
- •
Elevation of the island flap can be technically challenging because of the small diameter of the peripheral pedicle vessels and their course close to the medial border of the scapula.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


